The Hemlock Society: What We Are, What We Aren't, and Why
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
How We Die in North Carolina
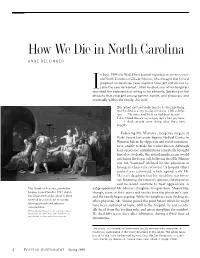
How We Die in North Carolina ANNE DELLINGER n June 1998 the Wall Street Journal reported on seventy-year- old North Carolinian Claude Marion, who thought that he had prepared for death ten years ahead of time, but still did not re- Iceive the care he wanted.1 After he died, one of his daughters described the experience of acting as his advocate. Speaking of the divisions that emerged among patient, family, and physician, and eventually within the family, she said, [My father] just tried really hard to do the right thing. And he died in a very undignified way. I felt so help- less. My sister and I felt we had been to war. I don’t think there’s a good guy and a bad guy here. I think people were doing what they were taught.2 Following Mr. Marion’s emergency surgery at Wake Forest University Baptist Medical Center in Winston-Salem, he slipped in and out of conscious- ness, unable to make his wishes known. Although four successive complications repeatedly brought him close to death, the attending physician would not honor the living will, believing that Mr. Marion was not “terminal” (defined by the physician as having no chance for recovery).3 A hospital ethics council was convened, which agreed with Mr. Marion’s daughters that his condition was termi- nal. Rejecting the council’s opinion, the physician said he would continue to treat aggressively. A The Death of Socrates, painted by judge appointed Mr. Marion’s daughters his guardians. Meanwhile, Jacques Louis David in 1787, depicts though, some of their aunts and uncles took the physician’s side, the Greek philosopher about to drink and the family began arguing. -
FENA Conversation with Fran
FINAL EXIT NETWORK VOL 18 • NO 1 WINTER, JAN/FEB 2019 CONTENTS TTHEHE TIME TO IMPROVE OREGON-STYLE LAWS? .........3 GOODGOOD DEMENTIA ADVANCE DEATHDEATH DIRECTIVES ...........................5 FISCAL YEAR REPORT ............9 SOCIETYSOCIETY AMERICANS ACCEPT FEN EUTHANASIA ..................... 11 A Conversation With Fran By Michael James, FEN Life Member enior Guide Fran Schindler’s voice was raspy after five days of protesting in Washington, DC, but this remarkable 79- Q: year-old’sS enthusiasm for FEN and life in general was loud and clear. “The privilege of someone being What’s going to willing to have me with them when they die, when I happen to you? only just sit with them, is the most meaningful thing I have ever done.” In the late 1980s, Fran faced a series of daunt- ing issues: a brain tumor, divorce, and mysterious A. symptoms which mimicked ALS. She acknowledg- es she became obsessed with finding ways to kill I will get dead. herself during those dark days. Eventually she heard Faye Girsh lecture about FEN. She quickly signed up for training and got her FEN membership card in November 2006. Twelve years later she estimates FRAN continued on page 2 Renew your membership online: www.finalexitnetwork.org FRAN continued from page 1 she’s been present for over 70 individuals who have taken their lives using FEN protocol. “At the FEN training class I discovered a major benefit of being a “Start doing FEN member. I looked at the trainers and my fellow classmates—people who didn’t know me—and real- what you want ized that if I needed them they would be there for me. -

Physician-Assisted Suicide
Recent Developments in Physician-Assisted Suicide October 2001 Copyright © 2001 Valerie J. Vollmar, all rights reserved. LITIGATION 1. Sampson v. Alaska, No. 3AN-98-11288CI (Alaska Super. Ct.), aff'd, 31 P.3d 88 (Alaska 2001). On 12/15/98, Kevin Sampson (a 43-year-old HIV-positive man) and "Jane Doe" (a female physician in her 60's with cancer) filed suit in Alaska Superior Court in Anchorage challenging Alaska's ban on physician-assisted suicide based on state constitutional claims of privacy, liberty, and equal protection. On 9/9/99, Judge Eric T. Sanders issued a written opinion rejecting the plaintiffs' claims and granting summary judgment to the defendant. On 11/14/00, the Alaska Supreme Court heard arguments on the appeal. On 9/21/01, the supreme court issued an opinion affirming the lower court's decision. 2. Cooley v. Granholm, No. 99-CV-75484 (E.D. Mich.), appeal pending, No. 01-1067 (6th Cir.). On 11/12/99, Professor Robert Sedler filed a federal lawsuit against Attorney General Jennifer Granholm and the Michigan Board of Medicine on behalf of two Michigan physicians, Roy Cooley and M.W. El-Nachef. The plaintiffs claimed that Michigan's ban on assisted suicide violates the Fourteenth Amendment right "to be relieved from unbearable pain and suffering." On 12/20/00, Judge Nancy G. Edmunds granted the defendants' motion for summary judgment and dismissed the complaint. On 1/12/01, plaintiffs appealed to the Sixth Circuit Court of Appeals. The final brief on appeal was filed on 6/4/01. Both sides have requested oral argument. -

The Right to Assisted Suicide and Euthanasia
THE RIGHT TO ASSISTED SUICIDE AND EUTHANASIA NEIL M. GORSUCH* I. INTRODUCTION ........................................................ 600 I. THE COURTS ............................................................. 606 A. The Washington Due Process Litigation............ 606 1. The Trial Court ...................... 606 2. The Ninth Circuit Panel Decision ............. 608 3. The En Banc Court ...................................... 609 B. The New York Equal ProtectionLitigation ........ 611 1. The Trial Court ........................................... 611 2. The Second Circuit ..................................... 612 C. The Supreme Court............................................. 613 1. The Majority Opinion ................................. 614 2. The Concurrences ....................................... 616 D. The Consequences ofGlucksberg and Quill .... 619 III. ARGUMENTS FROM HISTORY ................................... 620 A. Which History?................................................... 620 B. The Ancients ....................................................... 623 C. Early Christian Thinkers .................................... 627 D. English Common Law ......................................... 630 E. ColonialAmerican Experience........................... 631 F. The Modern Consensus: Suicide ........................ 633 G. The Modern Consensus: Assisting Suicide and Euthanasia.......................................................... 636 IV. ARGUMENTS FROM FAIRNESS .................................. 641 A . Causation........................................................... -

Toxicological Findings in Helium Deaths 2005-2010 Dawn Reed, LGC Forensics, F5 Culham Science Centre, Abingdon, Oxfordshire OX14 3ED
2834 - Tox helium deaths tech. poster:1281 - BMSS Poster for Della Shanahan v5.qxd 01/12/2010 09:31 Page 1 Toxicological findings in helium deaths 2005-2010 Dawn Reed, LGC Forensics, F5 Culham Science Centre, Abingdon, Oxfordshire OX14 3ED Final exit: The practicalities of self-deliverance and assisted suicide for the dying • The drugs available to the individuals are shown in the table below. Derek Humphry assisted his wife in taking a fatal drug overdose after she suffered declining health due to terminal cancer. He wrote the book Final Exit 1 in 1991 as a guide to others in similar situations. Final Exit sparked a debate surrounding Available drug No. of cases self-deliverance, assisted suicide and euthanasia which remains a contentious topic both morally and legally. Antidepressants Chlorpromazine 1 The 3rd edition of Final Exit, which was updated in April 2010 2, contains a comprehensive set of instructions on how to take a Escitalopram 1 life using helium, stating that death should occur in approximately five minutes. The chapter begins by informing the reader to Fluoxetine 1 purchase two cylinders of helium from a toy shop, and that using cash is advisable to avoid later investigations. The process is Mirtazapine 3 Paroxetine 1 described with the aid of diagrams and it is recommended that the 'patient' practices before the final attempt – there is a video Sertraline 1 available to purchase if required. Anti-Psychotics Interestingly, the author discusses the fact that so long as there are no bag marks on the neck, it should be possible to clear Lithium 1 away the bag and cylinder, wait an hour or two and then call for a doctor as if the natural disease state has finally caused the Olanzapine 1 Risperidone 2 individual's inevitable death. -

Debate on Euthanasia (Pros and Cons)
UNIVERSIDADE CATÓLICA PORTUGUESA FACULDADE DE TEOLOGIA MESTRADO INTEGRADO EM TEOLOGIA (1.º grau canónico) JOSEPH PAKHU DEBATE ON EUTHANASIA (PROS AND CONS) Dissertação Final sob orientação de: PROF. FAUSTO GOMEZ, O.P., S.Th.D Lisboa 2015 APPROVAL SHEET DEBATE ON EUTHANASIA (PROS AND CONS) JOSEPH PAKHU, OP Chairman:____________________________________________________________________ Examiner:____________________________________________________________________ Supervisor:____________________________________________________________________ ACKNOWLEDGMENT With the writing of this thesis, my time as a USJ student is about to end. At the end of this journey, I have to say “thank you.” I’d like to say “thank you” above all to God, because through his grace and blessing I have managed to accomplish this research paper. Moreover, I would like to express my sincere gratitude to the many wonderful people accompanied me and helped me in one way or another throughout these few years as a USJ student. In particular, I wish to thank the USJ Faculty of Religious Studies, its staff, and all the professors who shared their knowledge with us students, including Fr. Fausto Gomez O.P who has supervised me throughout this journey of writing my thesis. I am sincerely thankful to him for his time and generosity. In the second place, I like to thank also all the Dominican priests here in Macau who have walked with me and taken care of my needs as a Dominican Student brother. Also I give many thank, to all my Dominican brothers and sisters as well as to my other classmates. Indeed, it has been a good learning experience with all during these several years. I wish them all the best in your studies and life. -
The Death of and the -1 Truth About, Euthanasia
If someone you care about bought FinaZElxit, you must buy them D~lyComl,assiOn. Derek : The There. You got what you wanted. Ever since I was diagnosed as having cancer, you have done Death of everything conceivable to pre- cipitate my death. I was not alone in recognizing what you were doing. What you Hulll~hrvA did--desertion and abandonment Ann and subsequent harrassment of a dying woman--is so unspeakble there are no words to describe -1 the horror of it. and the Yet you know. And others know too. You will have to live with this untiol you die. Truth About, 1 May you never, ever forget. Euthanasia This is the actual suicide letter left by Ann Humphry. The hand- written note was added by Ann to a copy sent to Rita Marker, author of this book. The letter itself was addressed to Ann's husband, Derek Humphry, co-founder of the Hemlock Society and author of the number-one best-seller Rnal Exit. - '1 MAR 1 t RITA MARKER ISBN 0-688-12223-3 8 ,'\- IF " ISBN 0-688-12221-3 FPT $18.00 wtinuedfiomfiotatjap) ,, Tack Kevorkian. who has written article advocating medical experiments on death row prisoners -while they are still alive. An( she explains the ramifications of euthanasia course is not the same as giving in a country without adequate health insur- doctors the right to kill ance, like America, where people who really their patients on demand. want to live might choose death rather than bankrupt their families. Deadly Compassion is essential reading for anyone who has misgivings about giving DEADLY COMPASSION doctors the right to kill. -

Freedom to Flourish: a Catholic Analysis of Doctor–Prescribed Suicide and Euthanasia
V VERITAS Freedom to Flourish: A Catholic Analysis of Doctor–Prescribed Suicide and Euthanasia Jason B. Negri, JD and Father Christopher M. Saliga, O.P., RN The Veritas Series is dedicated to Blessed Michael McGivney (1852-1890), priest of Jesus Christ and founder of the Knights of Columbus. The Knights of Columbus presents The Veritas Series “Proclaiming the Faith in the Third Millennium” Freedom to Flourish: A Catholic Analysis of Doctor-Prescribed Suicide and Euthanasia by JASON B. NEGRI, JD & FR. CHRISTOPHER M. SALIGA, O.P., RN General Editor Fr. Juan-Diego Brunetta, O.P. Catholic Information Service Knights of Columbus Supreme Council Printed With Ecclesiastical Permission. Most Reverend Earl Boyea November 3, 2010 Diocese of Lansing Copyright ©2011-2021 by Knights of Columbus Supreme Council. All rights reserved. Cover: © 2011-2021 by Knights of Columbus Supreme Council. All rights reserved. No part of this book may be reproduced or transmitted in any form or by any means, electronic or mechanical, including photocopying, recording, or by information storage and retrieval system, without permission in writing from the publisher. Write: Catholic Information Service Knights of Columbus Supreme Council PO Box 1971 New Haven CT 06521-1971 www.kofc.org/cis [email protected] 203-752-4267 800-735-4605 fax Printed in the United States of America CONTENTS INTRODUCTION . 5 KILLING TO END SUFFERING?. 6 RATIONALE FOR KILLING . 7 SUFFERING. 9 LOSS OF AUTONOMY . 11 AUTONOMY AND THE CASE OF JO ROMAN . 13 FREEDOM TO FLOURISH . 15 FREEDOM TO FLOURISH: THE CASE OF CHRISTI CHRONOWSKI . 17 CHRISTI’S DIAGNOSIS: A VIRTUAL GUARANTEE OF SUFFERING AND DEATH. -

Physician-Assisted Suicide: Why Physicians Should Oppose It
Physician-Assisted Suicide: Why Physicians Should Oppose It Joseph E. Marine, MD, MBA Division of Cardiology Johns Hopkins University School of Medicine February 2, 2018 Disclosures • No relevant financial disclosures • I am a member of the American College of Physicians, the American Medical Association, and the Baltimore City Medical Society • All of these organizations oppose legalization of physician-assisted suicide and all other forms of euthanasia • There are no drugs or devices that have been approved by the US FDA for physician-assisted suicide or euthanasia Some Definitions • Physician-Assisted Suicide: A form of euthanasia (“good death) where a physician provides the means (such as a lethal drug prescription) for a patient to end his/her own life • Synonyms/ Euphemisms: • Physician/doctor-assisted death • Death with Dignity • End-of-Life Option • (Medical) Aid-in-Dying • includes euthanasia by lethal injection in Canada • Usual drugs used: 90-100 x 100 mg secobarbital tabs dissolved in liquid and swallowed quickly • Antiemetic premed usually given to prevent vomiting PAS/Euthanasia: Background • Mid-1800s – increasing medical use of morphine and chloroform anesthesia leads to proposals to use to hasten death for patients with advanced illnesses • 1906: Euthanasia law proposed in Ohio state legislature, voted down 79-23 • 1920s-1930s: Public support for euthanasia increases in USA, though not legally adopted • 1939-1945: WWII, Nuremberg trials Euthanasia in post-war era • 1945-1980: Little activity • 1980: Derek Humphry, a British journalist, founds Hemlock Society to promote euthanasia and assisted suicide for patients with advanced illness • 1992: Publication of Final Exit • 2003-4: Hemlock Society becomes Compassion and Choices Dr. -

FDA Regulation and Patient Assisted Suicides
FDA Regulation and Patient Assisted Suicides The Harvard community has made this article openly available. Please share how this access benefits you. Your story matters Citation FDA Regulation and Patient Assisted Suicides (1995 Third Year Paper) Citable link http://nrs.harvard.edu/urn-3:HUL.InstRepos:8965589 Terms of Use This article was downloaded from Harvard University’s DASH repository, and is made available under the terms and conditions applicable to Other Posted Material, as set forth at http:// nrs.harvard.edu/urn-3:HUL.InstRepos:dash.current.terms-of- use#LAA FDA Regulation and Patient Assisted Suicides David S. Weiss The 20th century has witnessed a steady, marked increase in the average life expectancy of Americans. Advances in nutrition, an increased em- phasis on preventative health care, and developments in the treatment and miti- gation of cancer and other fatal illnesses are among the many factors which have contributed most recently to the ability of Americans to live longer, healthier lives. Even with these advances, however, there are an increasing number of Americans who believe that the marginal benefit of surviving a few extra months is not worth the cost of suffering the pain, physical and/or mental deterioration, or increased dependency they would experience during that period due to a terminal illness or a debilitating condition. For these people, the right to opt to die painlessly, simply, and with dignity at the time and place of their choosing is paramount, and in recent years they have taken steps to secure that right. Their convictions have given rise to the Hemlock Society,1 the passage of an Oregon referendum authorizing physician-assisted suicide,2 and the work of Dr. -

2020-Winter.Pdf
FINAL EXIT NETWORK VOL 19 • NO 1 WINTER 2020 IN THIS ISSUE • A devoted husband’s murder-suicide farewell Page 2 • Mary Ewert: dementia and the growing RTD crisis 4 • How ‘Nora’ easily bequeathed a ‘thank you’ gift 5 • Volunteer Hall still leaves a distinguished mark 6 • Veterinarian has poetic take on peaceful deaths 12 • Grateful clients give voice to the essence of FEN 14 T R A I BULETN TO DELIVERANCE ‘My father shot my mother and then himself because her Alzheimer’s was too advanced for anyone to think she was competent to make a decision.’ By Jay Niver, FEN Editor criminal case,” Janet said. “They don’t cover suicides.” murder-suicide usually makes news. The details were unknown to all but the But when that tragedy involves an close friends and family to whom Bob wrote a elderly, devoted couple – and one or A letter, explaining their choice two days before both of them have debilitating dementia or a he pulled the trigger: first for his wife of more terminal disease – it grabs few headlines. than 60 years; then for himself. Authorities, family, friends, and courts The Shavers, too, had a long and storybook recognize that the victims planned and chose marriage. Alma was 80 and he was 79. It ended their exit because they didn’t have (or know) for them on a warm, Sunday afternoon last another way. June as they lay together on their canopy bed. Richard and Alma Shaver decided upon Some would say it ended such a death. But theirs made news across the for them much country after the Sunday New York Times ran a major feature last Dec. -

Don't Tell: the Secret Practice of Physician-Assisted Suicide, 44 Hastings L.J
Hastings Law Journal Volume 44 | Issue 6 Article 3 1-1993 Don't Ask--Don't Tell: The ecrS et Practice of Physician-Assisted Suicide Julia Pugliese Follow this and additional works at: https://repository.uchastings.edu/hastings_law_journal Part of the Law Commons Recommended Citation Julia Pugliese, Don't Ask--Don't Tell: The Secret Practice of Physician-Assisted Suicide, 44 Hastings L.J. 1291 (1993). Available at: https://repository.uchastings.edu/hastings_law_journal/vol44/iss6/3 This Note is brought to you for free and open access by the Law Journals at UC Hastings Scholarship Repository. It has been accepted for inclusion in Hastings Law Journal by an authorized editor of UC Hastings Scholarship Repository. For more information, please contact [email protected]. Note Don't Ask-Don't Tell: The Secret Practice of Physician-Assisted Suicide by JULIA PUGLIESE* It hath often been said that it is not death but dying that is terrible.1 Introduction Initially, Dr. Ethan Green2 was opposed to assisted suicide.3 How- ever, he was forced to reevaluate his position when a patient with AIDS, Michael Ellis, asked him for help in ending his life. Dr. Green thought he would be able to dissuade Michael by suggesting an aggressive pain treatment plan. After consultation the patient refused to accept the treatment option. Michael wanted to die. Dr. Green agonized over whether he should help Michael. He ini- tially told Michael that he needed to know more about him and his views and about the situation before he could make a decision to help. Dr.