(G6PD) Deficiencies in a Vivax-Predom
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Evaluation of the EC Cooperation with the LAO
Evaluation of EC co-operation with the LAO PDR Final Report Volume 2 June 2009 Evaluation for the European Commission This evaluation was commissioned by: Italy the Evaluation Unit common to: Aide à la Décision Economique Belgium EuropeAid Co-operation Office, Directorate-General for Development and PARTICIP GmbH Germany Directorate-General for External Relations Deutsches Institut für Entwicklungspolitik Germany Overseas Development Institute United Kingdom European Institute for Asian Studies Belgium Istituto Complutense de Estudios Internacionales Spain The external evaluation team was composed of Landis MacKellar (team leader), Jörn Dosch, Maija Sala Tsegai, Florence Burban, Claudio Schuftan, Nilinda Sourinphoumy, René Madrid, Christopher Veit, Marcel Goeke, Tino Smaïl. Particip GmbH was the evaluation contract manager. The evaluation was managed by the evaluation unit who also chaired the reference group composed by members of EC services (EuropeAid, DG Dev, DG Relex, DG Trade), the EC Delegations in Vientiane and Bangkok and a Representative of the Embassy of the LAO PDR. Full reports of the evaluation can be obtained from the evaluation unit website: http://ec.europa.eu/europeaid/how/evaluation/evaluation_reports/index_en.htm The opinions expressed in this document represent the authors’ points of view, which are not necessarily shared by the European Commission or by the authorities of the countries concerned. Evaluation of European Commission’s Cooperation with ASEAN Country Level Evaluation Final Report The report consists of 2 volumes: Volume I: FINAL REPORT Volume II: Annexes VOLUME I: DRAFT FINAL REPORT 1. Introduction 2. Development Co-operation Context 3. EC strategy and the logic of EC support 4. Findings 5. Conclusions 6. -

World Bank Document
Document of The World Bank Report No.: 62073 Public Disclosure Authorized Public Disclosure Authorized PROJECT PERFORMANCE ASSESSMENT REPORT LAO PEOPLE’S DEMOCRATIC REPUBLIC PROVINCIAL INFRASTRUCTURE PROJECT (CREDIT 3131) June 10, 2011 Public Disclosure Authorized IEG Public Sector Evaluation Independent Evaluation Group Public Disclosure Authorized Currency Equivalents (annual averages) Currency Unit = Laotian Kip 1998 US$1.00 Kip 3,298 1999 US$1.00 Kip 7,102 2000 US$1.00 Kip 7,888 2001 US$1.00 Kip 8,955 2002 US$1.00 Kip 10,056 2003 US$1.00 Kip 10,569 2004 US$1.00 Kip 10,585 2005 US$1.00 Kip 10,655 2006 US$1.00 Kip 10,160 2007 US$1.00 Kip 9,603 2008 US$1.00 Kip 8,744 2009 US$1.00 Kip 8,393 Abbreviations and Acronyms ASEAN Association of South-East Asian Nations CAS Country Assistance Strategy DCA Development Credit Agreement ERR Economic Rate of Return GOL Government of the Lao PDR ICR Implementation Completion Report IEG Independent Evaluation Group Lao PDR Lao People’s Democratic Republic M&E Monitoring and Evaluation MPH Ministry of Public Health MPWT Ministry of Public Works and Transport NAMPAPA (MPWT) Water Supply Enterprise (for urban areas) NAMSAAT (MPH) Institute of Clean Water (for rural areas) NEM New Economic Mechanism PAD Project Appraisal Document PPAR Project Performance Assessment Report Fiscal Year Government: October 1 – September 30 Director-General, Independent Evaluation : Mr. Vinod Thomas Director, IEG Public Sector Evaluation : Ms. Monika Huppi (acting) Manager, IEG Public Sector Evaluation : Ms. Monika Huppi Task Manager : Mr. -

LAOS Opium Survey 2003
LAOS Opium Survey 2003 June 2003 Laos Opium Survey 2003 Abbreviations GOL Government of Lao PDR ICMP UNODC Illicit Crop Monitoring Programme LCDC Lao National Commission for Drug Control and Supervision NSC Lao National Statistics Centre PFU Programme Facilitation Unit UNODC United Nations Office on Drugs and Crime Acknowledgements The following organisation and individuals contributed to the implementation of the 2003 opium survey in Lao PDR (Laos) and the preparation of the present report: Government of Lao PDR: Lao National Commission for Drug Control and Supervision National Statistics Centre National Geographic Department Ministry of Agriculture and Forestry The implementation of the survey would not have been possible without the support from the local administrations and the dedicated work of the field surveyors. UNODC: Shariq Bin Raza, Officer-in-charge, UNODC (Field Office - Laos) Leik Boonwaat, Programme Facilitation Unit UNODC (Field Office - Laos) Hakan Demirbuken, Survey data and systems Analyst (ICMP- Research Section) Denis Destrebecq, Survey technical supervision (ICMP-Research Section) Giovanni Narciso, Regional Illicit Crop Monitoring Expert (ICMP-Field Office Myanmar) Thibault le Pichon, Illicit Crop Monitoring Programme Manager (ICMP- Research Section) The implementation of UNODC’s Illicit Crop Monitoring Programme in Southeast Asia and the 2003 Laos Opium survey were made possible thanks to financial support from the Governments of the USA, Japan and Italy. NOTE: This publication has not been formally edited. Laos Opium Survey 2003 LAOS OPIUM SURVEY 2003 Executive Summary Although far behind Afghanistan and Myanmar, the remote and mountainous areas of Northern Laos, which border Thailand, Myanmar, China and Vietnam, have consistently come in third place as a source of the world’s illicit opium and heroin during the last ten years. -
LIWG Newsletter Volume 6
The 6th quarterly Newsletter of Land Information Working Group LIWG Newsletter Volume 6 January - March 2019 VOL.6 Welcome to the 6th issue of LIWG Newsletter. The issue covers activities from January – March 2019. In this issue, we have provided updates on activities implemented by the Secretariat, its members and its network related to land advocacy, natural resource protection, and the promotion of human rights related to land and natural resource tenures. For more updates, please keep following us on our Webpage and Facebook, and if you have comments and suggestions, please send us an email at: [email protected] Stories inside: Highlight story... Meeting and workshop organized by LIWG Working Group/Taskforce Meetings and Workshops which the LIWG secretariat attended LIWG‟s Initiatives and members Story of the months Communication and News updates LIWG next quarterly topics (April – June 2019) 400 year tea trees in Phongsaly district, Phongsaly province. Photo by LIWG Key fact: “ 60,000 people from 12,000 families in more than From visiting different communities, we have learnt the 200 villages across Laos are relocated to make way importance of land tenure security to local farmers because for power projects. Top 4 dam projects relocated they rely on land to produce tea or another crop-like cardamom people the most are: Nam Tha 1 dam, Nam Theun 2 for making their livelihoods and earning incomes. Dam, Xayaburi dam, and Theun-Hinboun Dam.” Read more inside on page 2….. - Source: Vientiane Times and ABC Laos News LIWG Newsletter, Issue 6: January - March 2019 2 I. Meeting and workshop organized by LIWG secretariat 1. -

World Bank Document
Document of The World Bank FOR OFFICIAL USE ONLY Public Disclosure Authorized Report No: PAD1371 INTERNATIONAL DEVELOPMENT ASSOCIATION PROJECT APPRAISAL DOCUMENT ON A PROPOSED CREDIT Public Disclosure Authorized IN THE AMOUNT OF SDR 9.4 MILLION (US$13.2 MILLION EQUIVALENT) AND A PROPOSED GRANT IN THE AMOUNT OF SDR 9.4 MILLION (US$13.2 MILLION EQUIVALENT) TO THE Public Disclosure Authorized LAO PEOPLE'S DEMOCRATIC REPUBLIC FOR A HEALTH GOVERNANCE AND NUTRITION DEVELOPMENT PROJECT June 2, 2015 Health, Nutrition, and Population Global Practice East Asia and Pacific Region Public Disclosure Authorized This document has a restricted distribution and may be used by recipients only in the performance of their official duties. Its contents may not otherwise be disclosed without World Bank authorization. CURRENCY EQUIVALENTS (Exchange Rate Effective April 30, 2015) Currency Unit = Lao Kip (LAK) 1 LAK = US$0.000123 US$ 1 = LAK 8,077 SDR 1 = US$1.40642 FISCAL YEAR October 1 – September 30 ABBREVIATIONS AND ACRONYMS ADALY Averted Disability Adjusted Life Years ADB Asian Development Bank ANC Ante Natal Care CIEH Center for Information and Education in Health CLTS Community-led Total Sanitation CNP Community Nutrition Project CRVS Civil Registration and Vital Statistics DA Designated Account DG Director General DHHP Department of Hygiene and Health Promotion DHIS2 District Health Information System DHO District Health Office DLI Disbursement Linked Indicators DPD Deputy Project Director DPIC Department of Planning and International Cooperation DPT -

Ethnic Group Development Plan LAO: Northern Rural Infrastructure
Ethnic Group Development Plan Project Number: 42203 May 2016 LAO: Northern Rural Infrastructure Development Sector Project - Additional Financing Prepared by Ministry of Agriculture and Forestry for the Asian Development Bank. This ethnic group development plan is a document of the borrower. The views expressed herein do not necessarily represent those of ADB's Board of Directors, Management, or staff, and may be preliminary in nature. Your attention is directed to the “terms of use” section of this website. In preparing any country program or strategy, financing any project, or by making any designation of or reference to a particular territory or geographic area in this document, the Asian Development Bank does not intend to make any judgments as to the legal or other status of any territory or area. Ethnic Group Development Plan Nam Beng Irrigation Subproject Tai Lue Village, Lao PDR TABLE OF CONTENTS Topics Page LIST OF ABBREVIATIONS AND TERMS v EXECUTIVE SUMMARY A10-1 A. Introduction A10-1 B. The Nam Beng Irrigation Subproject A10-1 C. Ethnic Groups in the Subproject Areas A10-2 D. Socio-Economic Status A10-2 a. Land Issues A10-3 b. Language Issues A10-3 c. Gender Issues A10-3 d. Social Health Issues A10-4 E. Potential Benefits and Negative Impacts of the Subproject A10-4 F. Consultation and Disclosure A10-5 G. Monitoring A10-5 1. BACKGROUND INFORMATION A10-6 1.1 Objectives of the Ethnic Groups Development Plan A10-6 1.2 The Northern Rural Infrastructure Development Sector Project A10-6 (NRIDSP) 1.3 The Nam Beng Irrigation Subproject A10-6 2. -

Download TDM Thesis
Tangled Affair or Fruitful Relationship? Foreign Aid Involvement in the Tourism PoliCy ProCess Case Study of Lao PDR Nadine Fiaux Master Degree Dissertation Tourism Destination Management September 2011 Tangled Affair or Fruitful Relationship? Foreign Aid Involvement in the Tourism Policy Process Case Study of Lao PDR Master Program Tourism Destination Management Master Degree Dissertation September 2011 Nadine Fiaux Student at the NHTV University of Applied Sciences, Breda NL Student ID: 102390 I hereby declare that this dissertation is wholly the work of Nadine Fiaux. Any other contributors or sources have either been referenced in the prescribed manner or are listed in the acknowledgements together with the nature and the scope of their contribution. PREFACE AND ACKNOWLEDGEMENTS Throughout my studies in tourism the area of tourism policy and planning has always interested me. The huge importance that appropriate planning can have on the development of tourism destinations is intriguing, especially after having travelled to many countries and experienced examples of tourism development going wrong first hand. The task that tourism planners nowadays have if they want to develop their destination in a sustainable way is highly complex and challenging and personally I have always liked a challenge. This is the reason why it was clear to me that my dissertation was to be related to the topic of tourism policy, although I had not decided on which facet to investigate. During the fieldtrip we did between February and April 2011 in the Asia-Pacific Region visiting Australia, Cambodia and Bali I fell in love with Southeast Asia making me want to stay in this region for my research. -

The Loss of the Ou River by Saimok
The Loss of the Ou River By Saimok “Talaeng taeng talam bam!” Sounds of warning: “I am coming to get you!” Khmu children play hide and seek along the banks of the Ou River in North- ern Laos. Ngoi district, Luangprabang province. November 2019. photo by author The Loss of 2 the Ou River The first time I saw the Ou River I was mesmer- Arriving in the northern province of Phongsa- ized by its beauty: the high karst mountains, the ly province by truck, I was surprised that this dense jungle, the structure of the river and the remote corner of the land of a million elephants flow of its waters. The majority of the people felt like a new province of China. Chinese lux- along the Ou River are Khmu, like me. We under- ury cars sped along the bumpy road, posing a stand one another. Our Khmu people belong to danger to the children playing along the dusty specific clans, and my Sim Oam family name en- roadside. In nearly every village I passed, the sures the protection and care of each Sim Oam newer concrete homes featured tiles bearing clan member I meet along my journey. Mao Zedong’s image. “I’ve seen this image in many homes in this area. May I ask who he is?” I Sim Oam is similar to a kingfisher, and as mem- asked the village leader at a local truck stop. bers of the Sim Oam clan, we must protect this animal, and not hunt it. If a member of our clan breaks the taboo and hunts a sim oam, his teeth will fall out and his eyesight will become cloudy. -
Study of the Provincial Context in Oudomxay 1
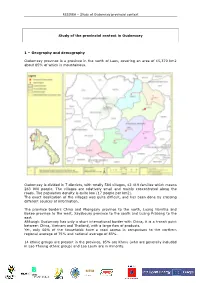
RESIREA – Study of Oudomxay provincial context Study of the provincial context in Oudomxay 1 – Geography and demography Oudomxay province is a province in the north of Laos, covering an area of 15,370 km2 about 85% of which is mountainous. Oudomxay is divided in 7 districts, with totally 584 villages, 42 419 families which means 263 000 people. The villages are relatively small and mainly concentrated along the roads. The population density is quite low (17 people per km2). The exact localization of the villages was quite difficult, and has been done by crossing different sources of information. The province borders China and Phongsaly province to the north, Luang Namtha and Bokeo province to the west, Xayaboury province to the south and Luang Prabang to the east. Although Oudomxay has only a short international border with China, it is a transit point between China, Vietnam and Thailand, with a large flow of products. Yet, only 66% of the households have a road access in comparison to the northern regional average of 75% and national average of 83%. 14 ethnic groups are present in the province, 85% are Khmu (who are generally included in Lao Theung ethnic group) and Lao Loum are in minority. MEM Lao PDR RESIREA – Study of Oudomxay provincial context 2- Agriculture and local development The main agricultural crop practiced in Oudomxay provinces is corn, especially located in Houn district. Oudomxay is the second province in terms of corn production: 84 900 tons in 2006, for an area of 20 935 ha. These figures have increased a lot within the last few years. -

Market Chain Assessments
Sustainable Rural Infrastructure and Watershed Management Sector Project (RRP LAO 50236) Market Chain Assessments February 2019 Lao People’s Democratic Republic Sustainable Rural Infrastructure and Watershed Management Sector Project Sustainable Rural Infrastructure and Watershed Management Sector Project (RRP LAO 50236) CONTENTS Page I. HOUAPHAN VEGETABLE MARKET CONNECTION 1 A. Introduction 1 B. Ban Poua Irrigation Scheme 1 C. Markets 1 D. Market Connections 4 E. Cross cutting issues 8 F. Conclusion 9 G. Opportunity and Gaps 10 II. XIANGKHOUANG CROP MARKETS 10 A. Introduction 10 B. Markets 11 C. Conclusion 17 D. Gaps and Opportunities 17 III. LOUANGPHABANG CROP MARKET 18 A. Introduction 18 B. Markets 18 C. Market connections 20 D. Cross Cutting Issues 22 E. Conclusion 23 F. Opportunities and Gaps 23 IV. XAIGNABOULI CROP MARKETS 24 A. Introduction 24 B. Market 24 C. Market Connection 25 D. Conclusion 28 E. Opportunities and Gaps 28 V. XIANGKHOUANG (PHOUSAN) TEA MARKET 29 A. Introduction 29 B. Xiangkhouang Tea 30 C. Tea Production in Laos 30 D. Tea Markets 31 E. Xiangkhouang Tea Market connection 33 F. Institutional Issues 38 G. Cross Cutting Issues 41 H. Conclusion 41 I. Opportunities and Gaps 42 VI. XIANGKHOUANG CATTLE MARKET CONNECTION ANALYSIS 43 A. Introduction 43 B. Markets 43 C. Export markets 44 D. Market Connections 46 E. Traders 49 F. Vietnamese Traders 49 G. Slaughterhouses and Butchers 50 H. Value Creation 50 I. Business Relationships 50 J. Logistics and Infrastructure 50 K. Quality – Assurance and Maintenance 50 L. Institutions 50 M. Resources 51 N. Cross Cutting Issues 51 O. Conclusion 51 P. -

8Th FIVE-YEAR NATIONAL SOCIO- ECONOMIC DEVELOPMENT PLAN
Lao People’s Democratic Republic Peace Independence Unity Prosperity 8th FIVE-YEAR NATIONAL SOCIO- ECONOMIC DEVELOPMENT PLAN (2016–2020) (Officially approved at the VIIIth National Assembly’s Inaugural Session, 20–23 April 2016, Vientiane) Ministry of Planning and Investment June 2016 8th FIVE-YEAR NATIONAL SOCIO-ECONOMIC DEVELOPMENT PLAN (2016–2020) (Officially approved at the VIIIth National Assembly’s Inaugural Session, 20–23 April 2016, Vientiane) Ministry of Planning and Investment June 2016 FOREWORD The 8th Five-Year National Socio-economic Development Plan (2016–2020) “8th NSEDP” is a mean to implement the resolutions of the 10th Party Conference that also emphasizes the areas from the previous plan implementation that still need to be achieved. The Plan also reflects the Socio-economic Development Strategy until 2025 and Vision 2030 with an aim to build a new foundation for graduating from LDC status by 2020 to become an upper-middle-income country by 2030. Therefore, the 8th NSEDP is an important tool central to the assurance of the national defence and development of the party’s new directions. Furthermore, the 8th NSEDP is a result of the Government’s breakthrough in mindset. It is an outcome- based plan that resulted from close research and, thus, it is constructed with the clear development outcomes and outputs corresponding to the sector and provincial development plans that should be able to ensure harmonization in the Plan performance within provided sources of funding, including a government budget, grants and loans, -

Northern Uplands Promoting Climate Resilience (NU PCR)
ANNEX VI PROJECT COMPLETION NARRATIVE REPORT (March 2014 – February 2018) Northern Uplands Promoting Climate Resilience (NU PCR) Contract Number: DCI-ENV/2014/303-318 This project implemented by January 2012 Page 1 of 55 DCI-ENV/2014/303-318 This publication has been produced with the assistance of the European Union. The contents of this publication are the sole responsibility of CARE and can in no way be taken to reflect the views of the European Union. • This report must be completed and signed by the Contact person. • The information provided below must correspond to the financial information that appears in the financial report. • Please complete the report using a typewriter or computer • Please expand the paragraphs as necessary. • Please refer to the Special Conditions of your grant contract and send one copy of the report to each address mentioned. • The Contracting Authority will reject any incomplete or badly completed reports. • The answer to all questions must cover the reporting period as specified in point 1.6. 1. Description 1.1. Name of beneficiary of grant contract: CARE Denmark 1.2. Name and title of the Contact person: Mr. FlemminG Gjedde Nielsen, Programme Coordinator, CARE Denmark 1.3. Name of partners in the Action: CCL, SAEDA 1.4. Title of the Action: Northern Uplands - Promoting Climate Resilience (NU-PCR) 1.5. Contract number: DCI-ENV/2014/303-318 1.6. Start date and end date of the reporting period: 12.3.2014 – 11.3.2018 1.7. Target country(ies) or region(s): Laos, Phongsaly, Gnot Ou, Samphan and Mai districts 1.8.