An International Collaboration to Unravel Hepatitis C Resistance
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Urban Aerosol Size Distributions Over the Mediterranean City of Barcelona, NE Spain
Discussion Paper | Discussion Paper | Discussion Paper | Discussion Paper | Atmos. Chem. Phys. Discuss., 12, 16457–16492, 2012 Atmospheric www.atmos-chem-phys-discuss.net/12/16457/2012/ Chemistry ACPD doi:10.5194/acpd-12-16457-2012 and Physics © Author(s) 2012. CC Attribution 3.0 License. Discussions 12, 16457–16492, 2012 This discussion paper is/has been under review for the journal Atmospheric Chemistry Urban aerosol size and Physics (ACP). Please refer to the corresponding final paper in ACP if available. distributions over the Mediterranean city of Urban aerosol size distributions over the Barcelona, NE Spain Mediterranean city of Barcelona, NE Spain M. Dall’Osto et al. 1 2 1 3,* 1 M. Dall’Osto , D.C.S. Beddows , J. Pey , S. Rodriguez , A. Alastuey , Title Page R. M. Harrison2,4, and X. Querol1 Abstract Introduction 1Institute for Environmental Assessment and Water Research (IDÆ-CSIC),´ Barcelona, Spain 2National Centre for Atmospheric Science, School of Geography, Earth and Environmental Conclusions References Sciences University of Birmingham, Edgbaston Birmingham B15 2TT, UK Tables Figures 3University of Huelva (Spain) at the Izana Atmospheric Observatory, INM-CSIC, La Marina 20, 6a planta, 38071, Santa Cruz de Tenerife, Canary Islands, Spain 4Centre of Excellence in Environmental Studies, King Abdulaziz University, P.O. Box 80203, J I Jeddah (21589), Saudi Arabia J I *now at: Izana˜ Atmospheric Research Centre, AEMET, Joint Research Unit to CSIC “Studies on Atmospheric Pollution”, La Marina 20, Planta 6, 38071 Santa Cruz de Tenerife, Canary Back Close Islands, Spain Full Screen / Esc Received: 1 June 2012 – Accepted: 14 June 2012 – Published: 4 July 2012 Correspondence to: M. -

Download Company Profile
TENERIFE / BARCELONA COMPANY PROFILE 2021 KID CONTENT CREATOR [email protected] Calle Jose Antonio Zarate y Penichet (Oficina 7) 38001 Santa Cruz deTenerife - Spain Tenerife +34 / 922 928 748 Calle Gracia 1 (Principal 2) 08012 Barcelona - Spain Barcelona +34 / 932 177 025 The team We offer the With over 10 years’ experience in the International Kids Animation industry, Tomavision offers following services: a wide range of creative and service-oriented solutions. We are an independent production company located in Barcelona and Tenerife (Spain), where we develop and produce Premium Kids Content, offering co-production and service work under the Canary Islands’ Tax Incentives Scheme, with up to 50% Tax Rebate. Our filmography includes well established Animated Properties, TV Series and Short Films critically acclaimed and multi-awarded. Emmy nominated Director Mercedes Marro oversees all creative aspects of productions Top Level 2D and 3D Animation Services via Industry Standards such as Toon Boom Harmony and Maya pipeline - We offer traditional animation services such as Clean-Up, Tones, FX and Ink & Paint. Scriptwriting: we work with some of the most talented scriptwriters, offering multiple scriptwriting services such as original content, punch-ups, rewrites, international adaptations, pitch bibles, springboards, etc. Mercedes Marro Pierre Nothman Carlos Roca Blanca Vivas Javier Martínez Director Executive Producer Studio Director Marketing & Communication Director Assistant Our Storyboard and Animation Team manages Toon Boom Storyboard pro Software package, creating accurate storyboards to capture the essence of each scene. We are a big believer in the power of well-executed while managing the company alongside executive producer Pierre Nothman. Storyboards and Animatics. -
Progress in Reconstructing Long Term Global Sea Level Changes
Historical tide-gauge sea-level observations in Alicante and Santander (Spain) since the 19th century Marta Marcos, Bernat Puyol, Angel Amores, Begoña Pérez Gómez, M. Angeles Fraile, Stefan A. Talke © Marcos et al. All rights reserved Spanish sea level historical archives at IGN Sea-level records stored in logbooks are archived at the IGN headquarters. This work is a new effort to recover and quality-control two of the longest and most relevant (in red) Historical data sets First year of data Alicante I 1874 ~140 years Alicante II 1957 Almería 1972 Cartagena 1927 Ceuta 1908 Marcos et al (2011) Cádiz 1880 doi:10.1029/2011JC007558 Coruña 1950 ~49 years Santander 1876 Marcos et al (2013) Santa Cruz de Tenerife 1927 doi:10.1002/jgrc.20377 © Marcos et al. All rights reserved Two new tide gauge stations recovered from archives at IGN (Spain) Example of hand-written logbooks for one month of data in Santander Location and time span of the new sea- level time series © Marcos et al. All rights reserved Santander tide gauge 1876-1924 Tide gauge type/name Period of operation Temporal sampling Adie (floating gauge) 07/1876-1914 and 1920-1924. Daily averages Mier (syphon gauge) 01/1920-07/1925 Daily averages Iglesias (syphon gauge) 01/1925-12/1928 Daily averages © Marcos et al. All rights reserved Santander tide gauge 1876-1924 High-precision levelling surveys in the vicinity of the tide gauges have been carefully investigated to provide the vertical distances among the benchmarks as well as their displacements over time Schematic view of the levelling surveys Final result of the tide gauge benchmarks for every instrument, location and period © Marcos et al. -

Employment Law Area
EMPLOYMENT LAW AREA MADRID | SEVILLA | SANTA CRUZ DE TENERIFE | LAS PALMAS DE GRAN CANARIA I CÓRDOBA | HUELVA LABORAL 3 4 5 Abstract The Firm 4 Philosophy 5 Employment Law Area Presentation 7 List of services 8 Members of Madrid Office 11 Members of Sevilla Office 15 Members of Santa Cruz de Tenerife and Las Palmas de Gran Canaria Offices 23 Figures 28 Offices 30 6 The Firm MONTERO|ARAMBURU has had an office in Santa Cruz de ABOGADOS was founded in Tenerife since 1980 and another in Seville(Spain) in 1971 as a tax Las Palmas de Gran Canaria since boutique and continued as such 2003. until 1992. The firm boasted over 150 lawyers At that time, the firm experienced a covering all areas of law. The firm’s diversification process that resulted clients come from a broad spectrum in the full-fledged legal service both in terms of their operating provider and multi-disciplinary law sector and the size of their firm that it is today. operations. As such, they include large industrial corporations, Since its beginnings, influential wine production MONTERO|ARAMBURU companies and top real estate ABOGADOS has achieved high firms, but also traditional family prestige, not only locally but companies and “SMEs” operating throughout all of Western in a variety of fields. Of course, Andalusia, where it has offices clients also include renowned established in Seville, Cordoba and professionals and entrepreneurs Huelva and, since 2014, in Madrid. in addition to partners in deeply Its area of influence also extends to rooted social non-profit companies the Canary Islands, where the firm and institutions. -

Free Trade Between the Canary Islands and Spanish America
FREE TRADE BETWEEN THE CANARY ISLANDS AND SPANlSH AMERICA This paper is based upon the results of a long scale research project undertaken between 1977 and 1984 in Sevilla, Simancas and Madrid. Its general aim has been to determine the results for the commercial relations between Spain and its American empire of the introduction of «free trade~,in the second half of the eighteenth century. The details of the free trade legislation, and its motives, are well-known; to a certain extent so, too, are its consequences. There has been disagreement, however, among historians about the size of the increase in trade, the re- lative importance of national and foreign goods in exports to America, and the shares of trade enjoyed by the thirteen Spa- nish ports enfranchised en 1778. The most important sources for the study are the registers of the individual ships which sai- led from and returned to Spain during the period 1778 - 1796, which are located in the Archivo General de Indias, Sevilla, The year 1796 has been chosen as the terminal point for the study because after that year the long cycle of war between Spain and Britain destroyed the pattern of trade established by the reforms of 1765 - 1789. The paper begins with a summary of the principal conclu- ~iuiisuf the fiisi part uf ihe pi~jeci,which was cüiiipleieíf en 198 1. This was concerned with exports from Spain to America. It describes and explains the average increase of 400 per cent in the value of exports between 1778 and 1796, the increase in the share oftotal exports enjoyed by national products (from 38 per cent in 1778 to 61 in 1794), and the relative shares of the ex- pert tra& enjcyed by the thirtee:: enfrunchised Spanish ports. -
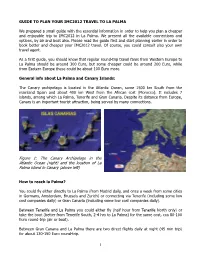
Right) and the Location of La Palma Island in Canary (Above Left
GUIDE TO PLAN YOUR IMC2012 TRAVEL TO LA PALMA We prepared a small guide with the essential information in order to help you plan a cheaper and enjoyable trip to IMC2012 in La Palma. We present all the available connections and options, by air and boat also. Please read the guide first and start planning earlier in order to book better and cheaper your IMC2012 travel. Of course, you could consult also your own travel agent. As a first guide, you should know that regular round-trip travel fares from Western Europe to La Palma should be around 300 Euro, but some cheaper could be around 200 Euro, while from Eastern Europe these could be about 100 Euro more. General info about La Palma and Canary Islands: The Canary archipelago is located in the Atlantic Ocean, some 1500 km South from the mainland Spain and about 400 km West from the African cost (Morocco). It includes 7 islands, among which La Palma, Tenerife and Gran Canaria. Despite its distance from Europe, Canary is an important tourist attraction, being served by many connections. Figure 1: The Canary Archipelago in the Atlantic Ocean (right) and the location of La Palma island in Canary (above left) How to reach la Palma? You could fly either directly to La Palma (from Madrid daily, and once a week from some cities in Germany, Amsterdam, Brussels and Zurich) or connecting via Tenerife (including some low cost companies daily) or Gran Canaria (including some low cost companies daily). Between Tenerife and La Palma you could either fly (half hour from Tenerife North only) or take the boat (better from Tenerife South, 2-4 hrs to La Palma) for the same cost, cca 80-100 Euro round-trip (air or boat). -

Staging Parkinson's Disease Combining Motor and Nonmotor
Hindawi Parkinson’s Disease Volume 2021, Article ID 8871549, 16 pages https://doi.org/10.1155/2021/8871549 Research Article Staging Parkinson’s Disease Combining Motor and Nonmotor Symptoms Correlates with Disability and Quality of Life D. Santos Garcı´a ,1 T. De Deus Fonticoba,2 J. M. Paz Gonza´lez,1 C. Cores Bartolome´,1 L. Valde´s Aymerich,1 J. G. Muñoz Enrı´quez,1 E. Sua´rez,2 S. Jesu´ s,3,4 M. Aguilar,5 P. Pastor,5 L. L. Planellas,6 M. Cosgaya,6 J. Garcı´a Caldentey,7 N. Caballol,8 I. Legarda,9 J. Herna´ndez Vara,10 I. Cabo,11 L. Lo´pez Manzanares,12 I. Gonza´lez Aramburu,4,13 M. A. A´ vila Rivera,14 M. J. Catala´n,15 V. Nogueira,16 V. Puente,17 J. M. Garcı´a Moreno,18 C. Borrue´,19 B. Solano Vila,20 M. A´ lvarez Sauco,21 L. Vela,22 S. Escalante,23 E. Cubo,24 F. Carrillo Padilla,25 J. C. Martı´nez Castrillo,26 P. Sa´nchez Alonso,27 M. G. Alonso Losada,28 N. Lo´pez Ariztegui ,29 I. Gasto´n,30 J. Kulisevsky,4,31 M. Bla´zquez Estrada,32 M. Seijo,11 J. Ru´ iz Martı´nez,33 C. Valero,34 M. Kurtis,35 O. de Fa´bregues,10 J. Gonza´lez Ardura,36 C. Orda´s,37 L. Lo´pez Dı´az,38 P. Mir,4,3 P. Martinez-Martin ,4 and COPPADIS Study Group39 1CHUAC, Complejo Hospitalario Universitario de A Coruña, A Coruña, Spain 2CHUF, Complejo Hospitalario Universitario de Ferrol, A Coruña, Spain 3Unidad de Trastornos del Movimiento, Servicio de Neurolog´ıa y Neurofisiolog´ıa Cl´ınica, Instituto de Biomedicina de Sevilla, Hospital Universitario Virgen del Roc´ıo/CSIC/Universidad de Sevilla, Seville, Spain 4CIBERNED (Centro de Investigaci´on Biom´edica en Red Enfermedades -

N E W S R E L E a S E
N E W S R E L E A S E CONTACT: Katherine Blodgett/The Philadelphia Orchestra Director of Public/Media Relations phone: 215.893.1939 e-mail: [email protected] FOR IMMEDIATE RELEASE DATE: December 19, 2008 THE PHILADELPHIA ORCHESTRAORCHESTRA,, WITH CHRISTOPH ESCHENBACHESCHENBACH CONDUCTING, TOURS EUROPE AND THE CANARY ISLANDS ThreeThree----weekweek tour includes visits to the Canary Islands, Spain, Portugal, Luxembourg, Hungary, and Austria ––– violinist Leonidas Kavakos joins tour as soloist (Philadelphia, December 19, 2008) – The Philadelphia Orchestra embarks on its 2009 Tour of Europe and the Canary Islands on January 26, 2009. Under the leadership of Christoph EschenbachEschenbach, the Orchestra visits nine cities in five countries making first visits to Santa Cruz de TenerifeTenerife, Las Palmas de Gran CanariaCanaria, LuxembourgLuxembourg, and BudapestBudapest. The three-week tour, which concludes February 14, also includes performances in BarcelonaBarcelona, LisbonLisbon, MadridMadrid, ValenciaValencia, and ViennaVienna. Violinist Leonidas Kavakos joins The Philadelphia Orchestra for eight of the tour’s concerts. ToToTourTo ur Repertoire and Artists On the 2009 tour, The Philadelphia Orchestra performs Prokofiev’s Fifth Symphony, Schubert’s Symphony in C major (“Great”), Pintscher’s Osiris , Bruckner’s Sixth Symphony, Schoenberg’s Chamber Symphony No. 1, and Beethoven’s Overture to Egmont . Guest soloist Leonidas Kavakos performs Bartók’s Violin Concerto No. 2 with the Orchestra on concerts in Santa Cruz de Tenerife, Las Palmas de Gran Canaria, and Luxembourg, and performs Sibelius’s Violin Concerto on concerts in Lisbon, Madrid, Valencia, Budapest, and Vienna. Conductor Christoph EschenbachEschenbach, music director of The Philadelphia Orchestra from 2003 to 2008, leads the 2009 Tour of Europe and the Canary Islands. -

MEDICAL SERVICES LIST Las Palmas De Gran Canaria, Consular
1 Embassy of the United States of America MEDICAL SERVICES LIST Las Palmas De Gran Canaria, Consular Agency Consular District of Madrid, Revised in July 2018 DISCLAIMER: The following list of hospitals and doctors has been compiled to assist American citizens in Spain in the event medical services are required. The U.S. Embassy Madrid, Spain assumes no responsibility or liability for the professional ability or reputation of, or the quality of services provided by, the medical professionals, medical facilities or air ambulance services whose names appear on the following lists, but great care has been exercised to include only those who are thought to be capable, reliable and ethical. Inclusion on this list is in no way an endorsement by the Department of State or the U.S. Embassy/Consulate. Names are listed alphabetically, and the order in which they appear has no other significance. Additionally, it has not been possible to include in this listing all of the capable physicians practicing in the Canary Islands. Users of this list should inquire in advance about hours of operations and fees. Important: American Citizens living or traveling abroad should be sure they have adequate medical insurance that will cover expenses incurred abroad. Medicare and Medicaid are only valid in the United States. Some private American medical insurance companies will pay for expenses abroad, but most require that the patient pay the bill first, then file for reimbursement. Hospitals and health care providers will expect payment if you are not covered by the Spanish health care system. The United States Embassy does not have funding to help cover medical expenses of American citizens in Spain. -

Alejandro S. Borlaff, Phd About Me: NASA Postdoctoral Fellow at the Ames Research Center
Alejandro S. Borlaff, PhD About me: NASA Postdoctoral Fellow at the Ames Research Center. Astrophysicist with background in galactic and extragalactic research. Skilled in data analysis and statistics. Large experience with observa- tional methods and instrumentation. I have participated in more than 50 observing nights in four different observatories. Research experience Alejandro S. Borlaff NASA Postdoctoral Program Fellowship [email protected] The ultra-low surface brightness Universe with HST and beyond https://borlaff. November 2019 - Present github.io/ NASA Ames Research Center, Moffett Field (California, USA) Madrid (Spain) Skype: a_borlaff Deep imaging is the next frontier for many studies in galaxy evolution Twitter: @asborlaff and cosmology. Nevertheless, as we increase the depth of the astronomi- GitHub: Borlaff cal images more and more instrumental effects prevent us from obtaining (+34) 635223247 a clear detection of the darkest regions of the Universe. The main objec- tive of this proposal is to use the archive deep cosmological observations of the Hubble Space Telescope (HST), simulations, and data from other telescopes to prepare the future observations with Euclid, James Webb Space Telescope (JWST) and other space observatories. PI: Pamela M. Marcum ([email protected]). European Space Agency: ESA - ESAC Faculty Research Specialist Image processing for low surface brightness emission with Euclid April 2019 - November 2019 ESA - ESAC, European Space Astronomy Centre, (Madrid, Spain) The main objective is to determine the capabilities of Euclid to analyse the low surface brightness Universe, as an extension to the primary sci- entific mission, enabling the study the darkest regions of the Universe. PIs: Bruno Altieri ([email protected]) and Roland Vavrek. -

CMN / EA International Provider Network HOSPITALS/CLINICS
CMN / EA International Provider Network HOSPITALS/CLINICS As of March 2010 The following document is a list of current providers. The CMN/EA International Provider Network spans approximately 200 countries and territories worldwide with over 2000 hospitals and clinics and over 6000 physicians. *Please note that the physician network is comprised of private practices, as well as physicians affiliated with our network of hospitals and clinics. Prior to seeking treatment, Members must call HCCMIS at 1-800-605-2282 or 1-317-262-2132. A designated member of the Case Management team will coordinate all healthcare services and ensure that direct billing arrangements are in place. Please note that although a Provider may not appear on this list, it does not necessarily mean that direct billing cannot be arranged. In case of uncertainty, it is advised Members call HCCMIS. CMN/EA reserves the right, without notice, to update the International Provider Network CMN/EA International Provider Network INTERNATIONAL PROVIDERS: HOSPITALS/CLINICS FacilitY Name CitY ADDRess Phone NUMBERS AFGHanistan DK-GERman MedicaL DiagnOstic STReet 66 / HOUse 138 / distRict 4 KABUL T: +93 (0) 799 13 62 10 CenteR ZOne1 ALBania T: +355 36 21 21 SURgicaL HOspitaL FOR ADULts TIRana F: +355 36 36 44 T: +355 36 21 21 HOspitaL OF InteRnaL Diseases TIRana F: +355 36 36 44 T: +355 36 21 21 PaediatRic HOspitaL TIRana F: +355 36 36 44 ALGERia 4 LOT. ALLIOULA FOdiL T: +213 (21) 36 28 28 CLiniQUE ChahRAZed ALgeR CHÉRaga F: +213 (21) 36 14 14 4 DJenane AchaBOU CLiniQUE AL AZhaR ALgeR -

Phenotypic Characterization of X-Linked Hypophosphatemia in Pediatric Spanish Population
Rodríguez‑Rubio et al. Orphanet J Rare Dis (2021) 16:154 https://doi.org/10.1186/s13023‑021‑01786‑5 CORRECTION Open Access Correction to: Phenotypic characterization of X‑linked hypophosphatemia in pediatric Spanish population Enrique Rodríguez‑Rubio1* , Helena Gil‑Peña2, Sara Chocron3, Leire Madariaga4, Francisco de la Cerda‑Ojeda5, Marta Fernández‑Fernández6, Carmen de Lucas‑Collantes7, Marta Gil8, María Isabel Luis‑Yanes9, Inés Vergara10, Juan David González‑Rodríguez11, Susana Ferrando12, Montserrat Antón‑Gamero13, Marta Carrasco Hidalgo‑Barquero14, Angustias Fernández‑Escribano15, Mº Ángeles Fernández‑Maseda16, Laura Espinosa17, Aniana Oliet18, Antonio Vicente19, Gema Ariceta3 and Fernando Santos1,2 on behalf of RenalTubeGroup Correction to: Orphanet J Rare Dis (2021) 16:104 Spain. 3 Servicio de Nefrología Pediátrica, Hospital Vall D’Hebron, Universitat 4 https://doi. org/ 10. 1186/ s13023- 021–01729-0 Autónoma de Barcelona, Barcelona, Spain. Servicio Nefrología Pediátrica, IIS Biocruces‑Bizkaia, Universidad del País Vasco UPV/EHU, Hospital Universitario Following the publication of the original article [1] the Cruces, Barakaldo, Spain. 5 Unidad de Nefrología Pediátrica, Hospital Virgen authors requested to update their funding declarations as del Rocío, Sevilla, Spain. 6 Servicio Pediatría, Complejo Asistencial Universi‑ tario de León, León, Spain. 7 Servicio Nefrología, Hospital Niño Jesús, Madrid, follows: Spain. 8 Servicio Pediatría, Hospital Universitario de Santiago de Compostela, Tis research has been partially funded by Kyowa Kirin Santiago de Compostela, Spain. 9 Servicio Pediatría, Hospital Universitario Farmacéutica S.L.U., project PI17/01745 from Insti- Nuestra Señora de Candelaria, Santa Cruz de Tenerife, Spain. 10 Servicio Pedi‑ atría, Complexo Hospitalario Universitario A Coruña (CHUAC), A Coruña, Spain. tuto de Salud Carlos III, Acción Estratégica en Salud 11 Unidad de Nefrología, Hospital General Universitario Santa Lucia, Cartagena, 2017–2020 and FEDER funds, Fondo de Investigaciones Spain.