Evaluation of a Sustained-Release Formulation of Buprenorphine for Analgesia in Rats
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Cellular and Genetic Bases of Cold Nociception and Nociceptive Sensitization in Drosophila Larvae
The Texas Medical Center Library DigitalCommons@TMC The University of Texas MD Anderson Cancer Center UTHealth Graduate School of The University of Texas MD Anderson Cancer Biomedical Sciences Dissertations and Theses Center UTHealth Graduate School of (Open Access) Biomedical Sciences 12-2016 Cellular and genetic bases of cold nociception and nociceptive sensitization in Drosophila larvae Heather N. Turner Follow this and additional works at: https://digitalcommons.library.tmc.edu/utgsbs_dissertations Part of the Molecular and Cellular Neuroscience Commons Recommended Citation Turner, Heather N., "Cellular and genetic bases of cold nociception and nociceptive sensitization in Drosophila larvae" (2016). The University of Texas MD Anderson Cancer Center UTHealth Graduate School of Biomedical Sciences Dissertations and Theses (Open Access). 714. https://digitalcommons.library.tmc.edu/utgsbs_dissertations/714 This Dissertation (PhD) is brought to you for free and open access by the The University of Texas MD Anderson Cancer Center UTHealth Graduate School of Biomedical Sciences at DigitalCommons@TMC. It has been accepted for inclusion in The University of Texas MD Anderson Cancer Center UTHealth Graduate School of Biomedical Sciences Dissertations and Theses (Open Access) by an authorized administrator of DigitalCommons@TMC. For more information, please contact [email protected]. CELLULAR AND GENETIC BASES OF COLD NOCICEPTION AND NOCICEPTIVE SENSITIZATION IN DROSOPHILA LARVAE by Heather Nicole Turner, B.S. APPROVED: _________________________ -

Operant Nociception in Nonhuman Primates ⇑ Brian D
PAINÒ 155 (2014) 1821–1828 www.elsevier.com/locate/pain Operant nociception in nonhuman primates ⇑ Brian D. Kangas , Jack Bergman Harvard Medical School, McLean Hospital, Belmont, MA, USA Sponsorships or competing interests that may be relevant to content are disclosed at the end of this article. article info abstract Article history: The effective management of pain is a longstanding public health concern. Morphine-like opioids have Received 22 April 2014 long been front-line analgesics, but produce undesirable side effects that can limit their application. Slow Received in revised form 10 June 2014 progress in the introduction of novel improved medications for pain management over the last 5 decades Accepted 16 June 2014 has prompted a call for innovative translational research, including new preclinical assays. Most current in vivo procedures (eg, tail flick, hot plate, warm water tail withdrawal) assay the effects of nociceptive stimuli on simple spinal reflexes or unconditioned behavioral reactions. However, clinical treatment Keywords: goals may include the restoration of previous behavioral activities, which can be limited by medica- Nociception assay tion-related side effects that are not measured in such procedures. The present studies describe an appa- Operant behavior Thermal pull ratus and procedure to study the disruptive effects of nociceptive stimuli on voluntary behavior in l-Opioids nonhuman primates, and the ability of drugs to restore such behavior through their analgesic actions. Opioid efficacy Squirrel monkeys were trained to pull a cylindrical thermode for access to a highly palatable food. Next, NOP agonists sessions were conducted in which the temperature of the thermode was increased stepwise until Squirrel monkey responding stopped, permitting the determination of stable nociceptive thresholds. -

The Role of Substance P in Opioid Induced Reward
The Role of Substance P in Opioid Induced Reward Item Type text; Electronic Dissertation Authors Sandweiss, Alexander Jordan Publisher The University of Arizona. Rights Copyright © is held by the author. Digital access to this material is made possible by the University Libraries, University of Arizona. Further transmission, reproduction or presentation (such as public display or performance) of protected items is prohibited except with permission of the author. Download date 02/10/2021 14:53:26 Link to Item http://hdl.handle.net/10150/621568 THE ROLE OF SUBSTANCE P IN OPIOID INDUCED REWARD by Alexander J. Sandweiss __________________________ Copyright © Alexander J. Sandweiss 2016 A Dissertation Submitted to the Faculty of the DEPARTMENT OF PHARMACOLOGY In Partial Fulfillment of the Requirements For the Degree of DOCTOR OF PHILOSOPHY In the Graduate College THE UNIVERSITY OF ARIZONA 2016 1 THE UNIVERSITY OF ARIZONA GRADUATE COLLEGE As members of the Dissertation Committee, we certify that we have read the dissertation prepared by Alexander J. Sandweiss, titled The Role of Substance P in Opioid Induced Reward and recommend that it be accepted as fulfilling the dissertation requirement for the Degree of Doctor of Philosophy. _______________________________________________________________ Date: June 13, 2016 Edward D. French, Ph.D. _______________________________________________________________ Date: June 13, 2016 Rajesh Khanna, Ph.D. _______________________________________________________________ Date: June 13, 2016 Victor H. Hruby, Ph.D. _______________________________________________________________ Date: June 13, 2016 Naomi Rance, M.D., Ph.D. _______________________________________________________________ Date: June 13, 2016 Todd W. Vanderah, Ph.D. Final approval and acceptance of this dissertation is contingent upon the candidate’s submission of the final copies of the dissertation to the Graduate College. -

Central Targeting of Trigeminal Primary Afferent Nerve Terminals Via Intracisternal Injection of Rtx and Its Effect on Pain Behavior
CENTRAL TARGETING OF TRIGEMINAL PRIMARY AFFERENT NERVE TERMINALS VIA INTRACISTERNAL INJECTION OF RTX AND ITS EFFECT ON PAIN BEHAVIOR By MELANIE M. WEXEL A THESIS PRESENTED TO THE GRADUATE SCHOOL OF THE UNIVERSITY OF FLORIDA IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF MASTER OF SCIENCE UNIVERSITY OF FLORIDA 2008 1 © 2008 Melanie M. Wexel 2 To my Mom, for inspiring me to continue education 3 ACKNOWLEDGMENTS I thank my committee chair (John Neubert, DDS, PhD) and my committee members (Robert Caudle, PhD and Calegero Dolce, DDS, PhD). I would also like to thank Heather Rossi, Alan Jenkins, Jean Kaufman, and Wendi Malphurs for assisting with the laboratory experiments. Also, I would like to acknowledge the NIH grant #R21 DE16704-01A1 and the Southern Association of Orthodontics grant for financial support. 4 TABLE OF CONTENTS page ACKNOWLEDGMENTS ...............................................................................................................4 LIST OF FIGURES .........................................................................................................................6 LIST OF ABBREVIATIONS..........................................................................................................7 ABSTRACT.....................................................................................................................................8 CHAPTER 1 INTRODUCTION ....................................................................................................................9 Background...............................................................................................................................9 -

Virtual Proposals: Studying the Effects of Age on Pain Perception In
The Journal of Biological Sciences Virtual Proposals: Studying the effects of age on pain perception in Drosophila melanogaster Jenny Pan, Taylor O’Rourke, Meghan Wachira, Manpreet Kaur, Ubaidah Khan Department of Biology, Rutgers University, Camden, N.J. 08102 Abstract of this paper, the elderly are defined as individuals 65 and Pain is described as an unpleasant sensory and emotional older. It is projected by the United States Census that by 2030, experience correlated with tissue damage. Pain can manifest nearly 20 percent of the US population will represent the itself into several forms such as acute and chronic. While elderly. As the elderly population grows, the percentage of aging is often accompanied with pain, little is known about chronic pain patients in this population will increase. how the aging process impacts each. Currently, there are However, a significant number of individuals that experience conflicting studies on how pain sensitivity changes over a chronic pain may go unidentified by medical professionals. lifetime. Various studies suggest that pain perception Chronic pain in elderly individuals is often not detected, decreases as an individual ages, while opposing studies leading to a lack of treatment of chronic pain states in these suggest that pain perception increases with age. Our study individuals (Kaye et al., 2010). In a geriatric nursing home, uses thermally induced noxious stimuli to test pain among researchers found that 66% of the residents dealt with various age-groups in Drosophila melanogaster. The short chronic pain, yet 34% of the cases were undetected by life span of D. melanogaster allows for age-related research to be conducted. -

A Genetic Screen for Wnt Signaling Factors That Regulate Drosophila Melanogaster Nociception
A GENETIC SCREEN FOR WNT SIGNALING FACTORS THAT REGULATE DROSOPHILA MELANOGASTER NOCICEPTION A Thesis By PAUL RICHARD FREEMAN Submitted to the Graduate School At Appalachian State University in partial fulfillment of the requirements for the degree of MASTER OF SCIENCE May 2017 Department of Biology A GENETIC SCREEN FOR WNT SIGNALING FACTORS THAT REGULATE DROSOPHILA MELANOGASTER NOCICEPTION A Thesis By PAUL RICHARD FREEMAN May 2017 APPROVED BY: ______________________________________ Dr. Andrew Bellemer Chairperson, Thesis Committee ______________________________________ Dr. Ece Karatan Member, Thesis Committee ______________________________________ Dr. Cortney Bouldin Member, Thesis Committee ______________________________________ Dr. Zack Murrell Chairperson, Department of Biology ______________________________________ Dr. Max C. Poole Dean, Research Graduate Studies Copyright by Paul Richard Freeman All Rights Reserved Abstract A GENETIC SCREEN FOR WNT SIGNALING FACTORS THAT REGULATE DROSOPHILA MELANOGASTER NOCICEPTION Paul Richard Freeman B.S., University of North Carolina at Pembroke M.S., Appalachian State University Chairperson: Dr. Andrew Bellemer The mechanisms that regulate the transduction of noxious stimuli and generation of appropriate behavioral responses in Drosophila melanogaster are not fully understood. In larvae, Class IV multidendritic neurons are highly branched sensory neurons that are responsible for detecting noxious chemical, thermal, or mechanical stimuli and generating appropriate behavioral responses. Recent studies have demonstrated involvement of Wnt signaling in regulating nociception and the development of chronic pain in vertebrate models, but the underlying cellular and molecular mechanisms are still not understood. In order to better understand the roles of Wnt signaling in Drosophila nociception, I have selected 53 Wnt signaling-related genes and obtained UAS-RNAi lines for each from the Drosophila TRIP collection for an RNAi screen for nociception defects. -

Pain in Flies
NIH Public Access Author Manuscript Dev Dyn. Author manuscript; available in PMC 2012 January 16. NIH-PA Author ManuscriptPublished NIH-PA Author Manuscript in final edited NIH-PA Author Manuscript form as: Dev Dyn. 2012 January ; 241(1): 16±26. doi:10.1002/dvdy.22737. Pokes, Sunburn, and Hot Sauce: Drosophila as an Emerging Model for the Biology of Nociception Seol Hee Im1 and Michael J. Galko1,2,3,* 1Department of Biochemistry and Molecular Biology, University of Texas MD Anderson Cancer Center, Houston, Texas 2Genes and Development Graduate Program, University of Texas Graduate School of Biomedical Sciences, Houston, Texas 3Neuroscience Graduate Program, University of Texas Graduate School of Biomedical Sciences, Houston, Texas Abstract The word “nociception” is derived from the Latin “nocere,” which means “to harm.” Nociception refers to the sensory perception of noxious stimuli that have the potential to cause tissue damage. Since the perception of such potentially harmful stimuli often results in behavioral escape responses, nociception provides a protective mechanism that allows an organism to avoid incipient (or further) damage to the tissue. It appears to be universal in metazoans as a variety of escape responses can be observed in both mammalian and non-mammalian vertebrates, as well as diverse invertebrates such as leeches, nematodes, and fruit flies (Sneddon [2004] Brain Research Review 46:123–130; Tobin and Bargmann [2004] Journal of Neurobiology 61:161–174; Smith and Lewin [2009] Journal of Comparative Physiology 195:1089–1106). Several types of stimuli can trigger nociceptive sensory transduction, including noxious heat, noxious chemicals, and harsh mechanical stimulation. Such high-threshold stimuli induce the firing of action potentials in peripheral nociceptors, the sensory neurons specialized for their detection (Basbaum et al. -

616.Full-Text.Pdf
Original Article Orally Active Neurotrophin-Enhancing Agent Protects Against Dysfunctions of the Peripheral Nerves in Hyperglycemic Animals Bunpei Kakinoki,1 Sumito Sekimoto,1 Satoshi Yuki,2 Tetsuya Ohgami,1 Mikiko Sejima,1 Keiji Yamagami,1 and Ken-ichi Saito1 Biological substances with neurotrophic activities, such as In diabetic peripheral neuropathy, it has also been nerve growth factor (NGF) and monosialoganglioside GM1, reported that nerve growth factor (NGF) and substance P have been considered as agents for diabetic peripheral levels in the skin decrease and that their decrease is neuropathy. Because recent studies have suggested that correlated with an impairment of sensory functions (7). decreased availability of these substances might contribute NGF affects the survival of small-diameter sensory nerve to the pathogenesis of diabetic peripheral neuropathy, fibers and sympathetic neurons as well as the maintenance some clinical trials of NGF for diabetic peripheral neurop- athy have been conducted and have led to mixed conclu- of their phenotypic properties, such as producing sub- sions. The major reasons were its limited delivery to the stance P and calcitonin gene–related peptide. The degen- nervous system and adverse effects induced by subcutane- eration of small fibers has a great impact on the quality of ous injection, which was necessary because NGF is a life of diabetic patients because most of the symptoms in polypeptide. The current study investigates whether an diabetic peripheral neuropathy are caused by small fiber orally active sialic acid derivative, MCC-257, has neuropro- dysfunctions. Regardless of the pathogenesis, supplying tective properties in diabetic peripheral nerves. MCC-257 the neurotrophin to neurons has been considered a poten- augmented NGF activity in cultured dorsal root ganglia and tial treatment for neurodegenerative disease, including PC12 (pheochromocytoma 12) cells. -
Structure-Based Discovery of Opioid Analgesics with Reduced Side Effects Aashish Manglik1*, Henry Lin2*, Dipendra K
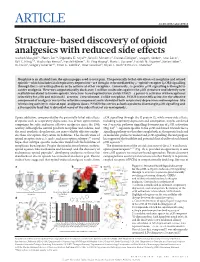
ARTICLE doi:10.1038/nature19112 Structure-based discovery of opioid analgesics with reduced side effects Aashish Manglik1*, Henry Lin2*, Dipendra K. Aryal3*, John D. McCorvy3, Daniela Dengler4, Gregory Corder5, Anat Levit2, Ralf C. Kling4,6, Viachaslau Bernat4, Harald Hübner4, Xi-Ping Huang3, Maria F. Sassano3, Patrick M. Giguère3, Stefan Löber4, Da Duan2, Grégory Scherrer1,5, Brian K. Kobilka1, Peter Gmeiner4, Bryan L. Roth3 & Brian K. Shoichet2 Morphine is an alkaloid from the opium poppy used to treat pain. The potentially lethal side effects of morphine and related opioids—which include fatal respiratory depression—are thought to be mediated by μ-opioid-receptor (μOR) signalling through the β-arrestin pathway or by actions at other receptors. Conversely, G-protein μOR signalling is thought to confer analgesia. Here we computationally dock over 3 million molecules against the μOR structure and identify new scaffolds unrelated to known opioids. Structure-based optimization yields PZM21—a potent Gi activator with exceptional selectivity for μOR and minimal β-arrestin-2 recruitment. Unlike morphine, PZM21 is more efficacious for the affective component of analgesia versus the reflexive component and is devoid of both respiratory depression and morphine-like reinforcing activity in mice at equi-analgesic doses. PZM21 thus serves as both a probe to disentangle μOR signalling and a therapeutic lead that is devoid of many of the side effects of current opioids. Opiate addiction, compounded by the potentially lethal side effects μ OR signalling through the G protein Gi, while many side effects, of opiates such as respiratory depression, has driven optimization including respiratory depression and constipation, may be conferred campaigns for safer and more effective analgesics since the 19th via β -arrestin pathway signalling downstream of μ OR activation 4–6 century. -

Comparative Efficacy of 3 Soluble Epoxide Hydrolase
European Journal of Pharmacology 700 (2013) 93–101 Contents lists available at SciVerse ScienceDirect European Journal of Pharmacology journal homepage: www.elsevier.com/locate/ejphar Neuropharmacology and analgesia Comparative efficacy of 3 soluble epoxide hydrolase inhibitors in rat neuropathic and inflammatory pain models Karen Wagner, Bora Inceoglu, Hua Dong, Jun Yang, Sung Hee Hwang, Paul Jones, Christophe Morisseau, Bruce D. Hammock n Department of Entomology and UC Davis Comprehensive Cancer Center, University of California Davis, One Shields Ave, Davis, CA 95616, United States article info abstract Article history: Epoxy-fatty acids have been recognized as important cell signaling molecules with multiple biological Received 8 June 2012 effects including anti-nociception. The main degradation pathway of these signaling molecules is via Received in revised form the soluble epoxide hydrolase (sEH) enzyme. Inhibitors of sEH extend the anti-nociceptive effects of 13 December 2012 fatty acid epoxides. In this study two models of pain with different etiology, streptozocin induced type I Accepted 19 December 2012 diabetic neuropathic pain and lipopolysaccharide induced inflammatory pain were employed to test Available online 28 December 2012 sEH inhibitors. A dose range of three sEH inhibitors with the same central pharmacophore but varying Keywords: substituent moieties was used to investigate maximal anti-allodynic effects in these two models of Nociception pain. Inhibiting the sEH enzyme in these models successfully blocked pain related behavior in both Soluble epoxide hydrolase models. The sEH inhibitors were more potent and more efficacious than celecoxib in reducing both Inflammatory pain diabetic neuropathic pain and lipopolysaccharide induced inflammatory pain. Because of their ability to Diabetic neuropathic pain Epoxygenated fatty acid block diabetic neuropathic pain sEH inhibition is a promising new approach to treat chronic pain conditions. -

Scientific Investigation of Crude Alkaloids from Medicinal Plants For
Shoaib et al. BMC Complementary and Alternative Medicine (2016) 16:178 DOI 10.1186/s12906-016-1157-2 RESEARCH ARTICLE Open Access Scientific investigation of crude alkaloids from medicinal plants for the management of pain Mohammad Shoaib1*, Syed Wadood Ali Shah1, Niaz Ali2, Ismail Shah1, Shafi Ullah1, Mehreen Ghias1, Muhammad Nawaz Tahir3, Farah Gul4, Sohail Akhtar5, Abd Ullah1, Wajid Akbar1 and Asad Ullah1 Abstract Background: Tissue damage is associated with pain, which is an alarming sign. Aspirin and morphine have been widely used in recent decades for management of pain. Medicinal herbs have been in use for treatment of different diseases for centuries. Many of these herbs possess analgesic activity with relatively less incidences of adverse effects. The strong positive correlation of alkaloids in medicinal plants for analgesic activity persuades an intention to determine possible analgesic activity of total alkaloids extracted from the selected medicinal plants using animal models to answer its possible mechanisms. Methods: Crude alkaloids from selected medicinal plants (Woodfordia fruticosa, Adhatoda vasica, Chenopodium ambrosioides, Vitex negundo, Peganum harmala and Broussonetia papyrifera) were extracted as per reported literature. The test crude alkaloids were screened foracute toxicity study. Writhings induced by acetic acid, tail immersion method and formalin-induced nociception assay procedures were used for possible analgesic effects of the crude alkaloids. Results: Crude alkaloids were safe up to dose of 1250 mg/kg body weight in mice. The alkaloids significantly reduced the abdominal constrictions, and increased the time for paw licking response in both phases with a significant raise in latency time in nociception models (P ≤ 0.05). -

WO 2017/049252 Al 23 March 2017 (23.03.2017) P O P C T
(12) INTERNATIONAL APPLICATION PUBLISHED UNDER THE PATENT COOPERATION TREATY (PCT) (19) World Intellectual Property Organization International Bureau (10) International Publication Number (43) International Publication Date WO 2017/049252 Al 23 March 2017 (23.03.2017) P O P C T (51) International Patent Classification: (81) Designated States (unless otherwise indicated, for every A61K 31/5513 (2006.01) A61P 25/14 (2006.01) kind of national protection available): AE, AG, AL, AM, C12N 15/861 (2006.01) A61P 25/28 (2006.01) AO, AT, AU, AZ, BA, BB, BG, BH, BN, BR, BW, BY, A61P 3/04 (2006.01) BZ, CA, CH, CL, CN, CO, CR, CU, CZ, DE, DK, DM, DO, DZ, EC, EE, EG, ES, FI, GB, GD, GE, GH, GM, GT, (21) International Application Number: HN, HR, HU, ID, IL, IN, IR, IS, JP, KE, KG, KN, KP, KR, PCT/US2016/052384 KW, KZ, LA, LC, LK, LR, LS, LU, LY, MA, MD, ME, (22) International Filing Date: MG, MK, MN, MW, MX, MY, MZ, NA, NG, NI, NO, NZ, 17 September 2016 (17.09.201 6) OM, PA, PE, PG, PH, PL, PT, QA, RO, RS, RU, RW, SA, SC, SD, SE, SG, SK, SL, SM, ST, SV, SY, TH, TJ, TM, (25) Filing Language: English TN, TR, TT, TZ, UA, UG, US, UZ, VC, VN, ZA, ZM, (26) Publication Language: English ZW. (30) Priority Data: (84) Designated States (unless otherwise indicated, for every 62/220,077 17 September 2015 (17.09.2015) US kind of regional protection available): ARIPO (BW, GH, 62/220,087 17 September 2015 (17.09.2015) US GM, KE, LR, LS, MW, MZ, NA, RW, SD, SL, ST, SZ, TZ, UG, ZM, ZW), Eurasian (AM, AZ, BY, KG, KZ, RU, (71) Applicant: SWITCH BIO, INC.