Clean RCHC Report 2012 Template ENGLISH
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

An Analysis of the Afar-Somali Conflict in Ethiopia and Djibouti
Regional Dynamics of Inter-ethnic Conflicts in the Horn of Africa: An Analysis of the Afar-Somali Conflict in Ethiopia and Djibouti DISSERTATION ZUR ERLANGUNG DER GRADES DES DOKTORS DER PHILOSOPHIE DER UNIVERSTÄT HAMBURG VORGELEGT VON YASIN MOHAMMED YASIN from Assab, Ethiopia HAMBURG 2010 ii Regional Dynamics of Inter-ethnic Conflicts in the Horn of Africa: An Analysis of the Afar-Somali Conflict in Ethiopia and Djibouti by Yasin Mohammed Yasin Submitted in partial fulfilment of the requirements for the degree PHILOSOPHIAE DOCTOR (POLITICAL SCIENCE) in the FACULITY OF BUSINESS, ECONOMICS AND SOCIAL SCIENCES at the UNIVERSITY OF HAMBURG Supervisors Prof. Dr. Cord Jakobeit Prof. Dr. Rainer Tetzlaff HAMBURG 15 December 2010 iii Acknowledgments First and foremost, I would like to thank my doctoral fathers Prof. Dr. Cord Jakobeit and Prof. Dr. Rainer Tetzlaff for their critical comments and kindly encouragement that made it possible for me to complete this PhD project. Particularly, Prof. Jakobeit’s invaluable assistance whenever I needed and his academic follow-up enabled me to carry out the work successfully. I therefore ask Prof. Dr. Cord Jakobeit to accept my sincere thanks. I am also grateful to Prof. Dr. Klaus Mummenhoff and the association, Verein zur Förderung äthiopischer Schüler und Studenten e. V., Osnabruck , for the enthusiastic morale and financial support offered to me in my stay in Hamburg as well as during routine travels between Addis and Hamburg. I also owe much to Dr. Wolbert Smidt for his friendly and academic guidance throughout the research and writing of this dissertation. Special thanks are reserved to the Department of Social Sciences at the University of Hamburg and the German Institute for Global and Area Studies (GIGA) that provided me comfortable environment during my research work in Hamburg. -

Districts of Ethiopia
Region District or Woredas Zone Remarks Afar Region Argobba Special Woreda -- Independent district/woredas Afar Region Afambo Zone 1 (Awsi Rasu) Afar Region Asayita Zone 1 (Awsi Rasu) Afar Region Chifra Zone 1 (Awsi Rasu) Afar Region Dubti Zone 1 (Awsi Rasu) Afar Region Elidar Zone 1 (Awsi Rasu) Afar Region Kori Zone 1 (Awsi Rasu) Afar Region Mille Zone 1 (Awsi Rasu) Afar Region Abala Zone 2 (Kilbet Rasu) Afar Region Afdera Zone 2 (Kilbet Rasu) Afar Region Berhale Zone 2 (Kilbet Rasu) Afar Region Dallol Zone 2 (Kilbet Rasu) Afar Region Erebti Zone 2 (Kilbet Rasu) Afar Region Koneba Zone 2 (Kilbet Rasu) Afar Region Megale Zone 2 (Kilbet Rasu) Afar Region Amibara Zone 3 (Gabi Rasu) Afar Region Awash Fentale Zone 3 (Gabi Rasu) Afar Region Bure Mudaytu Zone 3 (Gabi Rasu) Afar Region Dulecha Zone 3 (Gabi Rasu) Afar Region Gewane Zone 3 (Gabi Rasu) Afar Region Aura Zone 4 (Fantena Rasu) Afar Region Ewa Zone 4 (Fantena Rasu) Afar Region Gulina Zone 4 (Fantena Rasu) Afar Region Teru Zone 4 (Fantena Rasu) Afar Region Yalo Zone 4 (Fantena Rasu) Afar Region Dalifage (formerly known as Artuma) Zone 5 (Hari Rasu) Afar Region Dewe Zone 5 (Hari Rasu) Afar Region Hadele Ele (formerly known as Fursi) Zone 5 (Hari Rasu) Afar Region Simurobi Gele'alo Zone 5 (Hari Rasu) Afar Region Telalak Zone 5 (Hari Rasu) Amhara Region Achefer -- Defunct district/woredas Amhara Region Angolalla Terana Asagirt -- Defunct district/woredas Amhara Region Artuma Fursina Jile -- Defunct district/woredas Amhara Region Banja -- Defunct district/woredas Amhara Region Belessa -- -

Ethiopia: 2015 HRF Projects Map (As of 31 December 2015)
Ethiopia: 2015 HRF projects map (as of 31 December 2015) Countrywide intervention ERITREA Legend UNICEF - Nutrition - $999,753 Concern☃ - VSF-G ☈ ! Refugee camp WFP - Nutrition (CSB) - $1.5m National capital Shimelba Red Sea SUDAN Regional intervention International boundary Hitsa!ts Dalul UNICEF - Health - $1.0m ! !Hitsats ! ! Undetermined boundary ! ! SCI Tigray, Afar, Amhara, Oromia, Kelete Berahile ☃☉ May-Ayni Kola ! Somali, Gambella, SNPR & NRC - ☉ Ts!elemti Temben Awelallo Lake IRC - ★ ! ☄ ! ♫ Tanqua ! SUDAN ! ! ! Dire Dawa Adi Harush ! Enderta Abergele ! Ab Ala Afdera Project woredas Tselemt ! NRC - Debark GAA - ☇ ! WFP (UNHAS) - Coordination ☈ Abergele! Erebti ☋☉ Plan Int. - ACF - ☃ Dabat Sahla ☃Megale Bidu and Support Service - $740,703 Janamora Wegera! Clusters/Activities ! Ziquala Somali region Sekota ! ! Concern - SCI Teru ! Agriculture CRS - Agriculture/Seed - $2,5m ☃ ☃ Kurri ! Dehana ! ☋ ! Gaz Alamata ! Elidar GAA - ☋ Amhara,Ormia and SNNP regions ! ☃☉ Gonder Zuria Gibla ! Gulf of ! Education Plan Int. - Ebenat Kobo SCI☃☉ ☃ ! Gidan ☄ Lasta ! Aden CARE - Lay Guba ! Ewa ! ☃ ! Meket Lafto Gayint ! Food security & livelihood WV - ☃ Dubti ☈ ☉ ! Tach Habru Chifra SCI - ☃ Delanta ! ! - Tigray Region, Eastern Zone, Kelete Awelall, ! Gayint IMC - ☃ Health ☉ Simada Southern Zone, Alamata and Enderta woredas ! ! Mile DJIBOUTI ☊ Mekdela ! Bati Enbise SCI- Nutrition ! Argoba ☃☉ WV - ☃ Sar Midir Legambo ☃ ! Oxfam GB - Enarj ! ☉ ! ! Ayisha Non Food Items - Amhara region, North Gonder (Gonder Zuria), Enawga ! Antsokiya Dalfagi ! ! ! Concern -

COUNTRY Food Security Update
ETHIOPIA Food Security Outlook Update September 2013 Crops are at their normal developmental stages in most parts of the country Figure 1. Projected food security outcomes, KEY MESSAGES September 2013 • Following the mostly normal performance of the June to September Kiremt rains, most crops are at their normally expected developmental stage. A near normal Meher harvest is expected in most parts of the country. However, in places where Kiremt rains started late and in areas where some weather-related hazards occurred, some below normal production is anticipated. • Market prices of most staple cereals remain stable at their elevated levels compared to previous months, but prices are likely to fall slightly starting in October due to the expected near normal Meher production in most parts of the country, which, in turn, will also improve household-level food access from October to December. Source: FEWS NET Ethiopia • Overall, current nutritional status compared to June/July has slightly improved or remains the same with exceptions in Figure 2. Projected food security outcomes, some areas in northeastern Tigray and Amhara Regions as October to December 2013 well as some parts of East Hararghe Zone in Oromia Region. In these areas, there are indications of deteriorating nutritional status due to the well below average Belg harvest and the current absence of a green harvest from long-cycle Meher crops. CURRENT SITUATION • Cumulative Kiremt rainfall from June to September was normal to above normal and evenly distributed in all of Southern Nations, Nationalities, and Peoples’ Region (SNNPR), in most parts of Amhara, in central and western parts Oromia, and in the central parts of Tigray. -
20210714 Access Snapshot- Tigray Region June 2021 V2
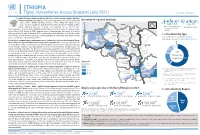
ETHIOPIA Tigray: Humanitarian Access Snapshot (July 2021) As of 31 July 2021 The conflict in Tigray continues despite the unilateral ceasefire announced by the Ethiopian Federal Government on 28 June, which resulted in the withdrawal of the Ethiopian National Overview of reported incidents July Since Nov July Since Nov Defense Forces (ENDF) and Eritrea’s Defense Forces (ErDF) from Tigray. In July, Tigray forces (TF) engaged in a military offensive in boundary areas of Amhara and Afar ERITREA 13 153 2 14 regions, displacing thousands of people and impacting access into the area. #Incidents impacting Aid workers killed Federal authorities announced the mobilization of armed forces from other regions. The Amhara region the security of aid Tahtay North workers Special Forces (ASF), backed by ENDF, maintain control of Western zone, with reports of a military Adiyabo Setit Humera Western build-up on both sides of the Tekezi river. ErDF are reportedly positioned in border areas of Eritrea and in SUDAN Kafta Humera Indasilassie % of incidents by type some kebeles in North-Western and Eastern zones. Thousands of people have been displaced from town Central Eastern these areas into Shire city, North-Western zone. In line with the Access Monitoring and Western Korarit https://bit.ly/3vcab7e May Reporting Framework: Electricity, telecommunications, and banking services continue to be disconnected throughout Tigray, Gaba Wukro Welkait TIGRAY 2% while commercial cargo and flights into the region remain suspended. This is having a major impact on Tselemti Abi Adi town May Tsebri relief operations. Partners are having to scale down operations and reduce movements due to the lack Dansha town town Mekelle AFAR 4% of fuel. -
Report on Evaluation of W SH
Report on Evaluation of WASH - Joint Action Plan (JAP) implementation in eight water insecure Woredas in Afar Regional state Submitted to UNICEF – Ethiopia WASH Section/Afar Field office Prepared by Tesfa Aklilu WASH - Consultant (CIPM, BSc, MPH, MSc (pending, AAU) November 13, 2015 Afar – Semera - Ethiopia | P a g e Table of contents Table of figures .............................................................................................................................................. i Tables ............................................................................................................................................................. i Acronyms ...................................................................................................................................................... ii WASHCOs: Water, Sanitation and Hygiene Committees ........................................................... ii Acknowledgement ........................................................................................................................................ ii Executive Summary ................................................................................................................................ iii 1. Introduction ........................................................................................................................................... 1 2. Objectives of Evaluation ............................................................................................................... 2 2.1. General -

Protecting Land Tenure Security of Women in Ethiopia: Evidence from the Land Investment for Transformation Program
PROTECTING LAND TENURE SECURITY OF WOMEN IN ETHIOPIA: EVIDENCE FROM THE LAND INVESTMENT FOR TRANSFORMATION PROGRAM Workwoha Mekonen, Ziade Hailu, John Leckie, and Gladys Savolainen Land Investment for Transformation Programme (LIFT) (DAI Global) This research paper was created with funding and technical support of the Research Consortium on Women’s Land Rights, an initiative of Resource Equity. The Research Consortium on Women’s Land Rights is a community of learning and practice that works to increase the quantity and strengthen the quality of research on interventions to advance women’s land and resource rights. Among other things, the Consortium commissions new research that promotes innovations in practice and addresses gaps in evidence on what works to improve women’s land rights. Learn more about the Research Consortium on Women’s Land Rights by visiting https://consortium.resourceequity.org/ This paper assesses the effectiveness of a specific land tenure intervention to improve the lives of women, by asking new questions of available project data sets. ABSTRACT The purpose of this research is to investigate threats to women’s land rights and explore the effectiveness of land certification interventions using evidence from the Land Investment for Transformation (LIFT) program in Ethiopia. More specifically, the study aims to provide evidence on the extent that LIFT contributed to women’s tenure security. The research used a mixed method approach that integrated quantitative and qualitative data. Quantitative information was analyzed from the profiles of more than seven million parcels to understand how the program had incorporated gender interests into the Second Level Land Certification (SLLC) process. -

Hum Ethio Manitar Opia Rian Re Espons E Fund D
Hum anitarian Response Fund Ethiopia OCHA, 2011 OCHA, 2011 Annual Report 2011 Office for the Coordination of Humanitarian Affairs Humanitarian Response Fund – Ethiopia Annual Report 2011 Table of Contents Note from the Humanitarian Coordinator ................................................................................................ 2 Acknowledgements ................................................................................................................................. 3 1. Executive Summary ............................................................................................................................ 4 1.1 2011 Humanitarian Context ........................................................................................................... 4 1.2 Map - 2011 HRF Supported Projects ............................................................................................. 6 2. Information on Contributors ................................................................................................................ 7 2.1 Donor Contributions to HRF .......................................................................................................... 7 3. Fund Overview .................................................................................................................................... 8 3.1 Summary of HRF Allocations in 2011 ............................................................................................ 8 3.1.1 HRF Allocation by Sector ....................................................................................................... -

PDF Download
Integrated Blood Pressure Control Dovepress open access to scientific and medical research Open Access Full Text Article ORIGINAL RESEARCH Knowledge and Attitude of Self-Monitoring of Blood Pressure Among Adult Hypertensive Patients on Follow-Up at Selected Public Hospitals in Arsi Zone, Oromia Regional State, Ethiopia: A Cross-Sectional Study This article was published in the following Dove Press journal: Integrated Blood Pressure Control Addisu Dabi Wake 1 Background: Self-monitoring of blood pressure (BP) among hypertensive patients is an Daniel Mengistu Bekele 2 important aspect of the management and prevention of complication related to hypertension. Techane Sisay Tuji 1 However, self-monitoring of BP among hypertensive patients on scheduled follow-up in hospitals in Ethiopia is unknown. The aim of the study was to assess knowledge and attitude 1Nursing Department, College of Medical and Health Sciences, Arsi University, of self-monitoring of BP among adult hypertensive patients. Asella, Ethiopia; 2School of Nursing and Methods: A cross-sectional survey was conducted on 400 adult hypertensive patients attend- Midwifery, College of Health Sciences, ing follow-up clinics at four public hospitals of Arsi Zone, Oromia Regional State, Ethiopia. Addis Ababa University, Addis Ababa, Ethiopia The data were collected from patients from March 10, 2019 to April 8, 2019 by face-to-face interview using a pretested questionnaire and augmented by a retrospective patients’ medical records review. The data were analyzed using the SPSS version 21.0 software. Results: A total of 400 patients were enrolled into the study with the response rate of 97.6%. The median age of the participants was 49 years (range 23–90 years). -

ETHIOPIA - National Hot Spot Map 31 May 2010
ETHIOPIA - National Hot Spot Map 31 May 2010 R Legend Eritrea E Tigray R egion !ª D 450 ho uses burned do wn d ue to th e re ce nt International Boundary !ª !ª Ahferom Sudan Tahtay Erob fire incid ent in Keft a hum era woreda. I nhabitan ts Laelay Ahferom !ª Regional Boundary > Mereb Leke " !ª S are repo rted to be lef t out o f sh elter; UNI CEF !ª Adiyabo Adiyabo Gulomekeda W W W 7 Dalul E !Ò Laelay togethe r w ith the regiona l g ove rnm ent is Zonal Boundary North Western A Kafta Humera Maychew Eastern !ª sup portin g the victim s with provision o f wate r Measle Cas es Woreda Boundary Central and oth er imm ediate n eeds Measles co ntinues to b e re ported > Western Berahle with new four cases in Arada Zone 2 Lakes WBN BN Tsel emt !A !ª A! Sub-city,Ad dis Ababa ; and one Addi Arekay> W b Afa r Region N b Afdera Military Operation BeyedaB Ab Ala ! case in Ahfe rom woreda, Tig ray > > bb The re a re d isplaced pe ople from fo ur A Debark > > b o N W b B N Abergele Erebtoi B N W Southern keb eles of Mille and also five kebeles B N Janam ora Moegale Bidu Dabat Wag HiomraW B of Da llol woreda s (400 0 persons) a ff ected Hot Spot Areas AWD C ases N N N > N > B B W Sahl a B W > B N W Raya A zebo due to flo oding from Awash rive r an d ru n Since t he beg in nin g of th e year, Wegera B N No Data/No Humanitarian Concern > Ziquala Sekota B a total of 967 cases of AWD w ith East bb BN > Teru > off fro m Tigray highlands, respective ly. -

73-84 Association of Arabica Coffee Quality Attributes with Selected So
East African Journal of Sciences (2015) Volume 9 (2) 73-84 Association of Arabica Coffee Quality Attributes with Selected Soil Chemical Properties Adugnaw Mintesnot1*, Nigussie Dechassa2,and Ali Mohammed1 1Jimma University, Department of Horticulture, P. O. Box 307, Jimma, Ethiopia 2Haramaya University, Department of Plant Sciences, P. O. Box 138, Dire Dawa, Ethiopia Abstract: Coffee (Coffea arabica L.) bean quality attributes differ based on the origin of the produce. Several agro-ecological conditions influence coffee bean quality attributes. Soil chemical properties may be some of the factors affecting the quality attributes. However, no study has so far been conducted to elucidate the association of coffee bean qualities with soil chemical properties in both major and minor coffee growing regions of Ethiopia. Thus, this research was conducted with the objective of establishing association of chemical soil properties with coffee cup quality attributes. Coffee beans as well as soil samples from which the beans originated were subjected to chemical analysis. The coffee beans and the corresponding soil samples originated from large scale coffee plantations (Bebeka, Gemadro and Goma), districts from southwestern major coffee growing region (Gore, Jimma, Lemkefa), West (Gimbi), East (Badano, Chiro, Darolebu, Habro and Melkabelo), South (Yirgacheffe) and northwestern minor coffee growing districts (Ankasha, Bure, Mecha and Jabi). The soil samples were collected from the depth of 0 - 50 cm near the coffee trunks and samples of ripe coffee cherries were picked up from the trees during the 2010/11 harvest season. Selected chemical properties of the soil, namely, available potassium, cation exchange capacity, exchangeable acidity, exchangeable bases, available micronutrients, available phosphorus, total nitrogen, soil pH, electrical conductivity, and percent organic carbon were determined from 53 soil samples in Jimma University soil laboratory and Wolkitie Soil Testing and Soil Fertility Improvement Centre using the established procedures. -

Floristic Composition and Carbon Pools Along Altitudinal Gradient: the Case of Gara–Muktar Forest, West Hararghe Zone, Eastern Ethiopia
Forestry Research and Engineering: International Journal Research Article Open Access Floristic composition and carbon pools along altitudinal gradient: the case of gara–muktar forest, west hararghe zone, eastern Ethiopia Abstract Volume 4 Issue 1 - 2020 Forests play vital role in combating climate change through carbon sequestration in the Asaminew Wodajo,1 Mehari A Tesfaye,2 atmosphere and serving as a carbon sink in the form of carbon pool systems of forest 3 ecosystems. The species composition and carbon stock in the different carbon pools Muktar Mohammed 1Bonga Agricultural Research Centre, Ethiopia, and analysis of the influence of the environmental gradients were studied by systematic 2Central Ethiopia Environment and Forest Research, Ethiopia sampling method collecting data in thirty-six quadrant plots of 20x20m each distributed 3Oda Bultum Universities, Ethiopia along transect lines. Diameter at breast ≥5cm and total height measured for each tree in the main plot. Above and below ground biomass was estimated using allometric equation, Correspondence: Mehari Alebachew Tesfaye, Central Ethiopia while the litter carbon was estimated by taking 50% of dry biomass as carbon. Soil sample Environment and Forest Research Centre box 30708, Addis was collected using auguring method and analyzed following Walkley-Black method, Ababa, Ethiopia, Tele +251911356756, while bulk density was performed using core sampling method. The data was analyzed Email was performed using one way ANOVA of R software. The carbon stocks in aboveground, belowground, litter biomass and soil organic carbon showed distinct variation along Received: November 27, 2020 | Published: February 28, 2020 environmental gradients. The aboveground and below ground carbon stock was showed a decreasing trend along with increasing altitude, while soil organic carbon and liter carbon showed increasing trend along with increasing in altitude.