Responding to NCD, Gender, and Ethnicity in Trinidad and Tobago
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

By Philip R. Woodside U.S. Geological Survey Open-File Report 8L This
UNITED STATES DEPARTMENT OF THE INTERIOR GEOLOGICAL SURVEY THE PETROLEUM GEOLOGY OF TRINIDAD AND TOBAGO By Philip R. Woodside U.S. Geological Survey Open-File Report 8l This report is preliminary and has not been reviewed for conformity with U.S. Geological Survey editorial standards and stratigraphic nomenclature* Any use of trade names is for descriptive purposes only and does not imply endorsment by the USGS. 1981 CONTENTS Page For ewo r d •————————•———-————————————————•————————•—•————•—— Abstract —• Introduction ——————————————————————————————————————————— 1 Structural Geology ————•—-———————•———•—•—————-———•—•——•—— 4 Introduction -——————————————————————————————————————— 4 Structural Areas of Trinidad ——————————————————————————— 5 The Northern Range ——————————•—————————————————————— 5 The Northern (Caroni) Basin —————————————————————————— 6 The Central Range ————————————————————————————————— 6 The Southern Basin (including Naparima Thrust Belt) ———————— 6 Los Bajos fault ———————————————————————————————— 7 The Southern Range ————————————————————————————————— 9 Shale Diapirs ———————————————————————————————————— 10 Stratigraphy ——————————————————————————————————————————— 11 Northern Range and Northern Basin ——————————————————————— 11 Central Range —————————————————————————————————————— 12 Southern Basin and Southern Range —————-————————————————— 14 Suimnary ————————————————————————————————————————————— 18 Oil and Gas Occurrence ———•——————————•——-——————•————-—•—•— 19 Introduction ————•—•————————————————————————-—— 19 Hydrocarbon Considerations -

Health and Climate Change: Country Profile 2020
TRINIDAD AND TOBAGO HEALTH & CLIMATE CHANGE COUNTRY PROFILE 2020 Small Island Developing States Initiative CONTENTS 1 EXECUTIVE SUMMARY 2 KEY RECOMMENDATIONS 3 BACKGROUND 4 CLIMATE HAZARDS RELEVANT FOR HEALTH 7 HEALTH IMPACTS OF CLIMATE CHANGE 9 HEALTH VULNERABILITY AND ADAPTIVE CAPACITY 11 HEALTH SECTOR RESPONSE: MEASURING PROGRESS Acknowledgements This document was developed in collaboration with the Ministry of Health and the Ministry of Planning and Development, who together with the World Health Organization (WHO), the Pan American Health Organization (PAHO), and the United Nations Framework Convention on Climate Change (UNFCCC) gratefully acknowledge the technical contributions of Mr Arnold Ramkaran, Dr Roshan Parasram, Mr Lawrence Jaisingh and Mr Kishan Kumarsingh. Financial support for this project was provided by the Norwegian Agency for Development Cooperation (NORAD). ii Health and Climate Change Country Profile “Many of the public health gains we have made in recent decades are at risk due to the direct and indirect impacts of climate variability and climate change.” EXECUTIVE SUMMARY Despite producing very little greenhouse gas policies, building resilience must happen in emissions that cause climate change, people parallel with the reduction of carbon emissions living in small island developing States (SIDS) by countries around the world. are on the frontline of climate change impacts. The WHO Special Initiative on Climate Change These countries face a range of acute to long- and Health in SIDS aims to provide national term risks, including extreme weather events health authorities in SIDS with the political, such as floods, droughts and cyclones, increased technical and financial support required to better average temperatures and rising sea levels. -

Education in Trinidad and Tobago
An Overview of The Educational System of Trinidad & Tobago American & Caribbean Law Initiative Fall 2008 Introduction to Trinidad and Tobago Located 7 mile off the coast of Venezuela The Republic of Trinidad and Tobago has a population of approximately 1.3 million inhabitants Majority of the population is located in Trinidad with about 50,000 inhabitants on the smaller island of Tobago Ruled by the British, Trinidad and Tobago gained independence in 1962 and declared itself a republic in 1976 The economy is largely based on the country’s abundance of natural resources, particularly Oil and Gas. Introduction to Trinidad and Tobago The country has a stable government and considers itself to be a leading political and economic power in the Caribbean. The total GDP in 2005 was approximately 14 million USD Literacy rate is 98.6- highest in the Caribbean The official language is English with French, Chinese, Spanish and the Caribbean Hindustani, a dialect of Hindi also spoken Map of Trinidad and Tobago Education System Based on British Model Education is free and compulsory for children ages 5 to 13 years of age Education System divided into 3 phases: Primary Education Secondary Education Higher Education Higher Education Higher Education is post-secondary study leading to diploma, certificates and degrees Two major higher education institutions: University of West Indies National Institute for Higher Education Primary Education Primary consists of 2 preparatory ("infant") grades and 5 "standard" grades Includes children -

Microtityus Rickyi (Dwarf Scorpion)
UWI The Online Guide to the Animals of Trinidad and Tobago Diversity Microtityus rickyi (Dwarf Scorpion) Order: Scorpiones (Scorpions) Class: Arachnida (Spiders, Scorpions and Mites) Phylum: Arthropoda (Arthropods) Fig. 1. Dwarf scorpion, Microtityus rickyi. [www.ntnu.no/ub/scorpion-files/m_rickyi2.jpg, downloaded 23 October 2016] TRAITS. Microtityus rickyi are the smallest scorpions of the Western Hemisphere with an average size of 19mm. A light yellow pigmentation with black to light brown spots is found throughout the carapace (anterior plate that covers the head and thorax) and opisthosoma (segmented mid-body and tail). Its stinger is dark brown. The almost triangular carapace with a distinctly notched margin is characteristic of Microtiyus rickyi (Fig. 1). Sexual dimorphism is exhibited in regards to their size; the largest females are 18.6mm and males 16.6mm (Kjellesvig- Waering, 1966) DISTRIBUTION. Microtityus rickyi are endemic to Trinidad and Tobago, found nowhere else, and rather rare, comprising less than 1% of the scorpion population sampled (Kjellesvig- UWI The Online Guide to the Animals of Trinidad and Tobago Diversity Waering, 1966). Microtityus rickyi can be found at Lady Chancellor Hill, Mt. St. Benedict, Chacachacare Island, Gaspar Grande Island (Fig. 2), and Speyside Tobago (Prendini, 2001). HABITAT AND ACTIVITY. Microtityus rickyi are predominantly found hanging motionless on the underside of rocks within forests, on exposed soil banks or leaf litter though some have been found near the coast and on hills at heights of 200m. They can also be considered as semi- arboreal as some have been found a few metres up tree trunks (Prendini, 2001). FOOD AND FEEDING. -

Trinidad and Tobago: Venezuelan Refugees at Risk
First UA: 126/20 AMR 49/2953/2020 Trinidad and Tobago Date: 13 August 2020 URGENT ACTION VENEZUELAN REFUGEES AT RISK At least 165 Venezuelans have been deported by Trinidad and Tobago in recent weeks. Pushing a xenophobic narrative targeting Venezuelans and associating them with COVID-19, the government announced it will deport Venezuelans who have “entered illegally” and those with legal residency found to be helping them. This fuels a climate of fear which risks pushing people underground and away from health services. We are calling on Trinidad and Tobago to refrain from deporting people in search of protection and to work with partners to find human rights-based solutions for them. TAKE ACTION: WRITE AN APPEAL IN YOUR OWN WORDS OR USE THIS MODEL LETTER The Honourable Dr Keith Rowley Prime Minister of Trinidad and Tobago 13-15 St Clair Avenue Port of Spain, Trinidad and Tobago Phone number: +1 (868) 622-1625 Emails: [email protected]; [email protected]; Dear Prime Minister, I write to you with deep concern over reports that at least 165 Venezuelans were deported from Trinidad and Tobago to their country in recent weeks. Trinidad and Tobago must guarantee and protect the rights of refugees and people seeking international protection. Millions of Venezuelans are fleeing an unprecedented human rights crisis in their country. They need a life jacket, not to be sent back to a country where they may face torture or other grave human rights violations. Instead, Venezuelan refugees and those who support them are targeted by xenophobic narratives and accusations of increasing the risks of COVID-19 for Trinidad and Tobago people, justifying procedures of deportation without properly assess the danger that those returned may face in Venezuela. -

The Journey That Is Chacachacare - Part 1/3 a Personal Account by Hans E.A.Boos
Quarterly Bulletin of the Trinidad and Tobago Field Naturalists’ Club January - March 2010 Issue No: 1/2010 The journey that is Chacachacare - part 1/3 A personal account by Hans E.A.Boos Several years ago I was asked, by Yasmin Comeau of the National Herbarium, U.W.I St. Augustine to write a short history titled “Human occupation and impact on the island of Chacachacare‖ ( which constitutes the main body of the account below), which was to be a part of a larger work on the vegetation of the island of Chacachacare. But, in that I do not know if it was ever published in any part or its entirety, I thought I would share it, and some more recent additions and observations, with the members of the Trinidad and Tobago Field Naturalists‘ Club, a club of which I have been proud to be a member since the middle of 1960. Chacachacare holds a special place in my interest, which interest will A part of the Leper colony be elaborated on below, and which was again sparked during a recent Photo Hans E. A. Boos excursion of the Club to this island on Sunday March 28th 2010. (Continued on page 3) Page 2 THE FIELD NATURALIST Issue No. 1/2010 Inside This Issue Quarterly Bulletin of the Trinidad and Tobago Field Naturalists’ Club 1 Cover January - March 2010 The Journey that is Chacachacare - A personal account by Hans E. A. Boos Editor Shane T. Ballah 7 Club Monthly Field Trip Report Editorial Committee La Table 31- 01 - 2010 Palaash Narase, Reginald Potter - Reginald Potter Contributing writers Christopher K. -
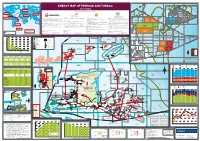
View the Energy Map of Trinidad and Tobago, 2017 Edition
Trinidad and Tobago LNG export destinations 2015 (million m3 of LNG) Trinidad and Tobago deepwater area for development 60°W 59°W 58°W Trinidad and Tobago territorial waters ENERGY MAP OF TRINIDAD AND TOBAGO 1000 2000 m m 2017 edition GRENADA BARBADOS Trinidad and Tobago 2000m LNG to Europe A tlantic Ocean 2.91 million m3 LNG A TLANTIC Caribbean 2000m 20 Produced by Petroleum Economist, in association with 00 O CEAN EUROPE Sea m Trinidad and Tobago 2000m LNG to North America NORTH AMERICA Trinidad and Tobago 5.69 million m3 LNG LNG to Asia 3 GO TTDAA 30 TTDAA 31 TTDAA 32 BA 1.02 million m LNG TO Trinidad and Tobago OPEN OPEN OPEN 12°N LNG to MENA 3 1.90 million m LNG ASIA Trinidad and Tobago CARIBBEAN TRINIDAD AND TOBAGO 2000m LNG to Caribbean Atlantic LNG Company profile Company Profile Company profile Company Profile 3 Established by the Government of Trinidad and Tobago in August 1975, The National Gas Company of Trinidad and Tobago Limited (NGC) is an BHP Billiton is a leading global resources company with a Petroleum Business that includes exploration, development, production and marketing Shell has been in Trinidad and Tobago for over 100 years and has played a major role in the development of its oil and gas industry. Petroleum Company of Trinidad and Tobago Limited (Petrotrin) is an integrated Oil and Gas Company engaged in the full range of petroleum 3.84 million m LNG internationally investment-graded company that is strategically positioned in the midstream of the natural gas value chain. -

THE HAMMER the Quarterly Magazine of the Geological Society of Trinidad and Tobago I June 2014
THE HAMMER The Quarterly Magazine of the Geological Society of Trinidad and Tobago I June 2014 GSTT STRATIGRAPHIC WORKSHOPS Hasley Vincent captures the ongoing discussions SEISMIC REPROCESSING IMPROVES PSTM IMAGING A case study by Terrell Dhanpaul and Samuel Ragbir ALL ABOARD FOR SOLDADO ROCK! Lidia Harripersad recounts this southwestern adventureJUNE 2014 I The HAMMER is the fellowship magazine IN THIS ISSUE of the Geological Society of Trinidad and Tobago. June 2014 The Geological Society of Trinidad and Tobago UTT Building, Esperanza Road Brechin Castle, Couva T: +868 679 6064 F: +868 679 6064 W: www.thegstt.com E: [email protected] Editor Keisha Fletcher The Executive of the Geological Society of Trinidad and Tobago (2013-2014) Mr. Xavier Moonan (President); Dr. Krishna Persad (President Elect); Mr. Sisnarine Seegobin (Treasurer); Ms. Nicholette Camps (Assistant Treasurer) Mrs. Helena Inniss-King (Immediate Past President); COVER STORY : ALL ABOARD FOR SOLDADO Mr. Ariel Thomas (Director); Mr. Veshash Singh (Director); ROCK! Mr. Anderson Arjoon (Director); Professor Brent Wilson (Director) Lidia Harripersad shares her experience on this field trip The Geological Society of Trinidad and Tobago accepts no responsibility for the views expressed in any article in this publication. All views expressed, except where explicitly stated otherwise, represent those of the author, and not those of the Geological Society of Trinidad and Tobago. All rights reserved. No paragraph of this publication may be reproduced, copied or transmitted save with written permission. Every effort has been made to trace copyright holders of material in this publication. If any rights have been omitted, the publishers offer their apologies. -

Crossing the Galleons' Passage
Journal of Caribbean Archaeology Copyright 2010 ISSN 1524-4776 CROSSING THE GALLEONS’ PASSAGE: AMERINDIAN INTERACTION AND CULTURAL (DIS)UNITY BETWEEN TRINIDAD AND TOBAGO Arie Boomert Faculty of Archaeology Leiden University P.O. Box 9515 2300 RA Leiden The Netherlands [email protected] Abstract The islands of Trinidad and Tobago formed separate sociopolitical, economic, and cultural entities throughout most of their colonial history. This situation was prefigured by the two islands’ prehistoric past following the Saladoid epoch of pan-Caribbean cultural unity. The Saladoid convergence disintegrated rapidly after the establishment of the Arauquinoid series in Trinidad by about AD 700/800 as simultaneously Tobago appears to have been drawn into the Troumassoid interaction sphere of the Windward Islands and Barbados. This paper discusses the patterns of Amerindian interaction and communication across the Galleons’ Passage between Trinidad and Tobago during Ceramic times and attempts to appreciate the post-Saladoid cultural realignment of the two islands and its consequences. Résumé Durant la majeure partie de leur histoire coloniale, les îles de la Trinité et de Tobago ont formé des entités sociopolitiques, économiques et culturelles séparées. Le passé préhistori- que de ces deux îles, après la période d’unité culturelle saladoïde de l’espace caribéen, pré- figurait déjà cette distinction. L’unité culturelle saladoïde s’est rapidement désagrégée après l’émergence de la série arauquinoïde à la Trinité vers 700-800 ap. J.-C., au moment même où Tobago semble avoir été tirée dans la sphère d’interaction troumassoïde des Îles du Vent et de la Barbade. Cet article traite des modes d’interaction et de communication amérindiens à travers le Passage des Galions, entre la Trinité et Tobago, durant l’époque céramique et tente de prendre la mesure du réalignement culturel des deux îles à l’époque post-saladoïde et de ses conséquences. -

Field Trip Guide a Visit to Chacachacare to Examine Outcrops of the Maraval
Field Guides of the Geological Society of Trinidad and Tobago FIELD TRIP GUIDE A VISIT TO CHACACHACARE TO EXAMINE OUTCROPS OF THE MARAVAL AND CHANCELLOR FORMATIONS LEADER CURTIS ARCHIE Saturday 31ST. JANUARY 2004 THE GEOLOGICAL SOCIETY OF TRINIDAD AND TOBAGO Field Guides of the Geological Society of Trinidad and Tobago A SYNOPSIS OF THE GEOLOGY WESTERN END OF THE NORTHERN RANGE The Northern Range of Trinidad is an east – west trending exposure of subgreenschist to lower greenschist grade metasedimentary rocks (Frey et. Al. 1988) located in the Caribbean-South American plate boundary zone. The rocks are predominantly slates, schists, metaquartzites and metacarbonates. The protoliths from which these rocks were derived are interpreted to have been deposited on a north facing passive margin along northern South America (Pindell 1985, Speed 1985). Relict fossils from scattered indicate Tithonian to Maastrichtian protolith depositional ages. Ar40 / Ar39 ages from white micas indicate mid-Tertiary (25Ma) metamorphism, which was likely synkinematic with the South American – Caribbean plate transpression. These metasedimentary rocks were then exhumed and uplifted during the Neogene. Field Guides of the Geological Society of Trinidad and Tobago The structure of the Northern Range varies along its length but on the whole the oldest rocks, Maraval and Maracas formations, occupy the central spine of the range, while younger rocks outcrop along the north and south flanks. In the western peninsula from Port of Spain to Chacachacare the structure that of a single north vergent overturned anticline trending East-West (Potter 1963), The fold appears to plunge gently westward as shown by the narrowing and then disappearance of the Maraval limestone core. -

Imagine All the People” Is a Series of Publications Pro- Duced by the Boston Redevelopment Authority for the People Mayor’S Office of Immigrant Advancement
imagine Trinidadians in Boston all the “imagine all the people” is a series of publications pro- duced by the Boston Redevelopment Authority for the Mayor’s Office of Immigrant Advancement. The series people provides a comprehensive profile of Boston’s diverse immigrant communities and their numerous contribu- tions to the city’s social, cultural and economic land- scape. It is part of an ongoing effort to celebrate immi- grants and gain insight into how they shape our city. Trinidadian-American Haseeb Hosein is first Muslim Boston Police Department captain Boston EMS at Caribbean Parade in Dorchester, photo: Jeremiah Robinson Trinidadians CITY OF BOSTON Martin J. Walsh Mayor 2016 Trinidad and Tobago is a twin island nation in the Caribbean that gained its political independence from England in 1962. The islands were originally colo- nized by the Spanish who first imported African slave labor to work in sugar plantations. After slavery was abolished, migrant workers from India were re- cruited to work in the sugar industry. During the 20th century, petroleum re- place sugar as the leading export from Trinidad. With a population of 1.3 million in 2015, this petroleum rich country has one of the highest per capita GDPs in the western hemisphere.1 Even with this strong economy, Trinidad and Tobago experienced a negative net migration rate and population decline in 2015. The United States, Canada and the United Kingdom are the leading destina- tions of Trinidadian and Tobagonian migration.2 Massachusetts has the eighth largest share (3 percent) of the 220,2343 foreign-born Trinidadian and Tobago- nians living in the United States in 2014. -

Bridget Brereton Contesting the Past: Narratives Of
BRIDGET BRERETON CONTESTING THE PAST: NARRATIVES OF TRINIDAD & TOBAGO HISTORY INTRODUCTION Historians and social scientists agree that nationalisms and national identities, ethnicities and ethnic identities, are all constructed or “invented” at specific historical conjunctures, and that the creation of narratives about the past is nearly always an important aspect of this process. The recent (June 2006) dec- laration by the Florida state legislature – that American history as taught in the state’s schools “shall be viewed as factual, not as constructed ... and shall be defined as the creation of a new nation based largely on the universal principles stated in the Declaration of Independence” – thus flies in the face of decades of academic consensus about how “history” is written. Every past, every claim to truth about the past, is open to interpretation. As Barry Schwartz (quoted in Johnson 2003:7) has put it, “recollecting the past is an active constructive process, not a simple matter of retrieving information. To remember is to place a part of the past in the service of conceptions and needs of the present.” All postcolonial states, in particular, have undergone a process of national self- creation, a process of identity formation involving “a recasting of history to produce a usable past” as Howard Johnson (2003:) has said of Jamaica. Nationalisms are invented, and their claims to historical continuity are always expressions of ideological and political concerns, and this is equally true of the construction of ethnicities and ethnic narratives. “Nations are imaginary constructs that depend for their existence on an apparatus of cultural fictions,” writes Timothy Brennan (990:49).