Making Cities Work: Policies and Programmes in India
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

International Public Health Hazards: Indian Legislative Provisions
“International public health hazards: Indian legislative provisions” presents an outline of the provisions in the Indian legal system which may enable the implementation of IHR in the country. International Health Regulations (2005) are International public health hazards: the international legal instrument designed to help protect all countries from the international spread of disease, including public health risks and public health Indian legislative provisions emergencies. The present document is the result of a study taken up for the regional workshop on public health legislation for International Health Regulations, Yangon, Myanmar,” 8–10 April 2013. The relevant Indian legislation in the various Acts and rules that may assist in putting early warning systems in place has been outlined. The document intends to provide a ready reference on Indian legislation to enable establishing an early warning system that could assist the Government to provide health care. ISBN 978-92-9022-476-1 World Health House Indraprastha Estate Mahatma Gandhi Marg New Delhi-110002, India 9 7 8 9 2 9 0 2 2 4 7 6 1 International public health hazards: Indian legislative provisions WHO Library Cataloguing-in-Publication data World Health Organization, Regional Office for South-East Asia. International public health hazards: Indian legislative provisions 1. Health Legislation 2. Public Health 3. National Health Programs I. India. ISBN 978-92-9022-476-1 (NLM classification: W 32) Cover photo: © http://parliamentofindia.nic.in/ © World Health Organization 2015 All rights reserved. Requests for publications, or for permission to reproduce or translate WHO publications – whether for sale or for noncommercial distribution – can be obtained from SEARO Library, World Health Organization, Regional Office for South-East Asia, Indraprastha Estate, Mahatma Gandhi Marg, New Delhi 110 002, India (fax: +91 11 23370197; e-mail: [email protected]). -

India in the Indian Ocean Donald L
Naval War College Review Volume 59 Article 6 Number 2 Spring 2006 India in the Indian Ocean Donald L. Berlin Follow this and additional works at: https://digital-commons.usnwc.edu/nwc-review Recommended Citation Berlin, Donald L. (2006) "India in the Indian Ocean," Naval War College Review: Vol. 59 : No. 2 , Article 6. Available at: https://digital-commons.usnwc.edu/nwc-review/vol59/iss2/6 This Article is brought to you for free and open access by the Journals at U.S. Naval War College Digital Commons. It has been accepted for inclusion in Naval War College Review by an authorized editor of U.S. Naval War College Digital Commons. For more information, please contact [email protected]. Color profile: Generic CMYK printer profile Composite Default screen Berlin: India in the Indian Ocean INDIA IN THE INDIAN OCEAN Donald L. Berlin ne of the key milestones in world history has been the rise to prominence Oof new and influential states in world affairs. The recent trajectories of China and India suggest strongly that these states will play a more powerful role in the world in the coming decades.1 One recent analysis, for example, judges that “the likely emergence of China and India ...asnewglobal players—similar to the advent of a united Germany in the 19th century and a powerful United States in the early 20th century—will transform the geopolitical landscape, with impacts potentially as dramatic as those in the two previous centuries.”2 India’s rise, of course, has been heralded before—perhaps prematurely. How- ever, its ascent now seems assured in light of changes in India’s economic and political mind-set, especially the advent of better economic policies and a diplo- macy emphasizing realism. -

Paper-20 Urban Sociology
MA SOCIOLOGY P-20 URBAN SOCIOLOGY Author Dr. P.K.Kar 1 Unit-I: Evolution of Cities in History based on Major Functions:Growth of Urbanization in India, City type and functions in India, The Rural-Urban dichotomy and continum in India and Theories of Unrbanization Unit-II:Social Institutions in the Urban Milieu:Family and Marriage Caste, Religion, Economy, Polity Unit-III: The new Social Structures in Urban India:Informal Sector: Various Occupations , Formal Sector: Various Professions and Secondary Institutions: Educational, Leisure and Recreation, Voluntary Organizations. Unit-IV: Problems of Urban India: Housing, Transport, Communication, Pollution, Sanitation, And Crime. UNIT-I Evolution of Cities in History based on Major Functions: CONTENTS 1.0. OBJECTIVES 1.1. EVOLUTION OF CITIES IN HISTORY BASED ON FUCTIONS 1.1.1 Ancient Cities 1.1.2 Medieval cities 1.1.3 Modern Cities 1.1.4 Pre-lndustrial Cities 1.1.5 Industrial Cities 1.2. GROWTH OF URBANIZATION IN INDIA 1.3. REGIONAL URBANISATION PROCESS: 1.4. FORMATION OF URBAN AGGLOMERATION 2 1.5. TRENDS AND PATTERNS OF URBANIZATION IN INDIA 1.5.1 Demographic approach 1.5.2 Geographic approach 1.6. URBAN ECONOMIC GROWTH 1.6.1. Size of total NDP by sectors and per capita NDP 1.7. COMPOUND ANNUAL GROWTH 1.8. CITY TYPE AND FUCTIONS IN INDIA 1.9. RURAL URBAN DICHOTOMY AND CONTINUUM 1.10. DISTINCTION BETWEEN RURAL AND URBAN COMMUNITIES 1.11. THEORIES OF URBAN GROWTH 1.11.1. Concentric zone model 1.11.2. Sectors model 1.11.3. Multiple nuclei model 1.11.4. -

Expectant Urbanism Time, Space and Rhythm in A
EXPECTANT URBANISM TIME, SPACE AND RHYTHM IN A SMALLER SOUTH INDIAN CITY by Ian M. Cook Submitted to Central European University Department of Sociology and Social Anthropology In partial fulfilment of the requirements for the degree of Doctor of Philosophy Supervisors: Professor Daniel Monterescu CEU eTD Collection Professor Vlad Naumescu Budapest, Hungary 2015 Statement I hereby state that the thesis contains no material accepted for any other degrees in any other institutions. The thesis contains no materials previously written and/or published by another person, except where appropriate acknowledgment is made in the form of bibliographical reference. Budapest, November, 2015 CEU eTD Collection Abstract Even more intense than India's ongoing urbanisation is the expectancy surrounding it. Freed from exploitative colonial rule and failed 'socialist' development, it is loudly proclaimed that India is having an 'urban awakening' that coincides with its 'unbound' and 'shining' 'arrival to the global stage'. This expectancy is keenly felt in Mangaluru (formerly Mangalore) – a city of around half a million people in coastal south Karnataka – a city framed as small, but with metropolitan ambitions. This dissertation analyses how Mangaluru's culture of expectancy structures and destructures everyday urban life. Starting from a movement and experience based understanding of the urban, and drawing on 18 months ethnographic research amongst housing brokers, moving street vendors and auto rickshaw drivers, the dissertation interrogates the interplay between the city's regularities and irregularities through the analytical lens of rhythm. Expectancy not only engenders violent land grabs, slum clearances and the creation of exclusive residential enclaves, but also myriad individual and collective aspirations in, with, and through the city – future wants for which people engage in often hard routinised labour in the present. -

Distributive Justice and the Sustainable Development Goals: Delivering Agenda 2030 in India
Law and Development Review 2019; aop Nandini Ramanujam*, Nicholas Caivano and Alexander Agnello Distributive Justice and the Sustainable Development Goals: Delivering Agenda 2030 in India https://doi.org/10.1515/ldr-2019-0020 Abstract: The sustainable development goals (SDGs) present a real opportunity to direct India towards a path of equality and equity. This article posits that India’s plans to achieve the millennium development goals by the end of their term in 2015 faltered because reforms designed to alleviate poverty and achieve equitable growth did not adequately address weaknesses in institutions of accountability, which undermined the reform agenda. These institutions, which include Parliament and the judiciary, exist in part to ensure that actions taken by public officials are subject to oversight so that government initiatives meet their stated objectives. As India shifts its attention to Agenda 2030, its renewed commitment to institutional reforms represents an occasion for the state to address the inequalities in income and the resulting human develop- ment concerns. For the government to achieve the SDGs, this article suggests that India must integrate what we refer to as a baseline conception of distribu- tive justice within its plans, which can account for structural barriers to its development arising from ineffective institutions of accountability and provide the poor with a route towards individual empowerment. Keywords: India, SDGs, international development, institutions, inequality, distributive justice 1 Introduction -
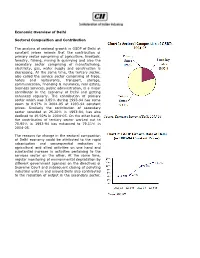
Economic Overview of Delhi Sectoral Composition and Contribution the Analysis of Sectoral Growth in GSDP of Delhi at Constant Pr
Economic Overview of Delhi Sectoral Composition and Contribution The analysis of sectoral growth in GSDP of Delhi at constant prices reveals that the contribution of primary sector comprising of agriculture, livestock, forestry, fishing, mining & quarrying and also the secondary sector comprising of manufacturing, electricity, gas, water supply and construction is decreasing. At the same time, the tertiary sector, also called the service sector comprising of trade, hotels and restaurants, transport, storage, communication, financing & insurance, real estate, business services, public administration, is a major contributor in the economy of Delhi and getting enhanced regularly. The contribution of primary sector which was 3.85% during 1993-94 has come down to 0.97% in 2004-05 at 1993-94 constant prices. Similarly the contribution of secondary sector recorded at 25.20% in 1993-94, has also declined to 19.92% in 2004-05. On the other hand, the contribution of tertiary sector worked out to 70.95% in 1993-94 has enhanced to 79.11% in 2004-05. The reasons for change in the sectoral composition of Delhi economy could be attributed to the rapid urbanisation and consequential reduction in agricultural and allied activities on one hand and substantial increase in activities pertaining to the services sector on the other. At the same time, regular monitoring of environmental degradation by different government agencies on the directives of Supreme Court and subsequent closing of polluting industrial units in and around Delhi also contributed to the reduction of output in the secondary sector. Delhi's service sector has expanded due in part to the large skilled English-speaking workforce that has attracted many multinational companies. -

Central University of Punjab, Bathinda, Punjab
Central University of Punjab, Bathinda, Punjab Course Scheme For M.A. (History) 1 CENTRE FOR SOUTH AND CENTRAL ASIAN STUDIES (Including Historical Studies) Course structure-M.A. IN HISTORY % Weightage Semester I Marks Paper Course Title L T P Cr A B C D E Code HST. 501 Research F 4 0 0 4 25 25 25 25 100 Methodology HST. 503 Indian Political C 4 0 0 4 25 25 25 25 100 Thought HST. 504 Pre-History and C 4 0 0 4 25 25 25 25 100 Proto-History of India HST. 505 Ancient India C 4 0 0 4 25 25 25 25 100 (600BCE-300CE) HST. XXX Elective Course I E* 4 0 0 4 25 25 25 25 100 IDC. XXX Inter- E 2 0 0 2 15 10 10 15 50 Disciplinary/Open (O)** Elective HST. 599 Seminar C 0 0 0 2 15 10 10 15 50 TOTAL SEM I - 24 24 - 600 Elective Courses (Opt any one courses within the department) HST. 511 Art and Architecture E* 4 0 0 4 25 25 25 25 100 of Ancient India HST. 512 Early State and E* 4 0 0 4 25 25 25 25 100 Society in Ancient India Interdisciplinary Course/Open Elective Offered (For other Centers) HST. 521 Harrappan E 2 0 0 2 15 10 10 15 50 Civilization (O)** HST. 522 Religion in Ancient E 2 0 0 2 15 10 10 15 50 India (O)** 2 Semester II % Weightage Marks Paper Course Title L T P Cr A B C D E Code HST. -

Rural-Urban Linkages : India Case Study
WORKING PAPER SERIES Document Nº 124 Working Group: Development with Territorial Cohesion Rural-Urban Linkages: India Case Study Eric Denis and Marie - Hélène Zérah October, 2014 This document is a product of a Rimisp initiative funded by The Ford Foundation. We authorize the non-for-profit partial or full reproduction and dissemination of this document, subject to the source being properly acknowledged. Citation: Denis E. and Zérah M.H., 2014. Rural-Urban Linkages: India Case Study. Working Paper Series Nº 124. Working Group: Development with Territorial Cohesion. Territorial Cohesion for Development Program. Rimisp, Santiago, Chile. Authors: Eric Denis, Géographie-cités Research Centre, Centre national de la recherche scientifique (CNRS) and Paris Panthéon-Sorbonne University, France. Marie - Hélène Zérah, Centre d’Études en Sciences Sociales sur les Mondes Africains, Américains et Asiatiques (CESSMA), Institut de Recherche pour le Développement (IRD), France. Rimisp in Latin America (www.rimisp.org) Chile: Huelén 10, Piso 6, Providencia, Santiago, Región Metropolitana | Tel. +(56-2)2 236 45 57 / Fax +(56-2) 2236 45 58 Ecuador: Av. Shyris N32-218 y Av. Eloy Alfaro, Edificio Parque Central, Oficina 610, Quito | Tel.+(593 2) 3823916 / 3823882 México: Yosemite 13 Colonia Nápoles Delegación Benito Juárez, México, Distrito Federal | Tel/Fax +(52) 55 5096 6592 INDEX 1. INTRODUCTION ...................................................................................................... 4 2. DEFINITIONS .......................................................................................................... -
Domestic Labour Relations in India Vulnerability and Gendered Life Courses in Jaipur
Domestic labour relations in India Vulnerability and gendered life courses in Jaipur Päivi Mattila Interkont Books 19 Helsinki 2011 Domestic labour relations in India Vulnerability and gendered life courses in Jaipur Päivi Mattila Doctoral Dissertation To be presented for public examination with the permission of the Faculty of Social Sciences in the Small Festive Hall, Main Building of the University of Helsinki on Saturday, October 8, 2011 at 10 a.m. University of Helsinki, Faculty of Social Sciences Department of Political and Economic Studies, Development Studies Interkont Books 19 opponent Dr. Bipasha Baruah, Associate Professor International Studies, California State University, Long Beach pre-examiners Dr. Bipasha Baruah, Associate Professor International Studies, California State University, Long Beach Adjunct Professor Raija Julkunen University of Jyväskylä supervisors Adjunct Professor Anna Rotkirch University of Helsinki Professor Sirpa Tenhunen Social and Cultural Anthropology, University of Helsinki copyright Päivi Mattila published by Institute of Development Studies University of Helsinki, Finland ISSN 0359-307X (Interkont Books 19) ISBN 978-952-10-7247-5 (Paperback) ISBN 978-952-10-7248-2 (PDF; http://e-thesis.helsinki.fi) graphic design Miina Blot | Livadia printed by Unigrafia, Helsinki 2011 CONTENTS Abstract i Acknowledgements iii 1 Introduction 1 1.1 Research task and relevance 2 1.2 The scope and scale of paid domestic work in India 7 From colonial times to contemporary practices 7 Regulation of domestic work 11 Gender -

City Characteristics, Migration, and Urban Development Policies in India
Papers of the East-West Population Institute No. 92 City characteristics, migration, and urban development policies in India Mahendra K. Premi with Judith Ann L. Tom East-West Center Honolulu, Hawaii PAPERS OF THE EAST-WEST POPULATION INSTITUTE, published about eight times a year, facilitate early dissemination of research findings and state-of-the-art es• says on the demography of Asia, the Pacific, and the United States. Annual sub• scription rate, $12. NOTE TO CONTRIBUTORS: The Population Institute considers unsolicited as well as commissioned manuscripts for the Paper Series. Appropriate topics are popu• lation estimation and analysis, causes and consequences of demographic behavior, urbanization and population distribution, and population policies and programs. All manuscripts are reviewed. In selecting manuscripts for publication, the Insti• tute considers quality of scholarship and usefulness to public officials and other professionals in the field of population; it "also seeks contributions reflecting di• verse cultural and disciplinary perspectives on population. The series can accom• modate articles not necessarily suited for journals because of unusual length or treatment of subject. All copy must be typed double-spaced. For additional in• formation on manuscript preparation, write to the Publications Office of the Center. OTHER SERIAL PUBLICATIONS OF THE EAST-WEST POPULATION INSTITUTE: Working Papers are circulated for comment and to inform interested colleagues about work in progress at the East-West Population Institute. They are intended to complement evidence of completed work as reflected in Papers of the East- West Population Institute and the Reprint Series. $1 per copy. Reprint Series brings selected articles originating from Institute research but pub• lished elsewhere to the attention of population specialists who might not other• wise see them. -

Neoliberalizing the Streets of Urban India: Engagements of a Free Market Think Tank in the Politics of Street Hawking
University of Kentucky UKnowledge Theses and Dissertations--Geography Geography 2013 NEOLIBERALIZING THE STREETS OF URBAN INDIA: ENGAGEMENTS OF A FREE MARKET THINK TANK IN THE POLITICS OF STREET HAWKING Priyanka Jain University of Kentucky, [email protected] Right click to open a feedback form in a new tab to let us know how this document benefits ou.y Recommended Citation Jain, Priyanka, "NEOLIBERALIZING THE STREETS OF URBAN INDIA: ENGAGEMENTS OF A FREE MARKET THINK TANK IN THE POLITICS OF STREET HAWKING" (2013). Theses and Dissertations--Geography. 14. https://uknowledge.uky.edu/geography_etds/14 This Doctoral Dissertation is brought to you for free and open access by the Geography at UKnowledge. It has been accepted for inclusion in Theses and Dissertations--Geography by an authorized administrator of UKnowledge. For more information, please contact [email protected]. STUDENT AGREEMENT: I represent that my thesis or dissertation and abstract are my original work. Proper attribution has been given to all outside sources. I understand that I am solely responsible for obtaining any needed copyright permissions. I have obtained and attached hereto needed written permission statements(s) from the owner(s) of each third-party copyrighted matter to be included in my work, allowing electronic distribution (if such use is not permitted by the fair use doctrine). I hereby grant to The University of Kentucky and its agents the non-exclusive license to archive and make accessible my work in whole or in part in all forms of media, now or hereafter known. I agree that the document mentioned above may be made available immediately for worldwide access unless a preapproved embargo applies. -

The Lockdown to Contain the Coronavirus Outbreak Has Disrupted Supply Chains
JOURNALISM OF COURAGE SINCE 1932 The lockdown to contain the coronavirus outbreak has disrupted supply chains. One crucial chain is delivery of information and insight — news and analysis that is fair and accurate and reliably reported from across a nation in quarantine. A voice you can trust amid the clanging of alarm bells. Vajiram & Ravi and The Indian Express are proud to deliver the electronic version of this morning’s edition of The Indian Express to your Inbox. You may follow The Indian Express’s news and analysis through the day on indianexpress.com DAILY FROM: AHMEDABAD, CHANDIGARH, DELHI, JAIPUR, KOLKATA, LUCKNOW, MUMBAI, NAGPUR, PUNE, VADODARA JOURNALISM OF COURAGE SATURDAY, AUGUST 22, 2020, NEW DELHI, LATE CITY, 16 PAGES SINCE 1932 `6.00 (`8 PATNA &RAIPUR, `12 SRINAGAR) WWW.INDIANEXPRESS.COM THE EDITORIAL PAGE OFFICIAL NOTE TO MEA NAGATALKS: BRIDGINGTHE AswithPak, NARRATIVEDIVIDE BY SANJIB BARUAH PAGE 8 selectChina BUSINESSASUSUAL entitiesface BY UNNY extravisascan Official:Tie-ups of Indian universities, institutionsare alsounder review SUSHANTSINGH The fire spread quickly, with smoke enveloping the powerhouse and the four storeysofthe plantthat lie underground, in Srisailam on Thursdaynight. PTI NEWDELHI,AUGUST21 AS SINO-INDIAN relations re- Bihar polls: In main tense following lackof Nine killed in Telangana powerhouse fire progress in talksonresolving the Thesteps, border situation in Ladakh, the EC guidelines, government is placing visasfor thesignal Five engineers among dead,survivors personsconnected to certain last hour of Red flags raised over dam’s poor Chinese think tanks, business EVER SINCE Beijing pre- saytheystayedbacktocontrolfire fora and advocacygroups under cipitated acrisis along voting day for the “requirement of prior the LACinLadakh, Delhi neers, including awoman engi- upkeep, fundscrunch in 2states screening/clearance”.