The Effect of Community-Based Interventions on Increasing Family
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

An Analysis of the Afar-Somali Conflict in Ethiopia and Djibouti
Regional Dynamics of Inter-ethnic Conflicts in the Horn of Africa: An Analysis of the Afar-Somali Conflict in Ethiopia and Djibouti DISSERTATION ZUR ERLANGUNG DER GRADES DES DOKTORS DER PHILOSOPHIE DER UNIVERSTÄT HAMBURG VORGELEGT VON YASIN MOHAMMED YASIN from Assab, Ethiopia HAMBURG 2010 ii Regional Dynamics of Inter-ethnic Conflicts in the Horn of Africa: An Analysis of the Afar-Somali Conflict in Ethiopia and Djibouti by Yasin Mohammed Yasin Submitted in partial fulfilment of the requirements for the degree PHILOSOPHIAE DOCTOR (POLITICAL SCIENCE) in the FACULITY OF BUSINESS, ECONOMICS AND SOCIAL SCIENCES at the UNIVERSITY OF HAMBURG Supervisors Prof. Dr. Cord Jakobeit Prof. Dr. Rainer Tetzlaff HAMBURG 15 December 2010 iii Acknowledgments First and foremost, I would like to thank my doctoral fathers Prof. Dr. Cord Jakobeit and Prof. Dr. Rainer Tetzlaff for their critical comments and kindly encouragement that made it possible for me to complete this PhD project. Particularly, Prof. Jakobeit’s invaluable assistance whenever I needed and his academic follow-up enabled me to carry out the work successfully. I therefore ask Prof. Dr. Cord Jakobeit to accept my sincere thanks. I am also grateful to Prof. Dr. Klaus Mummenhoff and the association, Verein zur Förderung äthiopischer Schüler und Studenten e. V., Osnabruck , for the enthusiastic morale and financial support offered to me in my stay in Hamburg as well as during routine travels between Addis and Hamburg. I also owe much to Dr. Wolbert Smidt for his friendly and academic guidance throughout the research and writing of this dissertation. Special thanks are reserved to the Department of Social Sciences at the University of Hamburg and the German Institute for Global and Area Studies (GIGA) that provided me comfortable environment during my research work in Hamburg. -

Districts of Ethiopia
Region District or Woredas Zone Remarks Afar Region Argobba Special Woreda -- Independent district/woredas Afar Region Afambo Zone 1 (Awsi Rasu) Afar Region Asayita Zone 1 (Awsi Rasu) Afar Region Chifra Zone 1 (Awsi Rasu) Afar Region Dubti Zone 1 (Awsi Rasu) Afar Region Elidar Zone 1 (Awsi Rasu) Afar Region Kori Zone 1 (Awsi Rasu) Afar Region Mille Zone 1 (Awsi Rasu) Afar Region Abala Zone 2 (Kilbet Rasu) Afar Region Afdera Zone 2 (Kilbet Rasu) Afar Region Berhale Zone 2 (Kilbet Rasu) Afar Region Dallol Zone 2 (Kilbet Rasu) Afar Region Erebti Zone 2 (Kilbet Rasu) Afar Region Koneba Zone 2 (Kilbet Rasu) Afar Region Megale Zone 2 (Kilbet Rasu) Afar Region Amibara Zone 3 (Gabi Rasu) Afar Region Awash Fentale Zone 3 (Gabi Rasu) Afar Region Bure Mudaytu Zone 3 (Gabi Rasu) Afar Region Dulecha Zone 3 (Gabi Rasu) Afar Region Gewane Zone 3 (Gabi Rasu) Afar Region Aura Zone 4 (Fantena Rasu) Afar Region Ewa Zone 4 (Fantena Rasu) Afar Region Gulina Zone 4 (Fantena Rasu) Afar Region Teru Zone 4 (Fantena Rasu) Afar Region Yalo Zone 4 (Fantena Rasu) Afar Region Dalifage (formerly known as Artuma) Zone 5 (Hari Rasu) Afar Region Dewe Zone 5 (Hari Rasu) Afar Region Hadele Ele (formerly known as Fursi) Zone 5 (Hari Rasu) Afar Region Simurobi Gele'alo Zone 5 (Hari Rasu) Afar Region Telalak Zone 5 (Hari Rasu) Amhara Region Achefer -- Defunct district/woredas Amhara Region Angolalla Terana Asagirt -- Defunct district/woredas Amhara Region Artuma Fursina Jile -- Defunct district/woredas Amhara Region Banja -- Defunct district/woredas Amhara Region Belessa -- -
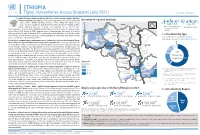
20210714 Access Snapshot- Tigray Region June 2021 V2
ETHIOPIA Tigray: Humanitarian Access Snapshot (July 2021) As of 31 July 2021 The conflict in Tigray continues despite the unilateral ceasefire announced by the Ethiopian Federal Government on 28 June, which resulted in the withdrawal of the Ethiopian National Overview of reported incidents July Since Nov July Since Nov Defense Forces (ENDF) and Eritrea’s Defense Forces (ErDF) from Tigray. In July, Tigray forces (TF) engaged in a military offensive in boundary areas of Amhara and Afar ERITREA 13 153 2 14 regions, displacing thousands of people and impacting access into the area. #Incidents impacting Aid workers killed Federal authorities announced the mobilization of armed forces from other regions. The Amhara region the security of aid Tahtay North workers Special Forces (ASF), backed by ENDF, maintain control of Western zone, with reports of a military Adiyabo Setit Humera Western build-up on both sides of the Tekezi river. ErDF are reportedly positioned in border areas of Eritrea and in SUDAN Kafta Humera Indasilassie % of incidents by type some kebeles in North-Western and Eastern zones. Thousands of people have been displaced from town Central Eastern these areas into Shire city, North-Western zone. In line with the Access Monitoring and Western Korarit https://bit.ly/3vcab7e May Reporting Framework: Electricity, telecommunications, and banking services continue to be disconnected throughout Tigray, Gaba Wukro Welkait TIGRAY 2% while commercial cargo and flights into the region remain suspended. This is having a major impact on Tselemti Abi Adi town May Tsebri relief operations. Partners are having to scale down operations and reduce movements due to the lack Dansha town town Mekelle AFAR 4% of fuel. -
Report on Evaluation of W SH
Report on Evaluation of WASH - Joint Action Plan (JAP) implementation in eight water insecure Woredas in Afar Regional state Submitted to UNICEF – Ethiopia WASH Section/Afar Field office Prepared by Tesfa Aklilu WASH - Consultant (CIPM, BSc, MPH, MSc (pending, AAU) November 13, 2015 Afar – Semera - Ethiopia | P a g e Table of contents Table of figures .............................................................................................................................................. i Tables ............................................................................................................................................................. i Acronyms ...................................................................................................................................................... ii WASHCOs: Water, Sanitation and Hygiene Committees ........................................................... ii Acknowledgement ........................................................................................................................................ ii Executive Summary ................................................................................................................................ iii 1. Introduction ........................................................................................................................................... 1 2. Objectives of Evaluation ............................................................................................................... 2 2.1. General -

Hum Ethio Manitar Opia Rian Re Espons E Fund D
Hum anitarian Response Fund Ethiopia OCHA, 2011 OCHA, 2011 Annual Report 2011 Office for the Coordination of Humanitarian Affairs Humanitarian Response Fund – Ethiopia Annual Report 2011 Table of Contents Note from the Humanitarian Coordinator ................................................................................................ 2 Acknowledgements ................................................................................................................................. 3 1. Executive Summary ............................................................................................................................ 4 1.1 2011 Humanitarian Context ........................................................................................................... 4 1.2 Map - 2011 HRF Supported Projects ............................................................................................. 6 2. Information on Contributors ................................................................................................................ 7 2.1 Donor Contributions to HRF .......................................................................................................... 7 3. Fund Overview .................................................................................................................................... 8 3.1 Summary of HRF Allocations in 2011 ............................................................................................ 8 3.1.1 HRF Allocation by Sector ....................................................................................................... -
Examining Alternative Livelihoods for Improved Resilience and Transformation in Afar
EXAMINING ALTERNATIVE LIVELIHOODS FOR IMPROVED RESILIENCE AND TRANSFORMATION IN AFAR May 2019 Report photos: Dr. Daniel Temesgen EXAMINING ALTERNATIVE LIVELIHOODS FOR IMPROVED RESILIENCE AND TRANSFORMATION IN AFAR May 2019 This document has been produced with the financial assistance of the European Union. The views expressed herein can in no way be taken to reflect the official opinion of the European Union. Report authors: Daniel Temesga, Amdissa Teshome, Berhanu Admassu Suggested citation: FAO and Tufts University. (2019). Examining Alternative Livelihoods for Improved Resilience and Transformation in Afar. FAO: Addis Ababa, Ethiopia. Implemented by: Feinstein International Center Friedman School of Nutrition Science and Policy Tufts University Africa Regional Office www.fic.tufts.edu © FAO TABLE OF CONTENTS EXECUTIVE SUMMARY ............................................................................................................................... 6 I. BACKGROUND............................................................................................................................................ 8 The Afar Region: context and livelihoods ................................................................................................... 8 The purpose of the study ............................................................................................................................ 8 The study’s approaches and methods ......................................................................................................... -

COUNTRY Food Security Update
ETHIOPIA Food Security Outlook Update June 2013 The delayed Belg harvest prolongs lean season in southern and eastern Belg-producing areas Figure 1. Current food security outcomes, June 2013 KEY MESSAGES • Following a three- to four-week delayed onset of the rains which delayed planting and crop development, Belg crops will likely not be harvested until mid-July in southern and eastern Belg-producing areas instead of mid-June. The delayed harvest prevents the timely planting of short-cycle Meher crops on the same land. • The poor performance of February to May Belg rains in the northeastern receiving areas is likely to result in a well below average and delayed Belg harvest, increasing food insecurity from July to September. In parts of the southern areas, food security will improve from Crisis (IPC Phase 3) in some areas to Stressed (IPC Phase 2) with increased supply from the Belg harvest, even if that harvest is both late and somewhat below average. Source: FEWS NET Ethiopia • The good performance of March to May Gu/Genna rains Figure 2. Projected food security outcomes, July to increased milk production, so the food security situation September 2013 in southern and southeastern pastoral areas has improved. The declines in milk prices have increased milk access for market-dependent households as well. • Above average rainfall totals since mid-May have enabled the planting of long-cycle maize and sorghum and land preparation for short-cycle crops in most parts of the country except in the northeastern areas where the total Belg rainfall was below average. With normal to above normal June to September Kiremt rains forecast, the Meher crop performance is likely to be normal in these areas. -

Afar: Insecurity and Delayed Rains Threaten Livestock and People
EMERGENCIES UNIT FOR UNITED NATIONS ETHIOPIA (UN-EUE) Afar: insecurity and delayed rains threaten livestock and people Assessment Mission: 29 May – 8 June 2002 François Piguet, Field Officer, UN-Emergencies Unit for Ethiopia 1 Introduction and background 1.1 Animals are now dying The Objectives of the mission were to assess the situation in the Afar Region following recent clashes between Afar and Issa and Oromo pastoralists, and focus on security and livestock movement restrictions, wate r and environmental issues, the marketing of livestock as well as “chronic” humanitarian issues. Special attention has been given to all southern parts of Afar region affected by recent ethnic conflicts and erratic small rains, which initiated early pastoralists movements in zone 3 & 5. The assessment also took into account various food security issues, including milk availability while also looking at limited water resources in Eli Daar woreda (Zone 1), where particularly remote kebeles1 suffer from water shortage. High concentrations of animals have been noticed in several locations of Afar region during the current dry season. The most important reason for the present humanitarian emergency crisis in parts of Afar Region and surroundings are the various ethnic conflicts among the Issa, the Kereyu, the Afar and the Ittu. These Dead camel in Doho, Awash-Fantale (photo Francois Piguet conflicts forced pastoralists to change UN-EUE, July 2002 their usual migration patterns and most importantly were denied access to either traditional water points and wells or grazing areas or both together. On top of this rather complex and confuse conflict situation, rains have now been delayed by more than two weeks most likely all over Afar Region and is now causing livestock deaths. -

Ethiopia COI Compilation
BEREICH | EVENTL. ABTEILUNG | WWW.ROTESKREUZ.AT ACCORD - Austrian Centre for Country of Origin & Asylum Research and Documentation Ethiopia: COI Compilation November 2019 This report serves the specific purpose of collating legally relevant information on conditions in countries of origin pertinent to the assessment of claims for asylum. It is not intended to be a general report on human rights conditions. The report is prepared within a specified time frame on the basis of publicly available documents as well as information provided by experts. All sources are cited and fully referenced. This report is not, and does not purport to be, either exhaustive with regard to conditions in the country surveyed, or conclusive as to the merits of any particular claim to refugee status or asylum. Every effort has been made to compile information from reliable sources; users should refer to the full text of documents cited and assess the credibility, relevance and timeliness of source material with reference to the specific research concerns arising from individual applications. © Austrian Red Cross/ACCORD An electronic version of this report is available on www.ecoi.net. Austrian Red Cross/ACCORD Wiedner Hauptstraße 32 A- 1040 Vienna, Austria Phone: +43 1 58 900 – 582 E-Mail: [email protected] Web: http://www.redcross.at/accord This report was commissioned by the United Nations High Commissioner for Refugees (UNHCR), Division of International Protection. UNHCR is not responsible for, nor does it endorse, its content. TABLE OF CONTENTS List of abbreviations ........................................................................................................................ 4 1 Background information ......................................................................................................... 6 1.1 Geographical information .................................................................................................... 6 1.1.1 Map of Ethiopia ........................................................................................................... -

Sero-Prevalence of Contagious Caprine Pleuropneu- Monia in Goat at Selected Woredas of Afar Region
Sero-Prevalence of Contagious Caprine Pleuropneu- monia in Goat at Selected Woredas of Afar Region Feyesa Regassa1* Misrak Netsere1, Tefera Tsertse2, 1 Jimma University, College of Agriculture and Veterinary Medicine, School of Veteri- nary Medicine, P. O. Box 307, Jimma, Ethiopia * Corresponding author: [email protected] 2 National Animal Health diagnostic and Investigation Center Abstract A cross - sectional survey was conducted from 17 Oct. to 11 Dec. 2008 with the aim of determining the sero-prevalence and the major risk factors of contagious caprine pleuropneumonia (CCPP) in the selected eight districts of Afar region namely: Afambo, Assaita, Dubti, Mille, Gewane, Amibara, Dewe and Telalak. During the study a total of 329 goat sera, was examined for the presence of specific antibod- ies against Mycoplasma capricolum sub. spp. capripneumoniae using CFT. The result revealed that 22.49% (74) prevalence rate. With respect to goats origin, the serological prevalence rates was 31.85%, 36.36%, 18.75%, 12.50%, 12.16%, 10%, 22.22%, and 19.56% from Afambo, Assaita, Dubti, Mille, Gewane, Amibara, Dewe and Telalak districts respectively. The result indicated that there is significant dif- ference (P < 0.05) in sero positive rate among the different districts. The considered risk factors, age (P<0.05, χ2=7.8792) and sex (P<0.05, χ2=5.9661) were found to be significantly associated with the prevalence of CCPP in the study population. In conclusion the present study indicated that the over all prevalence of CCPP in Afar region is high. The study underlines the importance of further epidemiologi- cal study of the disease and its associated risk factors, and implementation of ap- propriate preventive and control measures. -

Ethiopia: Humanitarian Access Situation Report
ETHIOPIA Humanitarian Access Situation Report January - March 2020 This report is produced by OCHA Ethiopia in collaboration with humanitarian partners. It covers the period January to March 2020. The next report will be issued in June 2020. OVERVIEW • The operational environment to relief operations North Number of incidents by woreda Western Central remained permissive through the reporting period. Western TIGRAY Eastern 1 - 2 3 - 4 5 - 6 South Kilbet Most access impediments continue related to hos- North Rasu Gondar Eastern Wag tilities, intra-community conflicts or social unrest, Central Southern Gondar Hamra West Fantana hindering the quality of the humanitarian response, Gondar AMHARA North Wello Rasu AFAR and to COVID-19. South Awsi Gondar Rasu Metekel Hari Awi West East South Wello Gojam Rasu • Humanitarian partners are committed to support BENISHANGUL Gojam Oromia GUMUZ Siti the government response to COVID-19 and ensure North North Gabi Kemashi Horo Shewa DIRE DAWA West Shewa Rasu that critical activities are sustained. Partners are Gudru West Mao Komo Wellega Wellega Shewa Fafan Special East Addis Ababa actively implementing precautionary measures to Wellega HARARI Kelem Wellega East South West West ensure the safety of aid personnel and the popula- Buno Bedele East Hararge Hararge Ilu Aba Shewa Shewa Guraghe GAMBELA Bora Jarar tion. Nuwer Arsi Erer Agnewak Jimma Hadiya Siltie Sheka Yem Sp.Halaba Sp. OROMIA Kembata Mejenger Kefa Doolo Dawuro Tibaro Nogob SOMALI • The humanitarian community is working with gov- Bench Maji West Arsi Konta Sp. Wolayita Bale Gofa Sidama ernment counterparts to ensure that partners can Gamo Korahe Mirab Basketo Gedeo continue movements and operations throughout Omo Amaro SNNP Derashe Alle Guji Shabelle the country, bearing in mind restrictions to contain South Omo BurjiWest Guji Konso Afder the spread of COVID-19. -

WEEKLY HUMANITARIAN HIGHLIGHTS in ETHIOPIA 16 September 2013
WEEKLY HUMANITARIAN HIGHLIGHTS IN ETHIOPIA 16 September 2013 Health Update The Ethiopian government, in collaboration with partners, continues to strengthen community based surveillance and to implement polio supplementary immunization activities following the polio outbreak in neighbouring Somalia and in Dadaab refugee camp and the host district in Kenya in May. In Ethiopia, one confirmed case of wild polio virus type 1 was reported from Injiro kebele in Geladi woreda of Doolo zone, Somali region on 10 July. As of 2 September, an initial emergency immunization campaign targeting 184,611 children below the age of 15 years in the Dollo Ado refugee camps and the host community; two rounds of immunization campaigns targeting 2,664,894 children under-5 in Somali region, Harari region, the city of Dire Dawa, as well as selected high-risk zones in Oromia and SNNP regions; and a third round of immunization campaign targeting 947,480 children under-5 in Somali region were completed. A fourth round targeting 1,096,358 children under-5 is planned for 27 to 30 September in Somali region. Meanwhile, mapping of cross border and transit points was done and eight permanent vaccination posts were established at cross border points. The posts are providing polio vaccines to all children under 15 years crossing the border to and from Somalia. The Government and partners aim to establish a total of 16 vaccination posts at border points with Somalia. In an effort to mobilize more resources, WHO and UNICEF are jointly developing a proposal for CERF application. In addition to financial resources, partners are requested to provide logistical support to strengthen the current polio response activities.