The Paralympic Athlete Dedicated to the Memory of Trevor Williams Who Inspired the Editors in 1997 to Write This Book
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Disability Classification System
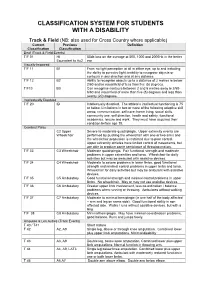
CLASSIFICATION SYSTEM FOR STUDENTS WITH A DISABILITY Track & Field (NB: also used for Cross Country where applicable) Current Previous Definition Classification Classification Deaf (Track & Field Events) T/F 01 HI 55db loss on the average at 500, 1000 and 2000Hz in the better Equivalent to Au2 ear Visually Impaired T/F 11 B1 From no light perception at all in either eye, up to and including the ability to perceive light; inability to recognise objects or contours in any direction and at any distance. T/F 12 B2 Ability to recognise objects up to a distance of 2 metres ie below 2/60 and/or visual field of less than five (5) degrees. T/F13 B3 Can recognise contours between 2 and 6 metres away ie 2/60- 6/60 and visual field of more than five (5) degrees and less than twenty (20) degrees. Intellectually Disabled T/F 20 ID Intellectually disabled. The athlete’s intellectual functioning is 75 or below. Limitations in two or more of the following adaptive skill areas; communication, self-care; home living, social skills, community use, self direction, health and safety, functional academics, leisure and work. They must have acquired their condition before age 18. Cerebral Palsy C2 Upper Severe to moderate quadriplegia. Upper extremity events are Wheelchair performed by pushing the wheelchair with one or two arms and the wheelchair propulsion is restricted due to poor control. Upper extremity athletes have limited control of movements, but are able to produce some semblance of throwing motion. T/F 33 C3 Wheelchair Moderate quadriplegia. Fair functional strength and moderate problems in upper extremities and torso. -

Grand Prix Freestyle FEI Dressage World Cup
D02 - Int. dressage competition - Grand Prix Freestyle FEI Dressage World Cup™ Qualifier 2019/2020 presented by VriendenLoterij Test: FEI Grand Prix Freestyle Edition 1999, revision 2009, update 2017 Saturday, 25. January 2020 - 12.15 hrs O F F I C I A L R E S U L T Pos. Rider Nation E H C M B Total Horse No. 1. Isabell Werth A 85.000 83.000 85.250 85.500 84.250 B 95.800 94.600 96.800 97.200 95.400 388 Weihegold OLD GER 90.280 black / 15y / M / Blue Hors Don Schufro / Sandro Hit / OLDBG / 102ZI90 / Christine Arns-Krogmann % 90.400 88.800 91.025 91.350 89.825 388 (2) (1) (1) (1) (1) 13,750.00 EUR 2. Charlotte Dujardin A 85.500 81.250 86.750 84.000 84.750 B 95.800 93.400 94.400 94.800 94.400 393 Mount St John Freestyle GBR 89.505 dbay / 11y / M / Fidermark / Donnerhall 11 / HANN / 105BZ34 / Emma & Jill Blundell % 90.650 87.325 90.575 89.400 89.575 393 (1) (3) (2) (2) (2) 10,000.00 EUR 3. Edward Gal A 82.500 77.750 82.000 81.000 79.000 B 89.800 91.800 92.400 89.600 88.000 381 Glock's Zonik N.O.P. NED 85.385 bay / 12y / S / Blue Hors Zack / Romanov / DWB / 104AW69 / Glock Hpc Nl B.V. % 86.150 84.775 87.200 85.300 83.500 381 (3) (4) (3) (3) (5) 7,500.00 EUR 4. Jessica von Bredow-Werndl A 82.000 77.750 80.500 76.250 78.000 B 89.400 91.200 93.600 91.200 90.400 376 Zaire-E GER 85.030 bay / 16y / M / Son de Niro / Jazz / KWPN / 102VM17 / Aubenhausen GbR % 85.700 84.475 87.050 83.725 84.200 376 (4) (5) (4) (4) (3) 5,625.00 EUR 5. -
May Newsletter 2014.Pdf
A Monthly Publication of the Potomac Valley Dressage Association • MAY 2014 • Vol. 50, Issue 5 Send your 2014 Calendar Items to [email protected]. Calendar JUNE 2014 Deadline: MAY 10 Calendar Editor: Jocelyn Pearson of Events www.pvda.org for complete calendar PVDA Schooling Shows on separate calendar at Sunset Bay Farm, Onancock, Va. Contact ChesapeakeDressage.com or call 410-267-7174 May [email protected] or 757-302-0224 NAJYRC in Lexington, Ky. www. CDCTA Licensed Show at Morven Park, 15-20 3-4 25-26 Dressage at Heavenly Waters, Licensed usdf.org Leesburg, Va. See www.cdcta.com Show. See www.usdfregion1.org WindCrest Farm Schooling Show, Dressage at The Meadow. See 19 3-4 31-June 1 Adult Team Competition South hosted by Clarksburg, Md. An evening schooling show in a usdfregion1.org NCDCTA in Raleigh, N.C. See www.usdfregion1.org friendly and fun setting. Avoid the July sun, join 4 Shore Dressage Chapter Dressage Clinic 31-FADS at Sugarloaf Equestrian Center, Boyds, us for dressage with wine and cheese. Contact with Deri Jeffers at Sunset Bay Farm, Md. See www.frederickdressage.org Dede Bierbrauer, 301-972-5102 or windcrestii@ Onancock, Va. Contact [email protected] or aol.com 757-302-0224 June 19 Hope Floats Equestrian Dressage Show Afternoon Dressage Clinic with Felicitas 6 6-8 VADAnova Licensed Show at Morven Park, Series, Show 2. See show info and registration at Von Neumann Cosel at Equidistance Horse www.hopefloatsequestrian.com Center. Free auditing and no trailer-in fee for Leesburg, Va. See www.vadanova.org Schooling Show at Begin Again Farm, those who want to ride. -
IPC Accessibility Guide
2 TABLE OF CONTENTS FIGURES AND TABLES ................................................................................................................. 8 Foreword ........................................................................................................................................... 10 Introduction ................................................................................................................................. 10 Evolving content ......................................................................................................................... 10 Disclosure ...................................................................................................................................... 11 Structure and content of the IPC Accessibility Guide ...................................................... 11 Content ........................................................................................................................................... 11 Executive summary ......................................................................................................................... 12 Aim and purpose of the Guide ................................................................................................ 12 Key objectives of the Guide ..................................................................................................... 12 Target audience of the Guide ................................................................................................. 12 1 General information -

2018 Jessica Uniack Beach to Bay Race Long Beach Yacht Club
2018 Jessica Uniack Beach to Bay Race Long Beach Yacht Club Results for 2018 Jessica Uniack Beach to Bay Race CFJ Class Sailed: 1, Discards: 0, To count: 1, Entries: 25, Scoring system: Appendix A Class SailNo Club HelmName CrewName R1 Total Nett CFJ HHSF Jack Haliday Nicholas Ridout CFJ HHSF Trae Sanchez Ben Hagadorn CFJ LBYC 7 LBYC Nicky Lech Kai Bramble 1.0 1.0 1.0 CFJ 22 ABYC Nicholas Muller Ulises Lewis 2.0 2.0 2.0 CFJ LBYC 10 LBYC Preston Woodworth Alex Lech 3.0 3.0 3.0 CFJ 43 ABYC Summer Drake Paige Odell 4.0 4.0 4.0 CFJ 23 ABYC Nikhil Stewart Jamarcus Parker 5.0 5.0 5.0 CFJ 42 ABYC Sean colley Thomas Dobson 6.0 6.0 6.0 CFJ 44 ABYC Nicolas Sanchez Nicole Morikawa 7.0 7.0 7.0 CFJ 24 ?? 8.0 8.0 8.0 CFJ 0 HHSF Trae Sanchez Ben H 9.0 9.0 9.0 CFJ LBYC 2 LBYC Kyer Fox Isaure Chalandon 10.0 10.0 10.0 CFJ LBYC 9 LBYC Sawyer Bambam-Moak Katin Cathey 11.0 11.0 11.0 Class SailNo Club HelmName CrewName R1 Total Nett CFJ 46 ABYC Elisabeth Rossbach Troy Davidson 12.0 12.0 12.0 CFJ 00 HHSF Jack Haliday Nicholas 13.0 13.0 13.0 CFJ 41 ABYC Michael Colley Emilia Anctil 14.0 14.0 14.0 CFJ 6161 DPYC Riley Lenthall 15.0 15.0 15.0 CFJ 9PYSF HHYC Jack Busche Nolan Davis 16.0 16.0 16.0 CFJ 1510 DPYC Ryan Brown Colin Sekerka 17.0 17.0 17.0 CFJ 5151 DPYC Christopher Andersen Hunter Laws 18.0 18.0 18.0 CFJ LBYC 3 LBYC Luke Bramble Rio Dumont 19.0 19.0 19.0 CFJ LBYC 5 LBYC Jack Snow Reese Lapham 26.0 DSQ 26.0 26.0 CFJ 6161 DPYC Carsen Lenthall 26.0 DNC 26.0 26.0 CFJ 6161 DPYC Riley Lenthall 26.0 DNC 26.0 26.0 CFJ 5151 DPYC Hunter Laws Christopher Anderson -
Ifds Functional Classification System & Procedures
IFDS FUNCTIONAL CLASSIFICATION SYSTEM & PROCEDURES MANUAL 2009 - 2012 Effective – 1 January 2009 Originally Published – March 2009 IFDS, C/o ISAF UK Ltd, Ariadne House, Town Quay, Southampton, Hampshire, SO14 2AQ, GREAT BRITAIN Tel. +44 2380 635111 Fax. +44 2380 635789 Email: [email protected] Web: www.sailing.org/disabled 1 Contents Page Introduction 5 Part A – Functional Classification System Rules for Sailors A1 General Overview and Sailor Evaluation 6 A1.1 Purpose 6 A1.2 Sailing Functions 6 A1.3 Ranking of Functional Limitations 6 A1.4 Eligibility for Competition 6 A1.5 Minimum Disability 7 A2 IFDS Class and Status 8 A2.1 Class 8 A2.2 Class Status 8 A2.3 Master List 10 A3 Classification Procedure 10 A3.0 Classification Administration Fee 10 A3.1 Personal Assistive Devices 10 A3.2 Medical Documentation 11 A3.3 Sailors’ Responsibility for Classification Evaluation 11 A3.4 Sailor Presentation for Classification Evaluation 12 A3.5 Method of Assessment 12 A3.6 Deciding the Class 14 A4 Failure to attend/Non Co-operation/Misrepresentation 16 A4.1 Sailor Failure to Attend Evaluation 16 A4.2 Non Co-operation during Evaluation 16 A4.3 International Misrepresentation of Skills and/or Abilities 17 A4.4 Consequences for Sailor Support Personnel 18 A4.5 Consequences for Teams 18 A5 Specific Rules for Boat Classes 18 A5.1 Paralympic Boat Classes 18 A5.2 Non-Paralympic Boat Classes 19 Part B – Protest and Appeals B1 Protest 20 B1.1 General Principles 20 B1.2 Class Status and Protest Opportunities 21 B1.3 Parties who may submit a Classification Protest -

Marelli D6C & D5C ATEX Motor Technical Catalogue
Motors for This catalogue refers to ATEX Motors belonging to Group I Category M2 and Group II Category 2G, 2D, 2GD as described. STANDARDS ® BEARINGS Hazardous Areas The ATEX Motors described in this catalogue are manufactured in accordance with IEC 60034-1-5-6-7-8-9-12-14, IEC 60072-1, EN 50347, EN 60079- D5, D6 SERIES Frame Size (mm) D - end N - end Frame Size Poles B 3 V 1 MarelliMotori 0-1-7, EN 61241-0-1. 71* 6202-2Z 6202-2Z D - end N - end D - end N - end I M2, II 2G, II 2D EUROPEAN DIRECTIVES 355-400 2 6217-C3 6217-C3 6217-C3 7217 B 80* 6204-2Z 6204-2Z Ex d/de I, Ex d/de IIB, Ex tD A21 IP65 Title Directive 90* 6205-2Z 6205-2Z 355 4 NU222-C3 6217-C3 NU222-C3 6217-C3 + 7217 B Equipment and protective system intended for use in potentially explosive atmospheres (ATEX) 94/9/EC 100* 6206-2Z 6206-2Z 400 4 NU222-C3 6222-C3 NU222-C3 6222-C3 + 7222 B Electromagnetic Compatibility (EMC) 2004/108/IEC 112* 6206-2Z 6206-2Z Low Voltage Directive (LVD) 2006/95/EC 132* 6308-2Z 6308-2Z HEADQUARTERS ITALIAN OFFICES Machinery Directive (MD) 98/37/EC 160 - 180M 6310-Z-C3 6209-Z-C3 Marelli Motori S.p.A. Milan CERTIFICATES 180L 6310-Z-C3 6210-Z-C3 Via Sabbionara, 1 Via Cesare Cantù, 29 200 6312-Z-C3 6210-Z-C3 Frame size Number Temperature Limits 36071 Arzignano (VI) Italy 20092 Cinisello Balsamo (MI) Italy 225 6313-Z-C3 6213-Z-C3 71-132 BVI 08 ATEX 0001 -20°C +40°C* 160-315 CESI 02 ATEX 071 -20 C +40 C* 250 6314-Z-C3 6213-Z-C3 (T) +39.0444.479711 (T) +39.02.660.131.66 ° ° These tables describe the bearing types used in standard configurations. -

Special-Sessions-1998-37941-600-21
INTERNATIONAL OLYMPIC ACADEMY 6th INTERNATIONAL POST GRADUATE SEMINAR 1/5-12/6/1998 4th JOINT INTERNATIONAL SESSION FOR DIRECTORS OF NATIONAL OLYMPIC ACADEMIES, MEMBERS AND STAFF OF NATIONAL OLYMPIC COMMITTEES AND INTERNATIONAL SPORTS FEDERATIONS 7-14/5/1998 ANCIENT OLYMPIA ISBN: 960-8144-04-3 ISSN: 1108-6831 Published and edited by the International Olympic Academy. Scientific supervisor: Dr. Konstantinos Georgiadis/IOA Dean. Athens 2000 EPHORIA OF THE INTERNATIONAL OLYMPIC ACADEMY President Nikos FILARETOS (I.O.C. Member) 1st Vice-President Sotiris YAGAS t 2nd Vice-President Georgios MOISSIDIS Dean Konstantinos GEORGIADIS Member ex-officio Lambis NIKOLAOU (I.O.C. Member) Members Dimitris DIATHESSOPOULOS Georgios GEROLIMBOS Ioannis THEODORAKOPOULOS Epaminondas KIRIAZIS Cultural Consultant Panayiotis GRAVALOS Honorary President Juan Antonio SAMARANCH Honorary Vice-President Nikolaos YALOURIS 3 I.O.C. COMMISSION FOR THE INTERNATIONAL OLYMPIC ACADEMY AND OLYMPIC EDUCATION President Nikos FILARETOS IOC Member in Greece Vice-President Carol Ann LETHEREN IOC Member in Canada Members Fernando Ferreira Lima BELLO IOC Member in Portugal Valeriy BORZOV IOC Member in Ukraine Ivan DIBOS IOC Member in Peru Francis NYANGWESO IOC Member in Uganda Mohamed ZERGUINI IOC Member in Algeria Representatives George MOISSIDIS Fern. BELTRANENA VALLARADES Rene ROCH Representative of IFs Dieter LANDSBERG-VELEN Representative of IFs Philippe RIBOUD Representative of Athletes Individual Members Helen BROWNLEE (Australia) Conrado DURANTEZ (Spain) Yoon-bang KWON (Korea) Marc MAES (Belgium) Prof. Norbert MUELLER (Germany) 4 PROLOGUE The publication of the proceedings of the IOA's special ses- sions, for the second consecutive year, is one more contribution of the Ephoria of the Academy and the Hellenic Olympic Com- mittee to Olympism and Olympic Education. -

TPS23861 IEEE 802.3At Quad Port Power-Over-Ethernet PSE
Product Order Technical Tools & Support & Folder Now Documents Software Community TPS23861 SLUSBX9I –MARCH 2014–REVISED JULY 2019 TPS23861 IEEE 802.3at Quad Port Power-over-Ethernet PSE Controller 1 Features 3 Description The TPS23861 is an easy-to-use, flexible, 1• IEEE 802.3at Quad Port PSE controller IEEE802.3at PSE solution. As shipped, it – Auto Detect, classification automatically manages four 802.3at ports without the – Auto Turn-On and disconnect need for any external control. – Efficient 255-mΩ sense resistor The TPS23861 automatically detects Powered • Pin-Out enables Two-Layer PCB Devices (PDs) that have a valid signature, determines • Kelvin Current Sensing power requirements according to classification and applies power. Two-event classification is supported • 4-Point detection for type-2 PDs. The TPS23861 supports DC • Automatic mode – as shipped disconnection and the external FET architecture – No External terminal setting required allows designers to balance size, efficiency and – No Initial I2C communication required solution cost requirements. • Semi-Automatic mode – set by I2C command The unique pin-out enables 2-layer PCB designs via logical grouping and clear upper and lower – Continuous Identification and Classification differentiation of I2C and power pins. This delivers – Meets IEEE 400-ms TPON specification best-in-class thermal performance, Kelvin accuracy – Fast-Port shutdown input and low-build cost. – Operates best when used in conjunction with In addition to automatic operation, the TPS23861 system reference code supports Semi-Auto Mode via I2C control for precision http://www.ti.com/product/TPS23861/toolssoftw monitoring and intelligent power management. are Compliance with the 400-ms TPON specification is ensured whether in semi-automatic or automatic • Optional I2C control and monitoring mode. -

Original Sport Performance Indicators in Football 7- A
Rev.int.med.cienc.act.fís.deporte - vol. 19 - número 74 - ISSN: 1577-0354 Gamonales, J.M.; León, K.; Jiménez, A. y Muñoz, J. (2019) Indicadores de rendimiento deportivo en el fútbol-7 para personas con parálisis cerebral / Sport Performance Indicators in Football 7- A-Side for People with Cerebral Palsy. Revista Internacional de Medicina y Ciencias de la Actividad Física y el Deporte vol. 19 (74) pp. 309-328 Http://cdeporte.rediris.es/revista/revista74/artindicadores1023.htm DOI: http://doi.org/10.15366/rimcafd2019.74.009 ORIGINAL SPORT PERFORMANCE INDICATORS IN FOOTBALL 7- A-SIDE FOR PEOPLE WITH CEREBRAL PALSY INDICADORES DE RENDIMIENTO DEPORTIVO EN EL FÚTBOL-7 PARA PERSONAS CON PARÁLISIS CEREBRAL Gamonales, J.M.1; León, K.1,2; Jiménez, A.1 y Muñoz-Jiménez, J.1,2 1 Facultad de Ciencias de la Actividad Física y el Deporte. Universidad de Extremadura (España) [email protected], [email protected], [email protected], [email protected] 2 Universidad Autónoma de Chile (Chile) [email protected], [email protected] Spanish-English translator: Rocío Domínguez Castells. [email protected] ACKNOWLEDGEMENTS AND/OR FUNDING This work was developed by the Research Group for the Optimization of Training and Sport Performance (Grupo de Optimización del Entrenamiento y Rendimiento Deportivo, G.O.E.R.D.) of the Faculty of Sport Sciences of the University of Extremadura. This work has been supported by the funding for research groups (GR15122) of the Government of Extremadura (Employment and infrastructure officeConsejería de Empleo e Infraestructuras), with the contribution of the European Union through the European Regional Development Fund (ERDF). -

Classification Made Easy Class 1
Classification Made Easy Class 1 (CP1) The most severely disabled athletes belong to this classification. These athletes are dependent on a power wheelchair or assistance for mobility. They have severe limitation in both the arms and the legs and have very poor trunk control. Sports Available: • Race Runner (RR1) – using the Race Runner frame to run, track events include 100m, 200m and 400m. • Boccia o Boccia Class 1 (BC1) – players who fit into this category can throw the ball onto the court or a CP2 Lower who chooses to push the ball with the foot. Each BC1 athlete has a sport assistant on court with them. o Boccia Class 3 (BC3) – players who fit into this category cannot throw the ball onto the court and have no sustained grasp or release action. They will use a “chute” or “ramp” with the help from their sport assistant to propel the ball. They may use head or arm pointers to hold and release the ball. Players with a impairment of a non cerebral origin, severely affecting all four limbs, are included in this class. Class 2 (CP2) These athletes have poor strength or control all limbs but are able to propel a wheelchair. Some Class 2 athletes can walk but can never run functionally. The class 2 athletes can throw a ball but demonstrates poor grasp and release. Sports Available: • Race Runner (RR2) - using the Race Runner frame to run, track events include 100m, 200m and 400m. • Boccia o Boccia Class 2 (BC2) – players can throw the ball into the court consistently and do not need on court assistance. -
Everything Within Reach! Myoelectric-Controlled Arm Prostheses
Everything within Reach! Myoelectric-controlled Arm Prostheses Information for user Table of Contents Myoelectric-controlled Arm Prostheses ������������������������������������������ 4 Cable-controlled Arm Prostheses ����������������������������������������������������� 6 Passive Arm Prostheses ����������������������������������������������������������������������� 8 Technology for People ���������������������������������������������������������������������������� 9 Prosthetic Fitting ����������������������������������������������������������������������������������� 10 System Electric Hands ����������������������������������������������������������������������� 12 SensorHand Speed ����������������������������������������������������������������������������� 14 System Electric Greifers �������������������������������������������������������������������� 16 Individual Combination and Adaptation ����������������������������������������� 18 Upper Arm Prostheses – DynamicArm ������������������������������������������� 20 Making Exploration Fun ��������������������������������������������������������������������� 24 Children’s Hand 2000 ������������������������������������������������������������������������� 26 Post-operative Therapy ����������������������������������������������������������������������� 28 Residual Limb Pain and Phantom Pain ������������������������������������������ 30 The Socket Decides ���������������������������������������������������������������������������� 32 Pay Attention to Yourself! �������������������������������������������������������������������