(Jcrc) 2014 Annual Report
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Republic of Uganda
REPUBLIC OF UGANDA VALUE FOR MONEY AUDIT REPORT ON SOLID WASTE MANAGEMENT IN KAMPALA MARCH 2010 1 TABLE OF CONTENTS REPUBLIC OF UGANDA .......................................................................................................... 1 VALUE FOR MONEY AUDIT REPORT ..................................................................................... 1 ON SOLID WASTE MANAGEMENT IN KAMPALA .................................................................... 1 LIST OF ABBREVIATIONS ...................................................................................................... 4 EXECUTIVE SUMMARY ........................................................................................................... 5 CHAPTER 1 ......................................................................................................................... 10 INTRODUCTION ................................................................................................................ 10 1.0 BACKGROUND .............................................................................................10 1.1 MOTIVATION ...............................................................................................12 1.2 MANDATE ....................................................................................................13 1.3 VISION ........................................................................................................13 1.4 MISSION ................................................................................................................. -

Vote:122 Kampala Capital City Authority V1: Vote Overview I
Kampala Capital City Authority Ministerial Policy Statement FY 2020/21 Vote:122 Kampala Capital City Authority V1: Vote Overview I. Vote Mission Statement To Deliver Quality Services to the City II. Strategic Objective 1. Improve Productivity of the city 2. Improve quality of social services 3. Enhance Attractiveness of the city 4. Enhance safety of communities 5. Improve Transport services 6. Improve Governance and Accountability 7. Optimize Resource Utilization 8. Increase Financial Resource Availability 9. Improve Communication 10. Promote Disaster Preparedness and Management 11. Improve Regulatory Framework 12. Improve Business Process Management 13. Improve Information Management 14. Increase KCCA Productivity 15. Enhance Human resource development 16. Enhance Strategic partnerships and collaboration 17. Improve Workplace Infrastructure Kampala Capital City Authority Ministerial Policy Statement FY 2020/21 Vote:122 Kampala Capital City Authority III. Major Achievements in 2019/20 SOLID WASTE MANAGEMENT -A total of 385 roads were cleaned across all divisions. Of these, 337 were swept daily whereas 48 roads periodically swept -A total of 112,801 tons of garbage was disposed of at the landfill from all the divisions by 189 (Max) collector trucks from a total of 21,858 trips of which 44% was delivered by KCCA while the rest (56%) was delivered by private companies -Fuelled and maintained 29 Garbage truck, made 5,683 trips to the Landfill at Kiteezi consuming a total of 119,623 litres of fuel. Community dialogue and sensitization -A total of 164 Community dialogues and sensitization meetings were conducted with 81 in Kawempe, 11 in Makindye, 26 in Central, 15 in Rubaga and 31 in Nakawa. -

Acknowledgement: the Authors Are Grateful for Financial Support from the Netherlands Ministry of Agriculture, Nature and Food Qu
PARTNERSHIPS FOR HEALTHY DIETS AND NUTRITION IN URBAN AFRICAN FOOD SYSTEMS – EVIDENCE AND STRATEGIES “THE KANYANYA FOOD CHALLENGE – FOOD SYSTEMS MAPPING” PROGRESS REPORT DELIVERABLE WP1: NOURICITY - KAMPALA Vincent Linderhof, Youri Dijkxhoorn (both Wageningen Economic Research), Joel Onyango (BoP innovation centre), Andrea Fongar (Bioversity International), and Martha Nalweyiso Date of the report 31-12-2019 Acknowledgement: The authors are grateful for financial support from the Netherlands Ministry of Agriculture, Nature and Food Quality (grant number BO-43-003.02-009 as part of LEAP-Agri program), and the flagship program Food Systems for Healthier Diets of the CGIAR program Agriculture for Nutrition and Health (A4NH). 1 | The Kanyanya food challenge Contents Glossary ............................................................................................................................ 3 List of figures ..................................................................................................................... 5 List of tables ...................................................................................................................... 6 1 Introduction ................................................................................................................. 7 2 Desk study ................................................................................................................... 8 1.1 2.1 Description of Kampala .................................................................................... 8 -

Public Health Environment Bulletin
V O L . 1 . | I S S U E 3 | J A N U A R Y 2 0 2 1 PUBLIC HEALTH & ENVIRONMENT BULLETIN D I R E C T O R A T E O F P U B L I C H E A L T H A N D E N V I R O N M E N T Dear Reader, Happy New year 2021! E D I T O R I A L T E A M Congratulations upon concluding the game changing year in public health (2020) We welcome you to issue 3, volume 1 of the KCCA-Public Daniel Ayen Okello Health and Environment Bulletin. The aim of this Bulletin is to document and communicate the works, achievements, Director Public Health & Environment and key challenges with regards to Kampala’s Public Health, Environment and other related events. The end goal is to Najib Lukoya Bateganya disseminate this information to the policy makers, health Deputy Director Public Health & professionals, the public, implementing partners and all Environment stakeholders. In this issue, we are excited to share with you a wide variety Sarah Zalwango of articles focusing on Kampala’s health and environment Manager Medical Services including: COVID-19 highlights and other PHEs, timely testing for Presumptive TB, participation of HIV clients in developing client-retention interventions, Maternal and New- Christopher Oundo born health care services, KCCA and Bloomberg’s Supervisor Medical Services Partnership on road safety and Gender Based Violence. While thanking you, we invite you to share with us your ideas Alex Ndyabakira and feedback. -
Owned Spaces and Shared Places
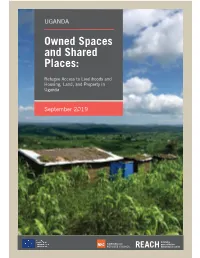
UGANDA Owned Spaces and Shared Places: Refugee Access to Livelihoods and Housing, Land, and Property in Uganda September 2019 Cover photo: Kyaka II refugee settlement. © IMPACT/2019 About REACH REACH Initiative facilitates the development of information tools and products that enhance the capacity of aid actors to make evidence-based decisions in emergency, recovery and development contexts. The methodologies used by REACH include primary data collection and in-depth analysis, and all activities are conducted through inter-agency aid coordination mechanisms. REACH is a joint initiative of IMPACT Initiatives, ACTED and the United Nations Institute for Training and Research - Operational Satellite Applications Programme (UNITAR-UNOSAT). For more information please visit our website: www.reach-initiative.org. You can contact us directly at: [email protected] and follow us on Twitter @REACH_info. About Norwegian Refugee Council The Norwegian Refugee Council is an independent humanitarian organisation working to protect the rights of displaced and vulnerable people during crises. NRC provides assistance to meet immediate humanitarian needs, prevent further displacement and contribute to durable solutions. NRC is Norway’s largest international humanitarian organisation and widely recognised as a leading field-based displacement agency within the international humanitarian community. NRC is a rights-based organisation and is committed to the humanitarian principles of humanity, neutrality, independence and impartiality. Refugee Access to Livelihoods and Housing, Land, and Property in Uganda – September 2019 AWKNOWLEDGEMENTS REACH Initiative and NRC would like to thank the government of Uganda’s Office of the Prime Minister (OPM) and the United Nations Commissioner for Refugees (UNHCR) for their assistance in designing and guiding this assessment. -
Usaid/Uganda Private Health Support Program (June 2013-June 2018)
USAID/UGANDA PRIVATE HEALTH SUPPORT PROGRAM (JUNE 2013-JUNE 2018) FINAL REPORT Contract No.: AID-617-C-13-00005 C Mothers and infants awaiting treatment at St Francis Health Care Services in Njeru (January 2018) September 2018 This report is made possible by the support of the American People through the United States Agency for International Development (USAID). The contents of this report are the sole responsibility of Cardno Emerging Markets USA, Ltd. and do not necessarily reflect the views of USAID or the United States Government. USAID/UGANDA PRIVATE HEALTH SUPPORT PROGRAM (JUNE 2013-JUNE 2018) FINAL REPORT Submitted by: Cardno Emerging Markets USA, Ltd. Submitted to: USAID/Uganda Contract No.: AID-617-C-13-00005 DISCLAIMER The author’s views expressed in this publication do not necessarily reflect the views of the United States Agency for International Development or the United States Government. USAID/Uganda Private Health Support Program Table of Contents ACRONYMS ............................................................................................................................................................. III EXECUTIVE SUMMARY ........................................................................................................................................... 1 CONTEXTUAL OVERVIEW ..................................................................................................................................... 4 PROGRAM OBJECTIVES ........................................................................................................................................... -

The Evolution of Town Planning Ideas, Plans and Their Implementation in Kampala City 1903-2004
School of Built Environment, CEDAT Makerere University, Kampala, Uganda and School of Architecture and the Built Environment Royal Institute of Technology, Stockholm, Sweden The Evolution of Town Planning Ideas, Plans and their Implementation in Kampala City 1903-2004 Fredrick Omolo-Okalebo Doctoral Thesis in Infrastructure, Planning and Implementation Stockholm 2011 i ABSTRACT Title: Evolution of Town Planning Ideas, Plans and their Implementation in Kampala City 1903-2004 Through a descriptive and exploratory approach, and by review and deduction of archival and documentary resources, supplemented by empirical evidence from case studies, this thesis traces, analyses and describes the historic trajectory of planning events in Kampala City, Uganda, since the inception of modern town planning in 1903, and runs through the various planning episodes of 1912, 1919, 1930, 1951, 1972 and 1994. The planning ideas at interplay in each planning period and their expression in planning schemes vis-à-vis spatial outcomes form the major focus. The study results show the existence of two distinct landscapes; Mengo for the Native Baganda peoples and Kampala for the Europeans, a dualism that existed for much of the period before 1968. Modern town planning was particularly applied to the colonial city while the native city grew with little attempts to planning. Four main ideas are identified as having informed planning and transformed Kampala – first, the utopian ideals of the century; secondly, “the mosquito theory” and the general health concern and fear of catching „native‟ diseases – malaria and plague; thirdly, racial segregation and fourth, an influx of migrant labour into Kampala City, and attempts to meet an expanding urban need in the immediate post war years and after independence in 1962 saw the transfer and/or the transposition of the modernist and in particular, of the new towns planning ideas – which were particularly expressed in the plans of 1963-1968 by the United Nations Planning Mission. -

Health Sector Annual Budget Monitoring Report FY2019/20
Health SECtor ANNUAL BUDGET MONITORING REPORT FINANCIAL YEAR 2019/20 NOVEMBER 2020 Ministry of Finance, Planning and Economic Development P.O. Box 8147, Kampala www.finance.go.ug Health Sector : Annual Budget Monitoring Report - FY 2019/20 A HEALTH SECtor ANNUAL BUDGET MONITORING REPORT FINANCIAL YEAR 2019/20 NOVEMBER 2020 Ministry of Finance, Planning and Economic Development TABLE OF CONTENTS ABBREVIATIONS AND ACRONYMS ............................................................................................... iii FOREWORD ...................................................................................................................................... iv EXECUTIVE SUMMARY ..................................................................................................................... v CHAPTER 1: INTRODUCTION ........................................................................................................ 1 1.1 Background .................................................................................................................................. 1 CHAPTER 2: METHODOLOGY ....................................................................................................... 2 2.1 Scope ....................................................................................................................................... 2 2.2 Methodology ................................................................................................................................ 3 2.2.1 Sampling ..................................................................................................................................... -

Kampala, Uganda, 2016 Produced By: Lars Schoebitz, Eawag/Sandec Charles B
SFD Promotion Initiative Kampala Uganda Final Report This SFD Report was prepared through desk-based research by Sandec (the Department of Sanitation, Water and Solid Waste for Development) at Eawag (the Swiss Federal Institute of Aquatic Science and Technology) as part of the SFD Promotion Initiative. Collaborating partners Date of production: 06.06.2016 Last update: 11.07.2016 Kampala Executive Summary Produced by: Eawag/Sandec Uganda SFD Report Kampala, Uganda, 2016 Produced by: Lars Schoebitz, Eawag/Sandec Charles B. Niwagaba, Makerere University Linda Strande, Eawag/Sandec ©Copyright All SFD Promotion Initiative materials are freely available following the open-source concept for capacity development and non-profit use, so long as proper acknowledgement of the source is made when used. Users should always give credit in citations to the original author, source and copyright holder. This Executive Summary and SFD Report are available from: www.sfd.susana.org Last Update: 06/06/2016 I Kampala Executive Summary Produced by: Eawag/Sandec Uganda 1. The Diagram Note: Percentages do not add up to 100 due to rounding 2. Diagram information dry seasons between December and March, and June and July (KSMP, 2004). The Shit Flow Diagram (SFD) was developed through desk-based research by Sandec 64% of the city is classified as residential area. (Sanitation, Water and Solid Waste for Wakiso and Mukono Districts surround Development) of Eawag (the Swiss Federal Kampala and have a population of 1,997,418 Institute of Aquatic Science and Technology) (Wakiso) and 596,804 (Mukono) (UBOS, and CEDAT (College of Engineering, Design 2016). It is estimated that the population Art and Technology) at Makerere University. -

Water Provision in Urban Centres, Water Sources
WATER PROVISION IN URBAN CENTRES, WATER SOURCES ANDSUPPLY INSTITUTIONS: A CASE STUDY OF LUBAGA DIVISION KAMPALA WASSWA-NSUBUGA FRANCIS B.A. ED. (HON) M.U A DISSERTATION SUBMITTED IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE MASTERS DEGREE OF ARTS IN LAND USE AND REGIONAL DEVELOPMENT (L.U.R.D) IN THE DEPARTMENT OF GEOGRAPHY, MAKERERE UNIVERSITY KAMPALA. FEBRUARY 2002 ii DECLARATION I WASSWA-NSUBUGA FRANCIS declare that this piece of work is mine and has never been presented in any University or Institution of higher learning for an academic award. Signed: ……………………………………………………. Date: ……………………………………………………. Signed: …………………………………………………… Dr. Hannington Sengendo Supervisor Date: …………………………………………………… iii DEDICATION This dissertation is dedicated to my late father Salongo Isaaya Nkugwa Bakunga, my mother Nalongo Imelda Nalukenge, my maternal Auntie’s and the entire family, for their parental, financial and spiritual support which have enabled me to attain this level of education. iv ACKNOWLEDGEMENT Many people have assisted me in various ways throughout the shaping of this dissertation and it is not possible to thank all of them individually. But I am particularly grateful to my supervisor Dr. H. Sengendo, Prof. Gunilla Andrae, the scholars and contributors on the project “people, provisioning and place”, who constantly reviewed and guided this work. I wish also to thank my mother Imelda Nalongo Nalukenge, Benjamin Kato Nkugwa, Masoudi Nsubuga, Nsereko Robert, Edith Namutebi for the encouragement and assistance rendered to me. Daisy Kirumira, I am grateful that you typed this work. I do appreciate the permission and tolerance given to me at my place of work to enable me finish this work. -

Vote: 122 Kampala Capital City Authority Structure of Submission
Vote Performance Report and Workplan Financial Year 2015/16 Vote: 122 Kampala Capital City Authority Structure of Submission QUARTER 3 Performance Report Summary of Vote Performance Cumulative Progress Report for Projects and Programme Quarterly Progress Report for Projects and Programmes QUARTER 4: Workplans for Projects and Programmes Submission Checklist Page 1 Vote Performance Report and Workplan Financial Year 2015/16 Vote: 122 Kampala Capital City Authority QUARTER 3: Highlights of Vote Performance V1: Summary of Issues in Budget Execution This section provides an overview of Vote expenditure (i) Snapshot of Vote Releases and Expenditures Table V1.1 below summarises cumulative releases and expenditures by the end of the quarter: Table V1.1: Overview of Vote Expenditures (UShs Billion) Approved Cashlimits Released Spent by % Budget % Budget % Releases (i) Excluding Arrears, Taxes Budget by End by End End Mar Released Spent Spent Wage 24.820 40.561 18.615 18.560 75.0% 74.8% 99.7% Recurrent Non Wage 6.072 20.546 4.079 3.952 67.2% 65.1% 96.9% GoU 2.145 34.312 0.741 0.596 34.6% 27.8% 80.4% Development Donor* 0.000 N/A 0.000 0.000 N/A N/A N/A GoU Total 33.037 95.419 23.435 23.109 70.9% 69.9% 98.6% Total GoU+Donor (MTEF) 33.037 N/A 23.435 23.109 70.9% 69.9% 98.6% Arrears 0.000 N/A 0.000 0.000 N/A N/A N/A (ii) Arrears and Taxes Taxes** 0.000 N/A 0.000 0.000 N/A N/A N/A Total Budget 33.037 95.419 23.435 23.109 70.9% 69.9% 98.6% (iii) Non Tax Revenue 3.118 N/A 1.960 1.781 62.9% 57.1% 90.9% Grand Total 36.155 95.419 25.395 24.890 70.2% 68.8% -
Statistical Abstract for Kampala City 2019
Kampala City Statistical Abstract, 2019 STATISTICAL ABSTRACT FOR KAMPALA CITY 2019 Report prepared with support from Uganda Bureau of Statistics Kampala City Statistical Abstract, 2019 TABLE OF CONTENTS ACRONYMS …………………………………………………………………….…………………………………………. vii ABOUT THIS STATISTICAL ABSTRACT ……………………………………………………………………...………. viii ACKNOWLEDGMENT ……………………………………………………………………………………………………… ix DEFINITIONS USED AS ADAPTED FROM THE NATIONAL POPULATION & HOUSING CENSUS REPORT (2014) 1 CHAPTER ONE: KAMPALA BACKGROUND INFORMATION …………………….…………………………. 2 CHAPTER TWO: CITY ADMINISTRATION ………………………………………….……………………………. 10 CHAPTER THREE: DEMOGRAPHIC AND SOCIO-ECONOMIC CHARACTERISTICS ………….……………. 23 CHAPTER FOUR: CITY ECOMOMY, BUSINESS, EMPLOYMENT AND LABOUR SERVICES ……………. 30 CHAPTER FIVE: TRANSPORT AND GETTING AROUND KAMPALA ……………….………………………. 51 CHAPTER SIX: HEALTH SERVICES …………………………………….……………………………………. 61 CHAPTER SEVEN: WATER, SANITATION, ENVIRONMENT ……………………………………………………. 73 CHAPTER EIGHT: EDUCATION SERVICES …………………………………….………………………………. 81 CHAPTER NINE: SOCIAL SERVICES ……………………………………….……………………………………. 87 CHAPTER TEN: CRIME, ACCIDENTS AND FIRE EMERGECIES ………………….……………………….. 93 CHAPTER ELEVEN: ASSORTED KCCA PERFORMANCE STATISTICS 2011 – 2019 …….…………………. 97 GENERAL INFORMATION …………………………………………………………………………………………………. 106 ii Kampala City Statistical Abstract, 2019 LIST OF TABLES Table 1: Distance to Kampala from Major Cities ......................................................................................................................................................................................................