Addressing Intimate Partner Violence in South Asia
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Death of Freedom Fighter Chittaranjan Das: This Day in History – Jun 16
Death of Freedom Fighter Chittaranjan Das: This Day in History – Jun 16 Chittaranjan Das, also known as C.R. Das, freedom fighter and eminent lawyer passed away on 16 June 1925 Darjeeling. This article will give details about his life and legacy within the context of the Indian History Segment of the IAS Exams. Biography of Chittranjan Das ● Chittaranjan Das was born on 5 Novem-ber 1870 at Telibagh in the Bengal Presidency, currently in Bangladesh. ● He was the son of Bhuban Mohan Das, a lawyer, and his wife, Nistarini Debi. His family members were actively involved in Raja Ram Mohan Roy’s Brahmo Samaj. Dad's uncle, Durga Mohan Das was a prominent Brahmo social reformer and worked in the fields of widow remarriage and women’s liberation. ● In 1890, Das completed his graduation from Calcutta’s Presidency College and then went to England to pursue higher studies and take the Indian Civil Services exam. He, however, did not clear the ICS. ● He finished his law studies from England and returned to India in 1893. ● He practised law for many years at the Calcutta High Court. ● In the 1908 Alipore Bomb Case, Das defended Aurobindo Ghosh and gained fame among Indians. ● He also contributed to the English weekly ‘Bande Mataram’ along with Aurobindo and Bipin Chandra Pal (Born on November 7th, 1858) ● He actively advocated the use of the Bengali language in university examinations. ● He championed the cause of Khadi and cottage industries and gave up his own western clothes and luxurious lifestyle. ● He became involved with the Non-Cooperation Movement led by Mahatma Gandhi. -
15 Kanika Singh Format
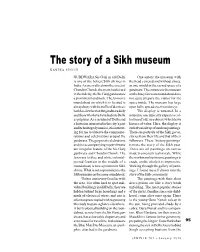
The story of a Sikh museum KANIKA SINGH GURDWARA Sis Ganj in old Delhi One enters the museum with is one of the holiest Sikh shrines in the head covered and without shoes, India. As one walks down the street of as one would in the sacred space of a Chandni Chowk, the main boulevard gurdwara. The entrance to the museum in the old city, the Sis Ganj gurdwara is on the busy fawwara roundabout does a prominent landmark. The fawwara not quite prepare the visitor for the roundabout on which it is located is space inside. The museum has large always busy with the traffic of devotees, open halls, spread over two storeys. both locals who visit the gurdwara daily The display is unusual. In a and those who have travelled into Delhi museum, one typically expects a col- as pilgrims. As a resident of Delhi and lection of old, rare objects which have a historian interested in the city’s past historical value. Here, the display is and its heritage dynamics, it is interest- entirely made up of modern paintings. ing for me to observe the commemo- There are portraits of the Sikh gurus, rations and celebrations around the stories from their life and that of their gurdwara. The gurpurab celebrations followers. These ‘history paintings’ and the accompanying nagar kirtans narrate the story of the Sikh past. are a regular feature of the Sis Ganj These are oil paintings on canvas gurdwara and Chandni Chowk. The made in a western realist style. While fawwara (a blue and white colonial- the workmanship in some paintings is period fountain in the middle of a crude, on the whole it is impressive. -

SIKH HISTORY Book-V
Stories from SIKH HISTORY Book-V Hemkunt STORIES FROM SIKH HISTORY BOOK-V (The Sikh Martyrs) ( I , I , .- C i r .. ; by Kartar" Singh M.A., and Gurdial Singh Dhillon edited by Pam Macormack ~ Hemkunt Press . A-78 Naraina Indl. Area Phase-I New Delhi-llOO28 © Hemkunt Press 1973 Fifteenth impression 1992 lSBlS : 81-~lUlO-olO-O Price Rs. 16 In this series Book I (Guru Nanak Dev) Book II (Guru Angad to Guru Arjun Dev) Book III (Guru Hargobind to Guru Teg Bahadur) Book IV (Guru Gobind Singh) Book V (Si~h Martyrs) Book VI (Banda Singh Bahadur) Book VII -(Maharaja Ranjit Singh) and thereafter till 1989) Printed at Batra Art Printers FOREWORD In this book you will read about some of your noble and glorious ancestors who passed through the portals ofDeath to achieve everlasting life. They gave up their lives on this earth and returned to the Abode of God, to live there for all times to come. Yet they will live also on this earth as long as the noble cause for which they lived and accepted death persists and flourishes. Some misguided people were determined to make their own religion the only religion of the land over which they ruled. Tq all who shared not their faith, they offered the choice between either to give up their faith or face death. Your ancestors ofwhom you will read in the following pages were all offered the above choice. They made their choice of death without even a minute's hesitation. Offers of every sort of earthly joys and pleasures were made to them in wild profusion. -

Guru Teg Bahadur
Guru Teg Bahadur Updated Nov 6, 2017 By Jugraj Kaur About the Author Jugraj Kaur's extraordinary career has spanned over three decades and crossed over two continents. During this time, she has worked in the field of television as well as in the area of education. Her career began in the television industry in New Delhi, India, where she worked as a television producer at the start of her professional career. She was responsible for producing educational shows for children which inspired her to begin her long and fulfilling career in education, first in India and then in the United States. She received her Bachelor of Arts degree in Geography Honors and Library Science from the University of Delhi and then a Master of Science Degree in Geography as well as in Social Work from Jawaharlal Nehru University in New Delhi, India. This allowed her to teach at Mount Carmel High School, a prestigious and well known private establishment in New Delhi for the next ten -

An Introduction to the Sattra Culture of Assam: Belief, Change in Tradition
Journal of Ethnology and Folkloristics 12 (2): 21–47 DOI: 10.2478/jef-2018-0009 AN INTRODUCTION TO THE SATTRA CULT URE OF ASSAM: BELIEF, CHANGE IN TRADITION AND CURRENT ENTANGLEMENT BABURAM SAIKIA PhD Student Department of Estonian and Comparative Folklore University of Tartu Ülikooli 16, 51003 Tartu, Estonia e-mail: [email protected] ABSTRACT In 16th-century Assam, Srimanta Sankaradeva (1449–1568) introduced a move- ment known as eka sarana nama dharma – a religion devoted to one God (Vishnu or Krishna). The focus of the movement was to introduce a new form of Vaishnava doctrine, dedicated to the reformation of society and to the abolition of practices such as animal sacrifice, goddess worship, and discrimination based on caste or religion. A new institutional order was conceptualised by Sankaradeva at that time for the betterment of human wellbeing, which was given shape by his chief dis- ciple Madhavadeva. This came to be known as Sattra, a monastery-like religious and socio-cultural institution. Several Sattras were established by the disciples of Sankaradeva following his demise. Even though all Sattras derive from the broad tradition of Sankaradeva’s ideology, there is nevertheless some theological seg- mentation among different sects, and the manner of performing rituals differs from Sattra to Sattra. In this paper, my aim is to discuss the origin and subsequent transformations of Sattra as an institution. The article will also reflect upon the implication of traditions and of the process of traditionalisation in the context of Sattra culture. I will examine the power relations in Sattras: the influence of exter- nal forces and the support of locals to the Sattra authorities. -

Women Saints in Gaudiya Vaishnavism
Women Saints in Gaudiya Vaishnavism - Jagadananda Das - There are few traditional societies in which women have played a dominant historical role. In this respect, Gaudiya Vaishnavism is no different. The egalitarianism of bhakti movements, which stress the universality of devotion and deny any disqualifications based on birth, sex, or caste, seems to have had limited real effects on the actual social circumstances of any of these classes of people. There are some, including the eminent Bengali historian, Ramakanta Chakravarti, who feel that the status of women was improved in Chaitanya Vaishnavism, mainly due to the singular example of Jahnava Devi. (1) Indeed, it does appear that literacy rates among women (and men) in Vaishnava castes in Bengal were somewhat higher than in other, comparable groups, but this evidence is far from overwhelming. Today, some women may be found playing the role of guru, especially ministering to other women, and there are some Chaitanya Vaishnava women who sing padavali kirtan or give discourses on Vaishnava texts. On the whole, however, despite their dominant numbers at most religious events, the role of women continues to be a supporting one and subordinate to that of men. One question that needs analysis is whether the importance of Radha in the Vaishnava pantheon and the general weight given to the female principle and feminine virtues in the Gaudiya Vaishnava culture has had any influence on the status of women. Many feminist analysts have pointed out that the worship of goddesses has no proven relation to any such amelioration in societies where such worship is conducted. -

Empire's Garden: Assam and the Making of India
A book in the series Radical Perspectives a radical history review book series Series editors: Daniel J. Walkowitz, New York University Barbara Weinstein, New York University History, as radical historians have long observed, cannot be severed from authorial subjectivity, indeed from politics. Political concerns animate the questions we ask, the subjects on which we write. For over thirty years the Radical History Review has led in nurturing and advancing politically engaged historical research. Radical Perspec- tives seeks to further the journal’s mission: any author wishing to be in the series makes a self-conscious decision to associate her or his work with a radical perspective. To be sure, many of us are currently struggling with the issue of what it means to be a radical historian in the early twenty-first century, and this series is intended to provide some signposts for what we would judge to be radical history. It will o√er innovative ways of telling stories from multiple perspectives; comparative, transnational, and global histories that transcend con- ventional boundaries of region and nation; works that elaborate on the implications of the postcolonial move to ‘‘provincialize Eu- rope’’; studies of the public in and of the past, including those that consider the commodification of the past; histories that explore the intersection of identities such as gender, race, class and sexuality with an eye to their political implications and complications. Above all, this book series seeks to create an important intellectual space and discursive community to explore the very issue of what con- stitutes radical history. Within this context, some of the books pub- lished in the series may privilege alternative and oppositional politi- cal cultures, but all will be concerned with the way power is con- stituted, contested, used, and abused. -

Annexure V - Caste Codes State Wise List of Castes
ANNEXURE V - CASTE CODES STATE WISE LIST OF CASTES STATE TAMIL NADU CODE CASTE 1 ADDI DIRVISA 2 AKAMOW DOOR 3 AMBACAM 4 AMBALAM 5 AMBALM 6 ASARI 7 ASARI 8 ASOOY 9 ASRAI 10 B.C. 11 BARBER/NAI 12 CHEETAMDR 13 CHELTIAN 14 CHETIAR 15 CHETTIAR 16 CRISTAN 17 DADA ACHI 18 DEYAR 19 DHOBY 20 DILAI 21 F.C. 22 GOMOLU 23 GOUNDEL 24 HARIAGENS 25 IYAR 26 KADAMBRAM 27 KALLAR 28 KAMALAR 29 KANDYADR 30 KIRISHMAM VAHAJ 31 KONAR 32 KONAVAR 33 M.B.C. 34 MANIGAICR 35 MOOPPAR 36 MUDDIM 37 MUNALIAR 38 MUSLIM/SAYD 39 NADAR 40 NAIDU 41 NANDA 42 NAVEETHM 43 NAYAR 44 OTHEI 45 PADAIACHI 46 PADAYCHI 47 PAINGAM 48 PALLAI 49 PANTARAM 50 PARAIYAR 51 PARMYIAR 52 PILLAI 53 PILLAIMOR 54 POLLAR 55 PR/SC 56 REDDY 57 S.C. 58 SACHIYAR 59 SC/PL 60 SCHEDULE CASTE 61 SCHTLEAR 62 SERVA 63 SOWRSTRA 64 ST 65 THEVAR 66 THEVAR 67 TSHIMA MIAR 68 UMBLAR 69 VALLALAM 70 VAN NAIR 71 VELALAR 72 VELLAR 73 YADEV 1 STATE WISE LIST OF CASTES STATE MADHYA PRADESH CODE CASTE 1 ADIWARI 2 AHIR 3 ANJARI 4 BABA 5 BADAI (KHATI, CARPENTER) 6 BAMAM 7 BANGALI 8 BANIA 9 BANJARA 10 BANJI 11 BASADE 12 BASOD 13 BHAINA 14 BHARUD 15 BHIL 16 BHUNJWA 17 BRAHMIN 18 CHAMAN 19 CHAWHAN 20 CHIPA 21 DARJI (TAILOR) 22 DHANVAR 23 DHIMER 24 DHOBI 25 DHOBI (WASHERMAN) 26 GADA 27 GADARIA 28 GAHATRA 29 GARA 30 GOAD 31 GUJAR 32 GUPTA 33 GUVATI 34 HARJAN 35 JAIN 36 JAISWAL 37 JASODI 38 JHHIMMER 39 JULAHA 40 KACHHI 41 KAHAR 42 KAHI 43 KALAR 44 KALI 45 KALRA 46 KANOJIA 47 KATNATAM 48 KEWAMKAT 49 KEWET 50 KOL 51 KSHTRIYA 52 KUMBHI 53 KUMHAR (POTTER) 54 KUMRAWAT 55 KUNVAL 56 KURMA 57 KURMI 58 KUSHWAHA 59 LODHI 60 LULAR 61 MAJHE -
The Ninth Nanak Guru Teg Bahadar Ji
The Ninth Nanak Guru Teg Bahadar ji March 13, 2021 by dedicated Sewadars of Sri Hemkunt Foundation Inc. INDEX # Title Page # Preface 2 1 Birth and Early Life 4 2 The First Battle 6 3 Stay at Kiratpur 7 4 Stay at Bakala 8 5 First Missionary Tour 9 6 Teg Bahadar as the Ninth Nanak 11 7 Message of Forgiveness 14 8 Selfish Behavior of Sikh Priests 16 9 Establishment of Anandpur 17 Second Missionary Tour and 10 18 Birth of Gobind Rai 11 Right to Freedom of Religion 20 12 Gobind Rai as the Tenth Nanak 22 13 Arrest of the Ninth Nanak 23 14 Martyrdom of the Ninth Nanak 24 15 Travel Map of the Ninth Nanak 27 16 Significant Contributions 28 17 Highlights of the Ninth Nanak’s Life 29 18 Significant World Events 30 References 31 1 Preface Sri Hemkunt Foundation Inc. was established four decades ago (in 1980) in New York, USA. The primary objectives of the Foundation are to help children and youth (6-25 years old) growing up in the Western hemisphere to learn Sikhi, develop public speaking skills, and be proud of being a Sikh. We do this through educational books on the Gurus lives, Sikh history, and Sikh philosophy; and by providing our youth opportunities for demonstrating their knowledge of Sikhi and skillfully communicating this understanding to others. The main Foundation-sponsored event is an annual Symposium. Participants compete in five age-groups: 6-8 years; 9-11 years; 12-14 years; 15-17 years; and 18-25 years. For each group, an age-appropriate book is prescribed. -

Assam State Disaster Management Plan
ASSAM STATE DISASTER MANAGEMENT PLAN ASSAM STATE DISASTER MANAGEMENT AUTHORITY GOVERNMENT OF ASSAM CONTENTS Glossary of Key Terms ................................................................................................... v Abbreviations................................................................................................................vii PART – I DISASTER MANAGEMENT IN ASSAM .....................................................1 SECTION 1: THE ASSAM STATE DISASTER MANAGEMENT PLAN..................... 1 1.1.1 Authority to Plan.........................................................................................1 1.1.2 Aim and Purpose of the Plan.......................................................................1 1.1.3 Scope of the State Disaster Management Plan.............................................1 SECTION 2: PROFILE OF THE STATE ....................................................................... 2 1.2.1 Administrative Divisions ............................................................................2 1.2.2 Demography ...............................................................................................3 1.2.3 Key departments in the State.......................................................................3 1.2.4 Economy ....................................................................................................4 1.2.5 Geography..................................................................................................5 1.2.6 Physiographic Divisions..............................................................................7 -

Dr.Kalyan Das, Assistant Professor, Department of Business Administration, Assam University, Silchar
Dr.Kalyan Das, Assistant Professor, Department of Business Administration, Assam University, Silchar Details of Research Papers Published in Journals: Sl. Name of the Total Title Authors Year Publishers ISSN Number No. Journals Pages SEDME (Small National Institute Impact of Microfinance on Kalyan Das Enterprises, for Micro, Small Housing – A Study on (Co-author: 1 2012 Development, and Medium 10 ISSN: 0970-8464 Narsingpur Development Block Prof. Nikhil Management, Enterprises, of the Cachar District of Assam Bhusan Dey) Extension) Journal Hyderabad. Kalyan Das Department of Role of Apex Level BANIJYA (A Peer (Co-author: Commerce, Assam 2 Microfinance Service Providers 2014 Reviewed Research 10 ISSN: 0975-0010 Prof. Nikhil University, in India Journal) Bhusan Dey) Silchar. PARIPEX-Indian Journal of Research Sara Publishing Growth of Microfinance Sector 3 Kalyan Das 2014 (A Peer Reviewed & Academy, 3 ISSN: 2250-1991 At The International Level Referred International Ahmedabad Journal) Global Journal for Performance of SHG-Bank Research Analysis (A Sara Publishing 4 Linkage Programme in Assam Kalyan Das 2014 Peer Reviewed & Academy, 3 ISSN: 2277-8160 (An Inter-District Analysis) Referred International Ahmedabad Journal) Pratidhwani the Echo Department of Performance of Swarnjayanti Kalyan Das ISSN: (A Peer-Reviewed Bengali, Gram Swarozgar Yojana (Co-author: 2278-5264 (Online) 5 2015 Indexed International Karimganj 7 (SGSY) Prof. Nikhil 2321-9319 (Print) Journal of Humanities College, in the Cachar District of Assam Bhusan Dey) & Social Science) Karimganj, Assam Department of Microfinance – Genesis, Commerce, 6 Kalyan Das 2015 SAMANVAYA 4 ISSN : 2249-4545 Concept and Approaches Gurucharan College, Silchar Kalyan Das Srikishan Sarada Poverty Estimates in India: An (Co-author: 7 2015 PURSUTS College, 8 ISSN : 0976-4593 Inter State Analysis Prof. -

Learning and Educational Achievements in Punjab Schools (LEAPS): Insights to Inform the Education Policy Debate
PAKISTA Learning and Educational Achievements in Punjab Schools (LEAPS): Insights to inform the education policy debate February 20, 2007 Tahir Andrabi, Jishnu Das, Asim Ijaz Khwaja, Tara Vishwanath, Tristan Zajonc 1 And The LEAPS Team 1 The authors’ affiliations are (in order): Andrabi: Pomona College, Das: The World Bank and Centre for Policy Research (New Delhi), Khwaja: Harvard University, Vishwanath: The World Bank and Zajonc: Harvard University. The findings, interpretations, and conclusions expressed in this paper are entirely those of the authors. They do not necessarily represent the view of the World Bank, its Executive Directors, or the countries they represent. ii CURRENCY AND EQUIVALENTS Currency Unit = Pakistan Rupee US$ = PKR 60.5 FISCAL YEAR July 1 – June 30 ACRONYMS AND ABBREVIATIONS AJK Azad Jammu & Kashmir NCTM National Council of Teachers of Mathematics EFA Education for All NWFP North Western Frontier Province EMIS Educational Management Information PIHS Pakistan Integrated Household Survey System FANA PTC Primary Teaching Certificate FATA Federally Administered Tribal Areas STR Student-Teacher Ratio FBS Federal Bureau of Statistics SW GPS Global Positioning System TIMMS Trends in International Math & Science Study ILO International Labor Organization NAGE National Assessment of Governing Board EC National Educational Census Vice President: Praful C. Patel, SARVP Country Director: Yusupha B. Crookes, SACPK Sector Director: John Roome, SASHD Sector Manager: Michelle Riboud, SASHD Task Managers: Tara Vishwanath, SASPR Jishnu Das, DECRG Acknowledgements The LEAPS surveys that form the basis of this report were carried out once a year between 2003 and 2007. A LEAPS year begins with pre-survey field work in July that carries on till November.