Official 30-Day Inpatient Hospital Rate Review – Posting Date
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Exhibit #2 Base Rates and Cost-To-Charge Ratios Source: Medicare FY 2019 IPPS Impact File - Correction Notice (September 2018) Effective 1/1/2020
Exhibit #2 Base Rates and Cost-to-Charge Ratios Source: Medicare FY 2019 IPPS Impact File - Correction Notice (September 2018) Effective 1/1/2020 Provider Total Individual Hospital Name Number CCR Base Rate 060001 North Colorado Medical Center 0.268 $6,930.02 060003 Longmont United Hospital 0.323 $6,416.24 060004 Platte Valley Medical Center 0.420 $6,296.29 060006 Montrose Memorial Hospital 0.404 $6,250.18 060008 San Luis Valley Health 0.386 $6,250.18 060009 Lutheran Medical Center 0.235 $6,370.99 060010 Poudre Valley Hospital 0.302 $6,499.23 060011 Denver Health Medical Center 0.324 $8,185.33 060012 Centura Health-St Mary Corwin Medical Center 0.229 $6,818.43 060013 Mercy Regional Medical Center 0.287 $8,029.28 060014 Presbyterian St Lukes Medical Center 0.154 $6,905.48 060015 Centura Health-St Anthony Hospital 0.205 $6,365.32 060020 Parkview Medical Center Inc 0.164 $6,901.98 060022 University Colo Health Memorial Hospital Central 0.221 $6,426.00 060023 St Mary’s Medical Center 0.308 $6,994.17 060024 University Of Colorado Hospital Authority 0.169 $7,902.58 060027 Foothills Hospital 0.218 $6,312.83 060028 Saint Joseph Hospital 0.196 $7,001.47 060030 Mckee Medical Center 0.366 $6,362.47 060031 Centura Health-Penrose St Francis Health Services 0.212 $6,387.05 060032 Rose Medical Center 0.136 $6,735.37 060034 Swedish Medical Center 0.120 $6,539.19 060044 Colorado Plains Medical Center 0.264 $6,621.20 060049 Uchealth Yampa Valley Medical Center 0.539 $9,490.44 060054 Community Hospital 0.322 $6,242.53 060064 Centura Health-Porter Adventist -

Town of Vail
TOWN OF VAIL TURNING YOUR FEEDBACK INTO ACTION Focusing on Housing for Local Families Making Progress with Parking & Transportation Taking a Leadership Role in Sustainability Financial & Department Updates THE DAVIS FAMILY New homeowners at Chamonix Vail in West Vail Building on In the pages that follow, learn what the Vail Town Council, Board your Feedback and Commission members, town staff and agency partners have been doing to involve the community in: 2017 was the year for listening, focus • Providing additional housing opportunities for local residents and action. With information gathered • Making it easier to get around town from the biennial community survey • Becoming a leader in our environmental sustainability practices coupled with ongoing outreach, including online forums and involvement from • Enhancing neighborhood amenities all corners of the community, considerable • Advancing Vail’s appeal as the premier international mountain progress was made in the focus areas of ECONOMY, COMMUNITY and EXPERIENCE. resort community Together, these initiatives are keeping Vail in a leadership position as the Premier Lastly, we’re pleased to celebrate the talents and contributions of International Mountain Resort Community. the people who have come together to make Vail a special place. 2017 MILESTONES JANUARY FEBRUARY MARCH APRIL MAY JUNE Jan 16 Feb 21 March 7 April 1 May 4 June 3 Community members invited Re-dedication of newly-renovated Life-Saving Recognition Awards Online citizen portal launched Year-round safe disposal Launch of -
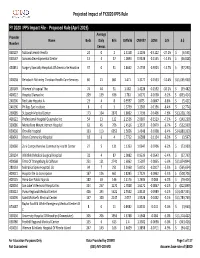
FY 2020 Proposed Rule Impact File.Xlsx
Projected Impact of FY2020 IPPS Rule FY 2020 IPPS Impact File ‐ Proposed Rule (April 2019) Average Provider Name Beds Daily Bills CMIV36 CMIV37 ∆CMI ∆ % ∆ $ Number Census 060107 National Jewish Health 24 0 2 1.5158 1.1036 ‐0.4122 ‐27.2%$ (6,595) 050547 Sonoma Developmental Center 13 4 37 1.0893 0.9338 ‐0.1555 ‐14.3% $ (46,028) 450831 Surgery Specialty Hospitals Of America Se Houston 37 0 31 2.8662 2.4739 ‐0.3923 ‐13.7%$ (97,290) 320038 Rehoboth Mckinley Christian Health Care Services 60 21 861 1.471 1.3177 ‐0.1533 ‐10.4%$ (1,055,930) 150149 Women's Hospital The 74 44 31 1.582 1.4228 ‐0.1592 ‐10.1%$ (39,482) 400022 Hospital Damas Inc 209 139 636 1.781 1.6172 ‐0.1638 ‐9.2%$ (833,414) 240206 Red Lake Hospital A 23 4 8 0.9597 0.875 ‐0.0847 ‐8.8%$ (5,421) 240196 Phillips Eye Institute 8 0 3 1.3739 1.2583 ‐0.1156 ‐8.4%$ (2,774) 260085 St Joseph Medical Center 173 104 2870 1.8602 1.7196 ‐0.1406 ‐7.6%$ (3,228,176) 400122 Professional Hospital Guaynabo Inc 54 13 122 2.1536 2.0007 ‐0.1529 ‐7.1%$ (149,230) 330086 Montefiore Mount Vernon Hospital 63 45 706 1.4516 1.3537 ‐0.0979 ‐6.7%$ (552,939) 050030 Oroville Hospital 133 113 6052 1.5656 1.4648 ‐0.1008 ‐6.4%$ (4,880,333) 460043 Orem Community Hospital 18 6 4 1.7712 1.6588 ‐0.1124 ‐6.3%$ (3,597) 320060 Zuni Comprehensive Community Health Center 27 5 131 1.1353 1.0647 ‐0.0706 ‐6.2%$ (73,989) 250134 Whitfield Medical Surgical Hospital 32 4 87 1.0082 0.9539 ‐0.0543 ‐5.4%$ (37,793) 420068 Trmc Of Orangeburg & Calhoun 251 121 2741 1.6062 1.5207 ‐0.0855 ‐5.3%$ (1,874,844) 280133 Nebraska Spine Hospital, -

Posting Date: June 1, 2021 This Posting
Posting Date: June 1, 2021 This posting serves as notification of SFY 2021-22 Outpatient Hospital EAPG Base Rates for all Hospitals participating in Health First Colorado. Consistent with the SFY20-21 EAPG Base Rates, individual letters will not be issued to each hospital. This method of communicating hospital rates has been approved by Hospitals participating in our Hospital Engagement Meetings that occur every other month. Information about past and upcoming Hospital Engagement Meetings is available at https://www.colorado.gov/pacific/hcpf/hospital-engagement-meetings. Hospital Base Rate Increase SFY 2021-22: The outpatient hospital EAPG base rates reflect the 2.5% provider rate increase effective July 1, 2021, as mentioned in SB 21-205. The rates in this letter show a 2.5% increase of the EAPG base rates that were effective July 1, 2020. Request for Informal Reconsideration or Appeal: Reimbursement rates for outpatient hospital services were calculated according to the regulations of the Health First Colorado Program. If you disagree with these figures, you may file a written request for informal reconsideration with the Department within thirty (30) days from the “posting date” listed in this communication. The request shall state the specific component of the rate the Provider wants reconsidered and the Provider’s position. Requests that do not comply with the requirements of this section shall be considered incomplete and shall be denied. If you desire an informal reconsideration for your hospital’s July 1, 2021 Outpatient Base Rate, please send your written request including your position as to each identified concern regarding the rate determination to: Andrew Abalos Fee-for-Service Rates Section Department of Health Care Policy and Financing 1570 Grant Street Denver, CO 80203 You may file an appeal of the decision on the informal reconsiderations with the office of administrative courts, as set forth at 10 C.C.R. -

Data Available in the Network
Data Available in the CORHIO Network MSH:4 values are the identification codes associated with data senders on CORHIO Notifications reports. Admission/ Laboratory Pathology Radiology Radiology Transcription Patient Care Summary HIE provider Discharge/ Reports Images Notes Centered Data Documents Available in Transfer Home Alerts PatientCare 360 1st Care Medical Clinic √ HEALTH CURRENT (MSH:4 VALUE: FCMC_HEALTHCURRENT) A New Leaf √ HEALTH CURRENT (MSH:4 VALUE: ANEWLF_HEALTHCURRENT) A. T. Still University √ HEALTH CURRENT (MSH:4 VALUE: ATSU_HEALTHCURRENT) AACH Emergency Department √ RELIANCE (MSH:4 VALUE: AACH_RELIANCE) EHEALTH COLLABORATIVE Abbeville General Hospital √ LOUISIANA HEALTH INFORMATION EXCHANGE (MSH:4 VALUE:AGH_LAHIE) Abrom Kaplan Memorial Hospital √ LOUISIANA HEALTH INFORMATION EXCHANGE (MSH:4 VALUE: AKMH_LAHIE) Acadia General Hospital √ LOUISIANA HEALTH INFORMATION EXCHANGE (MSH:4 VALUE:ACADIAGH_LAHIE) Acadian Medical Center √ LOUISIANA HEALTH INFORMATION EXCHANGE (MSH:4 VALUE:AMC_LAHIE) Acadia‐St. Landry Hospital √ LOUISIANA HEALTH INFORMATION EXCHANGE (MSH:4 VALUE: ALH_LAHIE) Accu Care Urgent Care √ HEALTH CURRENT (MSH:4 VALUE: ACUC_HEALTHCURRENT) Adelante √ HEALTH CURRENT (MSH:4 VALUE: ADL_HEALTHCURRENT) Advanced Clinical Associates √ HEALTH CURRENT (MSH:4 VALUE: ADCA_HEALTHCURRENT) Advanced Healthcare Associates √ IDAHO HEALTH DATA EXCHANGE (MSH:4 VALUE: AHA_IHIE) ADVANCED PRACTICE MEDICAL CLINIC LLC √ UTAH HEALTH INFORMATION NETWORK (MSH:4 VALUE: ADPRME_UHIN) ADVANCED PULMONARY SLEEP DISORDER AND √ UTAH HEALTH INFORMATION -

Patient-Concierge-Service-Brochure
PATIENT CONCIERGE SERVICE The Steadman Clinic delivers the highest standard of orthopaedic care and personal attention to each patient. Included in our patient-focused culture, we offer complimentary Patient Concierge Services to assist with travel, entertainment, dining, activities and other special requests. Please contact our Patient Concierge at 970-479-5898 or [email protected], 8 am to 5 pm Monday thru Friday, to address non-medical inquiries. Please contact The Steadman Clinic number below for medical attention. PHYSICAL ADDRESS Te Steadman Clinic in Edwards, Colorado is 130 miles west of Te Steadman Clinic in Vail, Colorado is 120 miles west of Denver (DEN) and just 20 miles east of the Vail/Eagle County Denver (DEN) and just 30 miles east of the Vail/Eagle County Airport (EGE). Airport (EGE). The Steadman Clinic Edwards Please use the main entrance of Vail Health Hospital through 322 Beard Creek Road the 2018-2019 construction to access Te Steadman Clinic Edwards, CO 81632 Vail. Tis address may be used for driving directions and ofers complimentary valet service. Valet is available at Vail Health from 970-476-1100 8 am to 5 pm Monday thru Friday. The Steadman Clinic Vail Te Steadman Clinic in Frisco, Colorado is 95 miles west of 181 West Meadow Drive, Suite 400 Denver (DEN) and just 55 miles east of the Vail/Eagle County Airport (EGE). Vail, CO 81657 The Steadman Clinic Frisco 970-476-1100 360 Peak One Drive, Suite 340 Frisco, CO 80443 970-476-1100 PATIENT CONCIERGE SERVICE 2 AIR TRANSPORTATION GROUND TRANSPORTATION AIRPORTS DENVER INTERNATIONAL AIRPORT (DEN) SILENT PARTNER LIMOUSINES 8500 Peña Blvd Denver, CO 80249 Private Limousines | $$$ 303-342-2000 970-470-2587 Denver International Airport is located 120 miles, approximately https://www.silentpartnerlimousines.com a 2 hour drive, east of Vail and is a non-stop destination for major Silent Partner Limousines is a HIPAA certifed transportation domestic and international airlines. -

Curriculum Vitae
August 2018 CURRICULUM VITAE NAME: Ernest E. Braxton Jr, MD, MBA, FAANS 37347 US Highway 6, #201 Avon, CO 81620 Work: (970) 393-2366 Mobile: (210)-488-8974 E-mail: [email protected] PERSONAL INFORMATION Date of Birth: April 9, 1975 Place of Birth: Altus, OK Citizenship: United States EDUCATION 06/1993-05/1997 BS United States Air Force Academy, Colorado Springs, Colorado 08/1997-05/2001 MD University of Pennsylvania, Philadelphia, Pennsylvania 07/2001-06/2002 Internship, Wilford Hall Medical Center, Lackland AFB, Texas 07/2003-06/2009 Residency in Neurosurgery, Allegheny General Hospital, Pittsburgh, Pennsylvania 08/2005-05/2007 MBA, Carnegie Mellon University, Pittsburgh, Pennsylvania 07/2008-06/2009 Chief Resident in Neurosurgery, Allegheny General Hospital, Pittsburgh, Pennsylvania CURRENT PROFESSIONAL POSITIONS 07/2017 Private Practice Vail Summit Orthopedics and Neurosurgery 108 South Frontage Road West, Suite 206 Vail, Colorado 81657 BOARD CERTIFICATION 04/2016 Passed, American Board of Neurologic Surgery Boards (ABNS) MEDICAL LICENSURE 2002- Indiana License #0105667A 2010 Maine License #018397 2011 Texas License #N8618 2017 Colorado License #0058687 HONORS/AWARDS 1993 National Defense Service Medal with 1 Service Star 1997 AF Training Ribbon August 2018 1997 AF Outstanding Unit Award with 3 Oak Leaf Clusters 2001 Global War on Terrorism Service Medal 2003 United States Air Force Commendation Medal 2003 Korean Defense Service Medal 2003 Nuclear Deterrence Operations Service Medal 2006 Canfield-Roseman Entrepreneur of the year award 2011 Afghanistan Campaign Medal with 2 Service Stars 2011 Air Force Expeditionary Service Ribbon with Gold Border 2011 NATO Medal 2015 AF Organizational Excellence Award 2017 AF Longevity Service with 3 Oak Leaf Clusters PREVIOUS PROFESSIONAL MILITARY POSITIONS 07/2002-06/2003 General Medical Officer, 51st Medical Group, Osan AB, Korea 08/2009-07/2014 Staff Neurosurgeon, Wilford Hall Medical Center, Lackland AFB, Texas 10/2009-06/2015 Staff Neurosurgeon, Brooke Army Medical Center, Ft. -
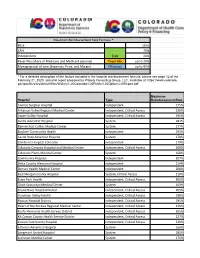
Maximum Reimbursement Rate Formula * Base CAH Type 20% Independent 20% Payer
Maximum Reimbursement Rate Formula * Base 155% CAH 20% Independent Type 20% Payer Mix (share of Medicare and Medicaid patients) Payer Mix up to 30% Managing cost of care (Expenses, Price, and Margin) Efficiency up to 40% * For a detailed description of the factors included in the hospital reimbursement formula, please see page 12 of the February 21, 2020, actuarial report prepared by Wakely Consulting Group, LLC, available at: https://www.colorado. gov/pacific/sites/default/files/Wakely%20Colorado%20Public%20Option%20Report.pdf Maximum Hospital Type Reimbursement Rate Animas Surgical Hospital Independent 175% Arkansas Valley Regional Medical Center Independent, Critical Access 236% Aspen Valley Hospital Independent, Critical Access 195% Avista Adventist Hospital System 181% Banner Fort Collins Medical Center System 177% Boulder Community Health Independent 193% Castle Rock Adventist Hospital System 178% Children's Hospital Colorado Independent 179% Colorado Canyons Hospital and Medical Center Independent, Critical Access 208% Colorado Plains Medical Center System 168% Community Hospital Independent 207% Delta County Memorial Hospital Independent 214% Denver Health Medical Center Independent 208% East Morgan County Hospital System, Critical Access 210% Estes Park Health Independent, Critical Access 205% Good Samaritan Medical Center System 163% Grand River Hospital District Independent, Critical Access 205% Gunnison Valley Health Independent, Critical Access 198% Haxtun Hospital District Independent, Critical Access 195% Heart of the Rockies -

HCR 2 Medicaid Expansion Enrollment and Claims Data SFY 21 Q1HCR 2
John Bel Edwards Dr. Courtney N. Phillips GOVERNOR SECRETARY State of Louisiana Louisiana Department of Health Office of the Secretary January 29, 2021 The Honorable John Bel Edwards, Governor State of Louisiana P.O. Box 94004 Baton Rouge, LA 70804 The Honorable Patrick Page Cortez, President Louisiana State Senate P.O. Box 94183, Capitol Station Baton Rouge, LA 70804-9183 The Honorable Clay Schexnayder, Speaker Louisiana State House of Representatives P.O. Box 94062, Capitol Station Baton Rouge, LA 70804-9062 Re: HCR 2 Quarterly Report SFY 21 Q1 - Medicaid Assessment Report In response to House Concurrent Resolution 2 (HCR 2) of the 2020 First Extraordinary Session, the Louisiana Department of Health (LDH) submits the enclosed report. This report can be viewed on LDH’s website at https://ldh.la.gov/index.cfm/newsroom/detail/5892 the resolution requires LDH to publish on a quarterly basis a report containing data directly related to payment for health care services through the implementation of a health coverage expansion of the Louisiana medical assistance program. The report includes the following: (a) Total Medicaid Expansion enrollment on a monthly basis from July 2020 through September 2020. (b) The average monthly Expansion premium paid to managed care organizations providing benefits and services to eligible Medicaid enrollees and the portion of the premium related to hospital payments for the July 1, 2020 rates. (c) The aggregate Medicaid Expansion claims payment by provider type for July 2020 through September 2020. (d) The total amount of inpatient and outpatient Medicaid Expansion claims paid to hospitals delineated by individual hospital for July Bienville Building ▪ 628 N. -

Public Health Agencies Will Be Administered to Health Care Workers at Local Hospitals That Do Not Have the Capability to Store Vaccine
Release 12/11: Colorado prepares to distribute first shipments of COVID-19 vaccine to health care facilities throughout state Colorado State Joint Information Center <[email protected]> Fri 12/11/2020 9:35 AM To: SOC_JICMediaList <[email protected]> INFORMACIÓN SEGUIDA EN ESPAÑOL AL ESTAR DISPONIBLE FOR IMMEDIATE RELEASE CONTACT: COVID-19 MEDIA LINE: 303-900-2849 (Please leave a message) Email: [email protected] Colorado prepares to distribute first shipments of COVID-19 vaccine to health care facilies throughout state Remote, Colo. (Dec. 11, 2020): In ancipaon of the first shipments of Pfizer and Moderna COVID-19 vaccines in December, the Colorado Department of Public Health and Environment (CDPHE) has collaborated closely with local public health agencies across the state to prepare health care facilies to receive the vaccine. These health care facilies will then distribute the vaccine to frontline health care workers. CDPHE has idenfied locaons across the state with ultra-low temperature freezers to receive the first shipment of the Pfizer vaccine. These locaons were chosen for their unique abilies to store, monitor, and handle vaccines in ultra-cold temperatures (-60°C to -80°C), as well as their willingness to redistribute COVID-19 vaccine(s) to other providers in their regions. The state also considered equitable geographic distribuon as well as transportaon logiscs given expected winter condions in the coming months. To be as equitable as possible, the state also purchased 10 ultra-cold storage units. CDPHE has distributed 8 of these and the remaining two will be distributed today. The federal government will deliver a shipment of the Moderna vaccine shortly aer the first shipment of the Pfizer vaccine. -
Physician Compensation and Productivity Survey Report
2019 Physician Compensation and Productivity Survey Report Survey data effective January 1, 2019 © 2019 SullivanCotter, Inc. All rights reserved. 200 W. Madison Street, Suite 2450 Chicago, IL 60606-3416 2019 PHYSICIAN COMPENSATION AND PRODUCTIVITY SURVEY REPORT Survey data effective January 1, 2019 LICENSE AGREEMENT LICENSE AGREEMENT By accessing or downloading the Survey Report files online or by opening the packaging for this Survey Report, you agree to the terms of this License Agreement (this “Agreement”). If you do not agree to these terms and have not yet accessed or downloaded the Survey Report files or opened the packaging for this Survey Report, you may cancel your online purchase or download at this time or you may return this Survey Report to SullivanCotter, Inc. for a full refund within thirty (30) days of receipt, but you may not access or download the Survey Report files or open the packaging for, or otherwise use, this Survey Report. Accessing or downloading the Survey Report files or opening the packaging, or otherwise using, this Survey Report binds you to this Agreement. This Agreement is entered into by and between SullivanCotter, Inc. ("SullivanCotter") and the purchaser or participant of this Survey Report (the “Licensee”). In consideration of the mutual covenants in this Agreement, SullivanCotter and the Licensee agree as follows: Grant of License. This Survey Report contains the aggregation of compensation data and other data provided to SullivanCotter by its survey participants, statistics, tables, reports, research, aggregations, calculations, data analysis, formulas, summaries, content, text and other information and materials provided to the Licensee by SullivanCotter through any other means, whether digital or hard copy, related thereto (the “Aggregated Data”). -

COVID-19 LIST of VACCINE RECIPIENTS 010821 1 Banner Fort Collins Medical Center
COVID-19 List of vaccine recipients To be as fair and efficient with distribution as possible, Colorado has developed a phased approach to vaccine distribution to save lives and end the crisis that has been brought on by the pandemic as quickly as possible. The Colorado Department of Public Health and Environment (CDPHE) has collaborated closely with local public health agencies across the state to prepare health care facilities to receive the vaccine. These health care facilities will then administer the vaccine to people who want one and are eligible under the phased distribution plan. Colorado is requesting enough vaccines to provide for all Coloradans. Because of supply chain limitations, we expect we will receive regular COVID-19 vaccine allocations from the federal government on a weekly basis. The federal government is determining the allocation amount by the size of every state’s total population and the quantity of ready-to-ship doses from the manufacturers. The following locations have received vaccine shipments: Alamosa County Public Health Department Animas Surgical Hospital Ardas Family Medicine Arkansas Valley Regional Medical Center Aspen Valley Hospital Avista Adventist Hospital Baca County Public Health Agency Banner Columbine Family Practice Loveland Banner East Morgan County Hospital COVID-19 LIST OF VACCINE RECIPIENTS 010821 1 Banner Fort Collins Medical Center Banner Health Clinic Summit View Banner Health Family Care Clinic in Sterling Banner McKee Medical Center Bent County Public Health Bloom Healthcare Physician