Cardiac Pacing in Incomplete Atrioventricular Block with Atrial Fibrillation
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Postural Heart Block*
Br Heart J: first published as 10.1136/hrt.44.2.221 on 1 August 1980. Downloaded from Case reports Br Heart J 1980; 44: 221-3 Postural heart block* PETER E SEDA, JOHN H McANULTY, C JOE ANDERSON From the Department of Medicine, University of Oregon Health Sciences Center, Portland, Oregon, USA SUMMARY A patient presented with orthostatic dizziness and syncope caused by postural heart block. When the patient was supine, atrioventricular conduction was normal and he was asymptomatic; when he was standing he developed second degree type II block and symptoms. The left bundle-branch block on his electrocardiogram and intracardiac electrophysiological study findings suggest that this heart block occurred distal to the His bundle. Orthostatic symptoms are usually presumed to be secondary to an inappropriate distribution of intravascular volume or to autonomic nervous system abnormalities. As shown in this patient, these symptoms may be the result of orthostatic heart block. Ambulatory monitoring may be useful in patients with orthostatic neurological symptoms, particularly when conduction abnormalities are present on the electrocardiogram. Orthostatic neurological symptoms usually result minute and regular, and increased to 90 beats a from inadequate cerebral perfusion caused by minute with some irregularity when he was upright. disturbances of the autonomic nervous system,'-3 The carotid pulse was normal, and there were no ineffective or inappropriate shifts in volume carotid bruits. The cardiac impulse was normal. http://heart.bmj.com/ distribution,4 or drugs.5 We report a patient with The second heart sound was paradoxically split. orthostatic dizziness and syncope caused by inter- There was a grade 2/6 apical systolic murmur. -

First Degree Atrioventricular Block Patrick Loftis Marquette University, [email protected]
Marquette University e-Publications@Marquette Physician Assistant Studies Faculty Research and Physician Assistant Studies, Department Publications 1-21-2011 First Degree Atrioventricular Block Patrick Loftis Marquette University, [email protected] James F. Ginter Aurora Cardiovascular Services Published version. Journal of the American Academy of Physician Assistants, Vol. 24, No. 1 (January 2011). Permalink. © 2011, American Academy of Physician Assistants and Haymarket Media Inc. Used with permission. First-degree atrioventricular blocks - Print Article - JAAPA http://www.jaapa.com/first-degree-atrioventricular-blocks/printarticle/1... << Return to First-degree atrioventricular blocks Patrick Loftis, PA-C, MPAS, RN, James F. Ginter, MPAS, PA-C January 21 2011 An atrioventricular (AV) block is a common cardiac abnormality. It involves a slowing or blockage of the electrical impulse coming from the sinoatrial (SA) node at or around the AV node (Figure 1). AV blocks are characterized by the slowing or partial or complete blocking of the impulse. This discussion will focus on first- degree atrioventricular block, which is the slowing or partial blocking of the impulse; complete blockade will be discussed in a future segment of this department. Despite the name, no impulse is actually blocked in first-degree AV block. Instead, each impulse is simply slowed at or near the atrioventricular node. On an ECG, AV block is manifested by a prolonged PR interval, which is measured from the beginning of the P wave to the beginning of the QRS complex. The ECG criterion for a first-degree atrioventricular block is a PR interval greater than 200 milliseconds. Symptoms First-degree AV block by itself does not result in symptoms. -
Atrioventricular Block in Children with Multisystem Inflammatory Syndrome Audrey Dionne, Douglas Y
Atrioventricular Block in Children With Multisystem Inflammatory Syndrome Audrey Dionne, MD,a,b Douglas Y. Mah, MD,a,b Mary Beth F. Son, MD,b,c Pui Y. Lee, MD, PhD,b,c Lauren Henderson, MD, MMSc,b,c Annette L. Baker, MSC, PNP,a,b Sarah D. de Ferranti, MD,a,b David R. Fulton, MD,a,b Jane W. Newburger, MD, MPH,a,b Kevin G. Friedman, MDa,b BACKGROUND: Children are at risk for multisystem inflammatory syndrome in children (MIS-C) abstract after infection with severe acute respiratory syndrome coronavirus 2. Cardiovascular complications, including ventricular dysfunction and coronary dilation, are frequent, but there are limited data on arrhythmic complications. METHODS: Retrospective cohort study of children and young adults aged #21 years admitted with MIS-C. Demographic characteristics, electrocardiogram (ECG) and echocardiogram findings, and hospital course were described. RESULTS: Among 25 patients admitted with MIS-C (60% male; median age 9.7 [interquartile range 2.7–15.0] years), ECG anomalies were found in 14 (56%). First-degree atrioventricular block (AVB) was seen in 5 (20%) patients a median of 6 (interquartile range 5–8) days after onset of fever and progressed to second- or third-degree AVB in 4 patients. No patient required intervention for AVB. All patients with AVB were admitted to the ICU (before onset of AVB) and had ventricular dysfunction on echocardiograms. All patients with second- or third- degree AVB had elevated brain natriuretic peptide levels, whereas the patient with first- degree AVB had a normal brain natriuretic peptide level. No patient with AVB had an elevated troponin level. -
The Frequency of Rhythm and Conduction Abnormalities and Benefits of 24-Hour Holter Electrocardiogram on Detecting These Abnormalities
ORIGINAL ARTICLE East J Med 24(3): 303-309, 2019 DOI: 10.5505/ejm.2019.31932 The Frequency of Rhythm and Conduction Abnormalities and Benefits of 24-Hour Holter Electrocardiogram on Detecting These Abnormalities In Patients With Acute Rheumatic Fever Serdar Epçaçan*, Yasemin Nuran Dönmez University of Health Sciences, Van Training and Research Hospital, Department of Pediatric Cardiology, Van, Turkey ABSTRACT During the acute phase of acute rheumatic fever (ARF), cardiac arrhythmias and conduction disorders may occur. Standard electrocardiogram (ECG) may be insufficient in the cases of possible paroxysmal rhythm or conduction abnormalities. The aim of this study is to evaluate arrhythmias and conduction disorders and benefits of 24-hour Holter ECG on detecting these disorders in children with ARF. Two hundred and ten patients who were diagnosed with ARF during a four-year period, were retrospectively analyzed. Demographic characteristics, clinical, laboratory, and echocardiographic findings of the patients were evaluated. Standard ECG and 24-hour Holter analysis were examined. First (47.8%), second (6.9%) and third degree (4.3%) atrioventricular (AV) blocks, bundle branch blocks (9.8%), intermittent pre-excitation (1.1%), accelerated nodal rhythm (15.2%), supraventricular (10.9%) and ventricular premature contractions (8.7%), as well as supraventricular (3.3%) and ventricular tachycardia (1.1%) were detected with 24 -hour Holter ECG. Frequency of both rhythm and conduction abnormalities were detected higher with Holter ECG than 12-lead ECG, and this was statistically significant (p<0.05). Second degree type II AV block and non-sustained supraventricular tachycardia as well as intermittent complete AV block were detected on 24-hour Holter analysis in patients with normal initial standard ECG. -

Answer: E) Atrial Fibrillation with Complete Heart Block Teaching Point
Answer: e) Atrial fibrillation with complete heart block Teaching Point: A slow regular ventricular rate in a patient with concurrent atrial fibrillation, as seen in this ECG, is diagnostic of complete heart block. Atrial fibrillation creates a diagnostic dilemma for identifying AV nodal disease or block. Close scrutiny should be placed on R-R intervals to identify patterns or regularity (1). Clinicians should be wary of a regular heart rate in a patient with persistent atrial fibrillation, especially in those using digitalis. If an AV nodal block is identified, it may be transient, and a search for reversible causes is indicated as in all cases of complete heart block prior to pacemaker placement. Electrolyte abnormalities, ischemia, and medications remain the leading reversible causes (2,3). The patient in this case was transferred to the Emergency Department and admitted for further observation. Ischemia was ruled out. Carvedilol was held, and he was diuresed. He continued to demonstrate adequate chronotropic response with exertion. The complete heart block soon resolved, and he was diuresed to euvolemia. Pacemaker placement was deferred given the transient nature of the AV block in the context of recent beta-blocker usage. He was discharged home with continuous heart rhythm monitoring without any further evidence of complete heart block. References: 1. Urbach JR, Grauman JJ, Straus SH. Quantitative Methods for the Recognition of Atrioventricular Junctional Rhythms in Atrial Fibrillation. Circulation. 1969; 39: 803- 817. 2. Kojic EM, Hardarson T, Sigfusson N, Sigvaldason H. The prevalence and prognosis of third-degree atrioventricular conduction block: the Reykjavik study. J Intern Med. -

An Extremely Rare Cause of Wolff-Parkinson
108 Erciyes Med J 2019; 41(1): 108–10 • DOI: 10.14744/etd.2018.18165 An Extremely Rare Cause of Wolff-Parkinson-White Syndrome: Rhabdomyoma in Association With Tuberous Sclerosis CASE REPORT Özlem Elkıran , Cemşit Karakurt , Damla İnce ABSTRACT Rhabdomyomas are the most common primary cardiac tumors in infants and children. They are usually associated with tuberous sclerosis (TS). As the tumors tend to regress spontaneously, surgical intervention is not usually performed unless they become obstructive or cause incessant arrhythmias. We report an extremely rare case of rhabdomyoma serving as a substrate for Wolff-Parkinson-White (WPW) syndrome and intractable supraventricular tachycardia accompanied by TS. Our case is particularly interesting because it was diagnosed prenatally. The signs of WPW syndrome disappeared from the elec- trocardiogram with the regression of the tumor. Keywords: Wolff-Parkinson-White Syndrome, child, rhabdomyoma INTRODUCTION Rhabdomyomas are the most common cardiac tumors in infants and children, and they are closely related with tuberous sclerosis (TS). A significant part of rhabdomyomas is asymptomatic, and they regress on follow-up. However, symptoms of cardiac failure, arrhythmias, and obstruction can be observed depending on their location in the heart. They require urgent medical or surgical treatment (1, 2). Cite this article as: Elkıran Ö, Karakurt C, İnce D. An Extremely Rhabdomyoma-related arrhythmias are reported as premature atrial and ventricular contractions, supraventricular Rare Cause of and ventricular tachycardia, sinus node dysfunction, atrioventricular block, and Wolff-Parkinson-White (WPW) Wolff-Parkinson-White syndrome (1, 3, 4). There are only a few studies of WPW syndrome occurring in association with TS, with and Syndrome: Rhabdomyoma in Association With without rhabdomyoma. -
ACLS Rhythms for the ACLS Algorithms
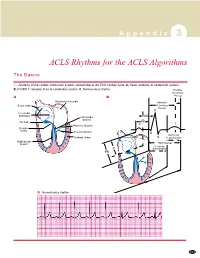
A p p e n d i x 3 ACLS Rhythms for the ACLS Algorithms The Basics 1. Anatomy of the cardiac conduction system: relationship to the ECG cardiac cycle. A, Heart: anatomy of conduction system. B, P-QRS-T complex: lines to conduction system. C, Normal sinus rhythm. Relative Refractory A B Period Bachmann’s bundle Absolute Sinus node Refractory Period R Internodal pathways Left bundle AVN branch AV node PR T Posterior division P Bundle of His Anterior division Q Ventricular Purkinje fibers S Repolarization Right bundle branch QT Interval Ventricular P Depolarization PR C Normal sinus rhythm 253 A p p e n d i x 3 The Cardiac Arrest Rhythms 2. Ventricular Fibrillation/Pulseless Ventricular Tachycardia Pathophysiology ■ Ventricles consist of areas of normal myocardium alternating with areas of ischemic, injured, or infarcted myocardium, leading to chaotic pattern of ventricular depolarization Defining Criteria per ECG ■ Rate/QRS complex: unable to determine; no recognizable P, QRS, or T waves ■ Rhythm: indeterminate; pattern of sharp up (peak) and down (trough) deflections ■ Amplitude: measured from peak-to-trough; often used subjectively to describe VF as fine (peak-to- trough 2 to <5 mm), medium-moderate (5 to <10 mm), coarse (10 to <15 mm), very coarse (>15 mm) Clinical Manifestations ■ Pulse disappears with onset of VF ■ Collapse, unconsciousness ■ Agonal breaths ➔ apnea in <5 min ■ Onset of reversible death Common Etiologies ■ Acute coronary syndromes leading to ischemic areas of myocardium ■ Stable-to-unstable VT, untreated ■ PVCs with -

A Case of Long QT Syndrome
CASE REPORT A case of long QT syndrome: challenges on a bumpy road Peter Magnusson1,2 & Per-Erik Gustafsson2 1Cardiology Research Unit, Department of Medicine, Karolinska Institutet, Stockholm SE-171 76, Sweden 2Centre for Research and Development, Uppsala University/Region Gavleborg,€ Gavle€ SE-801 87, Sweden Correspondence Key Clinical Message Peter Magnusson, Cardiology Research Unit, Department of Medicine, Karolinska Beta-agonist treatment during pregnancy may unmask the diagnosis of long QT Institutet, Karolinska University Hospital/ syndrome. The QT prolongation can result in functional AV block. A history of Solna, SE-171 76 Stockholm, Sweden. Tel: seizure and/or sudden death in a family member should raise suspicion of ven- +46(0)705 089407; Fax: +46(0)26 154255; tricular tachycardia. More than one mutation may coexist. Refusal of beta- E-mail: [email protected] blocker therapy complicates risk stratification. Funding Information Keywords No sources of funding were declared for this Genetic, implantable cardioverter–defibrillator, long QT syndrome, pregnancy, study. premature ventricular complex, risk stratification, sudden cardiac death. Received: 16 December 2016; Revised: 29 March 2017; Accepted: 4 April 2017 Clinical Case Reports 2017; 5(6): 954–960 doi: 10.1002/ccr3.985 Introduction experienced palpitations, and her ECG was abnormal, revealing PVCs, atrioventricular (AV) 2:1 block and QT Long QT syndrome (LQTS) is linked to mutations in the prolongation (520 msec) in precordial lead V5 during ion channels, which can lead to disturbances in ventricu- sinus rhythm at 90 beats per minute (Fig. 1) and rhythm lar repolarization [1]. This condition puts patients at risk strip while walking (Fig. -
Neurological Associations of Chronic Heart Block
J Neurol Neurosurg Psychiatry: first published as 10.1136/jnnp.39.6.571 on 1 June 1976. Downloaded from Journal ofNeurology, Neurosurgery, andPsychiatry, 1976, 39, 571-575 Neurological associations of chronic heart block C. D. LAMBERT AND A. J. FAIRFAX From the Departments of Neurology and Cardiology, St. George's Hospital, London SYNOPSIS A large group of patients with chronic heart block was studied for evidence of neurological disorder. Six out of 892 patients were found who had neuromuscular disease related to the conduction disturbance. In four patients, cardiac involvement appeared selectively to affect the conducting tissues. Three of these patients had a scapuloperoneal syndrome, the fourth, the oculocraniosomatic syndrome. In the remaining two patients, one with limb girdle dystrophy and the other with dystrophia myotonica, cardiomyopathy was present in addition to the conduction disturbance. This paper reports the first comprehensive with incomplete heart block or transient heart study of the frequency and nature of neuro- block secondary to myocardial infarction were not Protected by copyright. logical disorders occurring in association with included. complete heart block. The most common Those cases with evidence of neuromuscular disease were examined in detail, a family history pathological cause of chronic heart block is taken, serum creatine phosphokinase levels meas- idiopathic bundle branch fibrosis (Davies, ured and, when possible, electromyography per- 1971) thought by Lenegre, who described it, to formed. Muscle biopsy specimens, obtained under be a selective myopathy of the cardiac con- local anaesthetic, were examined using conven- ducting 'tissues (Lenegre, 1964). His original tional morphological and histochemical techniques series of 66 cases contained two patients with (Dubowitz and Brooke, 1973). -

Where's the PAC?
Where’s the PAC? A junctional premature contraction (JPC) is a beat that originates prematurely in the AV node. It can occur sporadically or in a grouped pattern. Junctional If PR interval is present, it does NOT represent atrial stimulation of Premature the ventricles. Contraction (JPC) PVC What is this called? Bigeminy - every other beat Trigeminy - every third beat Quadrigeminy - every fourth beat Just how mad Couplets - two in a row are you?? Triplets - three in a row V-Tach - 5 or more PVC’s Multifocal – More than one focus PVC Couplet Multifocal Bigeminy Trigeminy Quadrageminy BBB Hemiblock You are driving into the EKG. You need to turn. You signal. Right or left. Bundle Branch BLOCKS J point: the junction between the end of the QRS segment and the beginning of the ST segment Turn signal theory - Courtesy of Mike Taigman Advanced Field Cardiology “Drive your car” Aortic stenosis Dilated cardiomyopathy LBBB AMI/Extensive CAD Causes Primary disease of the cardiac electrical conduction system Long standing hypertension leading to aortic root dilatation = aortic regurgitation •RVH / Cor pulmonale •PE RBBB •Ischemic heart disease Causes •Rheumatic heart disease •Myocarditis or cardiomyopathy •Degeneration of conduction system “Drive your car” AV Blocks What is actually blocked? A vessel? Is something really “blocked?” Heart Blocks Defined by PR Interval First-Degree Regularity: Regular Heart Block P wave: Normal PR interval: Prolonged >0.20 sec QRS width: Normal Syncopal episode – is this the culprit? First degree AV block is a constant and prolonged PR interval Insult to AV node, hypoxemia, Inferior MI, dig st toxicity, ischemia of the conduction system and 1 Degree AV increased vagal tone Block Criteria Rhythm: Regular PRI: > .20 Degree 2nd Regularity: Regularly irregular AV Block - P wave: Present Type I PR interval: Variable QRS width: Normal Dropped beats: Yes, patterned Long, Longer, Longest, DROP! Rinse and repeat. -

Pharmacological Treatment of Chronic Stable Angina Pectoris
■ DRUG THERAPIES IN... Clinical Medicine 2013, Vol 13, No 1: 63–70 Pharmacological treatment of chronic stable angina pectoris Jason M Tarkin and Juan Carlos Kaski ABSTRACT – Chronic stable angina is the most common Overview of chronic stable angina manifestation of ischaemic heart disease in the developed world and is associated with impaired quality of life and The term angina pectoris refers to William Heberden’s classic increased mortality. The pathogenesis of stable angina is description of the clinical symptoms of angina, as reported to 1 complex and often, albeit not always, involves flow-limiting the Royal College of Physicians in 1768. There is currently no epicardial coronary artery stenoses (atheromatous plaques) systematically agreed definition for angina pectoris and the that reduce the ability of the coronary circulation to deliver term is used to define both the typical chest pain associated appropriate blood supply to the myocardium. The coronary with myocardial ischaemia and the syndrome characterised by microcirculation can also play an important role. An imbal- chest pain, myocardial ischaemia and obstructive atheroscle- ance between myocardial oxygen supply and metabolic rotic coronary artery disease. In this article, we use the term oxygen demand causes the symptoms of angina pectoris ‘angina’ in relation to the occurrence of typical central chest and represents a major therapeutic target. Rational treat- pain associated with myocardial ischaemia, irrespective of the ment requires a multi-faceted approach combining lifestyle presence or absence of flow-limiting organic coronary artery changes, aggressive management of modifiable coronary stenosis. artery disease risk factors, pharmacological therapy and Angina is considered to be ‘chronic’ and ‘stable’ when symp- myocardial revascularisation when appropriate. -

Wolff-Parkinson-White Syndrome Type B with Tachycardia-Dependent
Br Heart J: first published as 10.1136/hrt.43.4.481 on 1 April 1980. Downloaded from Case reports Br HeartJ 1980; 43: 481-6 Wolff-Parkinson-White syndrome type B with tachycardia-dependent (phase 3) block in the accessory pathway and in left bundle-branch coexisting with rate-unrelated right bundle-branch block IVAN J MENDOZA, AGUSTIN CASTELLANOS, RUEY J SUNG From the Division of Cardiology, Department of Medicine, University of Miami School of Medicine, Miami, Florida, USA suMMARY A patient with Wolff-Parkinson-White syndrome type B developed 2:1 atrioventricular block resulting from the association of persistent right bundle-branch block with tachycardia-dependent (phase 3) left bundle-branch block. Electrophysiological studies disclosed the coexistence of a tachy- cardia-dependent (phase 3) block in the accessory pathway. This conduction disturbance was exposed, not by carotid sinus massage as in previous studies, but by pacing-induced prolongation of the interval between two consecutively conducted atrial impulses. Furthermore, the surface electrocardiogram showed, at different times, ventricular complexes resulting from: (1) exclusive atrioventricular conduc- tion through the normal pathway without bundle-branch block; (2) predominant, or exclusive, atrio- ventricular conduction through a right-sided accessory pathway; (3) exclusive atrioventricular conduction http://heart.bmj.com/ through the normal pathway with right bundle-branch block; (4) exclusive conduction through the normal pathway, with left bundle-branch block; (5) fusion between (1) and (2); and finally, (6) fusion between (2) and (3) However, QRS complexes resulting from simultaneously occurring Wolff-Parkinson-White syndrome type B and left bundle-branch block could not be identified.