Manual Wheelchairs 15
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Hoist to Transfer Athletes from Wheelchair Into a Kayak
Hoist to Transfer Athletes from Wheelchair into a Kayak Team Members: Jennifer Batryn Javier Mendez Kyle Mooney Sponsors: Team Advisors: Maggie Palchak, Disabled Sports Eastern Sierra Program Sarah Harding, Cal Poly Mechanical Engineering Department Coordinator Dr. Kevin Taylor, Cal Poly Kinesiology Department E.L. Smoogen, Disabled Sports Eastern Sierra Dr. Brian Self, Cal Poly Mechanical Engineering Department June 7, 2013 Team Kayakity Quacks California Polytechnic State University, San Luis Obispo [email protected] Statement of Disclaimer Since this project is a result of a class assignment, it has been graded and accepted as fulfillment of the course requirements. Acceptance does not imply technical accuracy or reliability. Any use of information in this report is done at the risk of the user. These risks may include catastrophic failure of the device or infringement of patent or copyright laws. California Polytechnic State University at San Luis Obispo and its staff cannot be held liable for any use or misuse of the project. 2 Team Kayakity Quacks California Polytechnic State University, San Luis Obispo [email protected] Table of Contents 1 - Introduction ............................................................................................................................... 7 2 - Background Research ................................................................................................................ 8 2.1 Kayak Design ................................................................................................................... -

FOR INDIVIDUALS WHO USE a WHEELCHAIR Toolkit for the Fitness Professional Table of Contents
FITNESS ASSESSMENTS FOR INDIVIDUALS WHO USE A WHEELCHAIR Toolkit for the Fitness Professional Table of Contents Introduction to Fitness Assessments 4 What are Fitness Assessments 4 Why are Fitness Assessments Important 4 What Will Your Client Need 4-5 Assessments Defined 5 Order of Tests 5 Preparation for Fitness Assessments 6 Pre Assessment 6 Types of Fitness Assessments 6 Cardiovascular Testing 7 Arm Ergometer Test 7-9 Six-Minute Push Test 9-10 Muscular Strength Testing 10 Medicine Ball Throw Test 10-11 Handgrip Test 11-12 One-Repetition Maximum Test 12-13 Muscular Endurance Testing 14 Push-Up Test 14 Curl Up Test 15-16 Balance Testing 16 Seated Balance Test 16-17 Modified Functional Reach Test 18 Flexibility Testing 19 Shoulder (Range of Motion) Flexibility Test 19-20 Back Scratch Test 20 Body Composition Testing 21 Circumference Measurements 21-23 2 Fitness Assessments for Individuals who use a Wheelchair DEXA 23-26 BIA 26 Disability Awareness 27 Are you KnowledgeABLE 27 Disability Etiquette 28-29 References 30-34 Assessment Recording Resources 35 VO2max Arm Ergometer Test Recording Sheet 35 Six-Minute Push Test Recording Sheet 36 Medicine Ball Throw Test Recording Sheet 37 Handgrip Test Recording Sheet 39 One-Repetition Maximum Test Recording Sheet 40 Push-Up/Curl Up Test Recording Sheet 41-42 Seated Balance Test Recording Sheet 43 Modified Functional Reach Test Recording Sheet 44 Shoulder (ROM) Flexibility Test Recording Sheet 45 Circumference Measurements Test Recording Sheet 46 DEXA Test Recording Sheet 48 BIA Test Recording Sheet 49 To Watch a Video Series on How To Conduct These Tests go to www.nchpad.org/fitnesstesting. -

Wheelchair Page 9 Page 11 Page 13
AMIGO Amigo Mobility International sold the first motorized shopping cart in 1970 just two years after Amigo was founded. It was in 1968 when Al Thieme invented the first three-wheel personal mobility vehicle for a person living with multiple sclerosis. ValueShopper ValueShopper XL SmartShopper Page 3 Page 5 Page 7 SmartChair SmartChair XT Wheelchair Page 9 Page 11 Page 13 Move more with our material handling carts, Page 21 With our roots planted in healthcare, finding quality solutions for mobility needs has become our passion. We have over half a century’s worth of experience in designing and manufacturing products that serve others, and our pace of innovation continues to accelerate. TM TM From the creation of a single healthcare unit, Amigo has DEX DEX PRO+ grown to include a robust grocery and retail division and is now expanding into material handling. Moving more is our DEX PRO TM business, and our mission continues to be Improving Lives Through Mobility®. MAX TM MAX PRO TM ValueShopper “Wow” isn’t an expression you might expect when talking about motorized shopping carts, but we’ve heard it. You lift the ValueShopper seat to see the inner workings of one of the world’s most popular models and you get it. The front drive motor has modular components that keep things simple and sensible – only replace the parts you need, not the whole motor. A front drive motor features a tight turning radius so shoppers can navigate aisles with ease. Match your ValueShoppers to your decor: Front drive, most popular 3 amigoshopper.com Commercial Product Guide ValueShopper XL So hefty! Who doesn’t appreciate the deals buying in bulk provide? Know any people with limited mobility that know the value of stocking up? So do we, and the ValueShopper XL can accommodate large merchandise. -

Wheelchair Racing 101
Wheelchair Racing 101 Tami English Seattle Adaptive Sports [email protected] www.seattleadaptivesports.org Track Chair Basics • What do we need? – Race chair • Can be obtained by contacting the adapted sports program on the East or West side of the state. – Gloves • Can be obtained by contacting the adapted sports program on the East or West side of the state or ordered directly from Sportaid.com. – Helmet • Can be any standard bike helmet Basics of Pushing • It is completely different from a standard day chair push, but very similar to the A’s and B’s of running • If the handrim is a clock, the push starts at 1:00- 2:00 and continues on around to the bottom of the handrim, releasing at 6:00-7:00. • The arm extends behind in full extension, then flexes and “punches” the handrim again at 1:00- 2:00 YouTube Videos • Seattle Adaptive Sport Channel Track/Field Instructional (1) http://www.youtube.com/watch?v=vbVZBJu4LTQ Track/Field Instructional (2) http://www.youtube.com/watch?v=pMq6i7MoshQ • National Alliance for Youth Sports Coaching Youth with Disabilities http://www.youtube.com/playlist?list=PL7E7E3BB9E22DA793 • Scot Hollonbeck – Track Athlete/Coach Wheelchair Stroke http://www.youtube.com/watch?v=TgtJO_YRVng Racing Gear Bag http://www.youtube.com/watch?v=EHYA5mUxcrk Wheelchair Transfer http://www.youtube.com/watch?v=fuTu_2-ZhgE • Wheelchair Racing in Slow Motion http://www.youtube.com/watch?v=pvPTBBZExDI Emerging Elite Athletes http://www.teamusa.org/US-Paralympics/Sports/Track-and-Field How is this different from Special Olympics? • These athletes have a primary diagnosis of a physical disability and would not qualify for Special Olympics. -

Two Centuries of Wheelchair Design, from Furniture to Film
Enwheeled: Two Centuries of Wheelchair Design, from Furniture to Film Penny Lynne Wolfson Submitted in partial fulfillment of the Requirements for the degree Master of Arts in the History of the Decorative Arts and Design MA Program in the History of the Decorative Arts and Design Cooper-Hewitt, National Design Museum, Smithsonian Institution and Parsons The New School for Design 2014 2 Fall 08 © 2014 Penny Lynne Wolfson All Rights Reserved 3 ENWHEELED: TWO CENTURIES OF WHEELCHAIR DESIGN, FROM FURNITURE TO FILM TABLE OF CONTENTS LIST OF ILLUSTRATIONS ACKNOWLEDGEMENTS i PREFACE ii INTRODUCTION 1 CHAPTER 1. Wheelchair and User in the Nineteenth Century 31 CHAPTER 2. Twentieth-Century Wheelchair History 48 CHAPTER 3. The Wheelchair in Early Film 69 CHAPTER 4. The Wheelchair in Mid-Century Films 84 CHAPTER 5. The Later Movies: Wheelchair as Self 102 CONCLUSION 130 BIBLIOGRAPHY 135 FILMOGRAPHY 142 APPENDIX 144 ILLUSTRATIONS 150 4 List of Illustrations 1. Rocking armchair adapted to a wheelchair. 1810-1830. Watervliet, NY 2. Pages from the New Haven Folding Chair Co. catalog, 1879 3. “Dimension/Weight Table, “Premier” Everest and Jennings catalog, April 1972 4. Screen shot, Lucky Star (1929), Janet Gaynor and Charles Farrell 5. Man in a Wheelchair, Leon Kossoff, 1959-62. Oil paint on wood 6. Wheelchairs in history: Sarcophagus, 6th century A.D., China; King Philip of Spain’s gout chair, 1595; Stephen Farffler’s hand-operated wheelchair, ca. 1655; and a Bath chair, England, 18th or 19th century 7. Wheeled invalid chair, 1825-40 8. Patent drawing for invalid locomotive chair, T.S. Minniss, 1853 9. -
Americans with Disabilities Act Transition Plan
Americans with Disabilities Act Transition Plan December 2012 City of Hobart ADA Coordinator Mike Hannigan, Building Commissioner 414 Main Street City of Hobart, IN 46342 1 COMMON COUNCIL OF THE CITY OF HOBART, INDIANA 2 Resolution Number 2012-30 3 4 A Resolution Approving, Adopting and Making 5 ADA Transition Plan Effective for the City of Hobart 6 7 8 WHEREAS, the Common Council (“Council”) of the City of Hobart, Indiana (“City”) 9 has been advised that the City is obligated to prepare, adopt and make effective in the City a 10 Transition Plan for the implementation of physical pedestrian improvements within the public 11 rights of way of the City as required by the Americans with Disabilities Act of 1990 (“ADA”), as 12 amended, (42 U.S.C §12101, et seq.); and 13 WHEREAS, a draft of such Transition Plan has been under development since early in 14 2012 and has been compiled by Mike Hannigan, Building Official of the City and Jake 15 Dammarell, City Project Manager, such final draft being attached hereto and made a part hereof; 16 and 17 WHEREAS, by the adoption of Ordinance 2011-39 on December 7, 2011, the Council 18 assigned the Building Department as the ADA compliance program for the City, and designated 19 the City Building Commissioner as ADA Coordinator; and 20 WHEREAS, the Council desires to approve, adopt and make such plan effective in the 21 City through this Resolution. 22 THEREFORE, BE IT RESOLVED by the Common Council of the City of Hobart as 23 follows: 24 The Americans with Disabilities Act Transition Plan, which is attached hereto, is adopted 25 and approved, in all respects, and is hereby made effective in the City of Hobart, according to its 26 terms, forthwith. -

Power-Assist Wheelchair Attachment Catherine Van Blommestein
Santa Clara University Scholar Commons Mechanical Engineering Senior Theses Engineering Senior Theses 6-12-2019 Power-Assist Wheelchair Attachment Catherine van Blommestein Ryan Boyce Rosemary Cole Matthew aM rks Follow this and additional works at: https://scholarcommons.scu.edu/mech_senior Part of the Mechanical Engineering Commons POWER‒ASSIST WHEELCHAIR ATTACHMENT By Catherine van Blommestein, Ryan Boyce, Rosemary Cole, and Matthew Marks SENIOR DESIGN PROJECT REPORT Submitted to the Department of Mechanical Engineering of SANTA CLARA UNIVERSITY in Partial Fulfillment of the Requirements for the degree of Bachelor of Science in Mechanical Engineering Santa Clara, California 2019 Abstract This senior design project sought to combine the best characteristics of manual and power wheelchairs by creating a battery-powered attachment to propel a manual wheelchair. The primary customer needs were determined to be affordability, portability, and travel on uneven surfaces. After the initial prototype, using a hub motor proved unsuccessful, so a second design was developed that consisted of a gear reduction motor and drive wheel connected to the back of the wheelchair by a trailing arm that could be easily attached/detached from the frame. The prototype of the second design succeeded in meeting most of the project goals related to cost, off-road capability, inclines, and range. Improvements can be made by reducing the attachment weight and improving user control of the device. iii Acknowledgements The team would like to acknowledge the important contributions that the following parties made towards the success of this project: ● Drs. Robert Marks, Tony Restivo, and Don Riccomini for their guidance and patience throughout the year ● Donald MacCubbin and Calvin Sellers for their time and expertise in the machine shop ● Stryker Endoscopy for their generosity with building a custom sprocket ● Pacific Heat Treatment for their high quality services, quick turnaround time, and generosity iv Table of Contents 1. -

Adapted Nordic Skiing Version 1.0 022316
ADAPTED NORDIC SKIING The NWBA recommends that wheelchair basketball be introduced as an inte- grated sport open to all students regardless of the presence of a disability. This will increase the number of potential athletes and insure the potential for GUIDELINESadequate numbers to field a team. VERSION 1.0 ABOUT ATHLETICS FOR ALL History The Office for Civil Rights (OCR) of the S.U. Department of Education issued a Dear Colleague Letter on January 25, 2013 clarifying elementary, secondary, and postsecondary level schools’ responsibilities under Section 504 of the Rehabilitation Act of 1973 (Rehab Act) to provide extracurricular athletic opportunities for students with disabilities. The guidance clarifies when and how schools should include students with disabilities in mainstream interscholastic athletic programs, defines what true equal treatment of student athletes with disabilities means, and urges schools to create adapted interscholastic athletic programs for students with disabilities. The OCR Dear Colleague Letter helps clarify the existing regulations and statue under the Rehabilitation Act of 1973 (Rehab Act) to provide interscholastic, club, and intramural athletics for students with disabilities. The Rehab Act protects the rights of students with disabilities from discrimination in educational programs and activities in colleges and universities. The Rehab Act requires that students with disabilities be provided equal opportunity for participation in interscholastic, club, and intramural athletic programs offered by a school. -
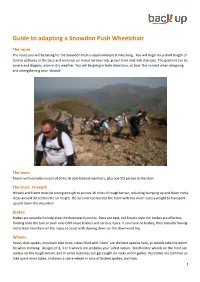
Guide to Adapting a Snowdon Push Wheelchair
Guide to adapting a Snowdon Push Wheelchair The route The route you will be taking for the Snowdon Push is approximately 8 miles long. You will begin on a short length of tarmac pathway at the base and continue on mixed narrow rock, gravel track and rock staircase. The gradient can be severe and slippery, even in dry weather. You will be going in both directions, so bear this in mind when designing and strengthening your ‘chariot’. The team Teams will normally consist of 10 to 16 able-bodied members, plus one SCI person in the chair. The chair: Strength Wheels and frame must be strong enough to survive 16 miles of rough terrain, including bumping up and down rocky steps around 30 centimetre sin height. Be sure not too burden the team with too much excess weight to transport up and down the mountain. Brakes Brakes are essential to help slow the downward journey. Discs are best, but bicycle style rim brakes are effective. Holding onto the tyre or push rims CAN cause blisters and serious injury. If you have no brakes, then consider having more team members on the ropes to assist with slowing down on the downward trip. Wheels Heavy duty spokes, mountain bike tyres, tubes filled with ‘slime’ are the best options here, as wheels take the worst hit when climbing. Designs of 2, 3 or 4 wheels are probably your safest option. Small castor wheels on the front are useless on the rough terrain, and in some instances can get caught on rocks and in gullies. -
Cycling Without Age Quantitative and Qualitative Study
CIVIL MONEY PENALTY (CMP) FUNDED PROJECT REPORT Grantee Miravida Living Campus 225 North Eagle Street Oshkosh, WI 54902 Project Title Cycling Without Age Quantitative and Qualitative Study Award Amount $67,372 Grant Period December 1, 2016-November 30, 2017 Additional Information and Resources Final Report Manual Cycling Without Age Video Department of Health Services / Division of Quality Assurance Quality Assurance and Improvement Committee This project report has been prepared by the author under a research grant from the Department of Health Services (DHS) Quality Assurance and Improvement Committee. The views expressed in the report/training are personal to the author and do not necessarily reflect the view of the Department of Health Services or any of its staff and do not bind the Department in any manner. F-01593A (03/2016) 1 Project: Cycling Without Age Prepared by: P. McNiel DNP, RN, APHN-BC and J. Westphal PhD, RN, NE-BC University of WI Oshkosh School of Nursing For further information and questions, please contact P. McNiel at 920-424-3089 2 Abstract (Project Objective) The purpose of this study is to examine the impact of the Cycling Without Age (CWA) program introduced to enhance the quality of life in persons living in nursing homes on the Miravida Living (ML) campus. Program participants will spend more time outdoors, enjoy touring the community in rickshaws, and develop intergenerational relationships with their pilots (rickshaw drivers). The CWA program will help to dispel uninformed beliefs held by individuals not familiar with elders and nursing home life. It will strengthen ties between nursing home residents and the greater community. -

Types of Wheelchairs
APPENDIX Types of Wheelchairs Reprinted from Wheelchairs: A Prescription Guide, by A. Bennett Wilson, Jr . and Samuel R. McFarland. Charlottesville, VA: Rehabilitation Press, 6-18, 44-46, 1986. THE BASIC WHEELCHAIR floor vary with the width approximately as shown in Table 1. he configuration and dimensions of the adult Selection of the proper seat width is impor- Tbasic chair are shown in Figure 10. The dimen- tant to comfort and stability . A seat too narrow sions and components that must be specified in a is not only uncomfortable, but access to the chair prescription of a wheelchair are: is made difficult. Furthermore, the chances of pressure sores developing is increased. A seat that is Seat: Dimensions, type too wide encourages the user to lean toward one Back: Dimensions, type side, thus promoting scoliosis and increased pressure Arms: Type, dimensions, in some cases over the buttocks on one side . In addition, a seat Footrest: Type wider than is necessary makes propulsion more Legrest : Type difficult. Wheels and Tires: Type and size of wheel, type and A seat that is too shallow reduces the area in size of tire, type of driving rim contact with the seat and causes more pressure on Casters : Type and size the soft tissues in contact with the seat than is necessary. Furthermore, the footrests do not sup- Other considerations are weight, amount and port the feet and legs properly, and balance of the type of use expected, upholstery material and color, user is affected. and seating inserts. A seat that is too deep, or longer than it should be, can restrict circulation in the legs, and causes the Seat Width and Depth patient either to sit with his legs extended or to slide Chairs are regularly available in widths ranging forward in the chair. -

Nordic Sit Ski Instructor Manual
aralym p p A ic S s u n o g r i n d i c s k i Sit Ski Instructor Manual mpics ly a r a g p n i A i S k u s i c n o r d TABLE OF CONTENTS Pg 1. Overview Pg 2. Guiding Principles of Successful Teaching Pg 3. Chapter 1 Student Assessment Pg 5. Chapter 2 Equipment & Fit Pg 11. Chapter 3 Terrain & Environment Pg 12. Chapter 4 Assistance Pg 14. Chapter 5 Teaching Sit Skiing Pg 15. Getting Started Pg 16. Double Poling & Braking Pg 17. Falling & Getting Up Pg 18. Turning & Maneuvering Pg 20. Negotiating Tracks Pg 21. Uphills Pg 21. Sidehills Pg 23. Downhills Pg 24. Conclusion Pg 25. Appendices Photo Credits: Jenny White, Kristina Trygstad-Saari, Eileen Carey 1. OVERVIEW Adaptive sports are sports that are adapted in some way to better support individuals with intellectual or physical impairments. These adaptations can include differences in equipment, technique, or teaching techniques. Cross-country skiing (also called Nordic skiing) is a wonderful option for people with disabilities who enjoy exploring trails or engaging in physical activity in winter environments. Some people pursue Nordic skiing for the peace and solitude, some like the fitness that comes with practice of the sport, and others en- joy pushing their bodies to the physical limit. Sit skiing is a great way for people with spinal cord injuries (SCIs), leg amputations or injuries, or mobility impairments to enjoy the sport of cross-country skiing. As with other snow sports, the teaching progression for skiers with disabilities has evolved as instructors and students explore different and innovative approaches.