Sonography of Adenomyosis
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Aderomyoma of the Common Bile Duct --Report of a Case
Yamanashl Med. J. 4 (2), 83"v87, 1989 Case Report AdeRomyoma of the Common Bile Duct --Report of a Case Yoshiro MATsuMoTe, Masatoshi MoGAKi, Hidehisa AoyAMA, Takayoshi SEKmAwA, Katsnhiko SuGAHARA, Koichi SuDAi), and Masayuki FuJiNo2) DePa,rt・ment of Surge7pu. i)DePartment of Pathology, 2)DePartment of lnte7"nal Medicine, YamanasJzi Medical Coglege, Tamaho, Nakakoma, Ya?nanashi 409-38, JaPan Abstract: Adenomyomas in the extrahepatic biie duc£ are extremely rare. In a 75-year- old male with acute cholangitis due to adenomyoma £erming a protruding lesion iR the terminal bile duct, pamacreatoduodenectomy was carried out, resulting complete cure, Key words: Adenomyoma of the common bile duct, Early bile dact cancer, Obstructive jaundice formed, aRd £rom the histologic examina- INTRODUCTION tion of the surgical specimen, adenomyoma Adenomyoma in the biliary ductal system of the common bile duct was confirmed. is most freguently fouRd in the gallbladder. Although beRign neoplasma o£ the bile The gallbiadder wall is more abuRdant in duct system are uncommon, the tumors are muscle fibers than is the wall o£ the bile clinically very important because they can duct. Adenomyoma in the gallbladder is cause obstructive jaundice4) and require knowlt to be closely re}ated to the forma- differentiation £rom eary cancer of the bile tion of gallstones. In other parts of the duct. biliary ductal system, kex4xeve]-, adeno- We report here the surgical results and myoma is very rarei)・2), although a few pathologic findings in a case of adeno- cases of a tumor arising from the papil}a myoma of the terminal bile duct. of Vater3) have beelt reported. -

HIV-1: Cancer Evaluation 8/1/16
Report on Carcinogens Monograph on Human Immunodeficiency Virus Type 1 August 2016 Report on Carcinogens Monograph on Human Immunodeficiency Virus Type 1 August 1, 2016 Office of the Report on Carcinogens Division of the National Toxicology Program National Institute of Environmental Health Sciences U.S. Department of Health and Human Services This Page Intentionally Left Blank RoC Monograph on HIV-1: Cancer Evaluation 8/1/16 Foreword The National Toxicology Program (NTP) is an interagency program within the Public Health Service (PHS) of the Department of Health and Human Services (HHS) and is headquartered at the National Institute of Environmental Health Sciences of the National Institutes of Health (NIEHS/NIH). Three agencies contribute resources to the program: NIEHS/NIH, the National Institute for Occupational Safety and Health of the Centers for Disease Control and Prevention (NIOSH/CDC), and the National Center for Toxicological Research of the Food and Drug Administration (NCTR/FDA). Established in 1978, the NTP is charged with coordinating toxicological testing activities, strengthening the science base in toxicology, developing and validating improved testing methods, and providing information about potentially toxic substances to health regulatory and research agencies, scientific and medical communities, and the public. The Report on Carcinogens (RoC) is prepared in response to Section 301 of the Public Health Service Act as amended. The RoC contains a list of identified substances (i) that either are known to be human carcinogens or are reasonably anticipated to be human carcinogens and (ii) to which a significant number of persons residing in the United States are exposed. The NTP, with assistance from other Federal health and regulatory agencies and nongovernmental institutions, prepares the report for the Secretary, Department of HHS. -

Heavy Menstrual Bleeding
25/06/2018 Definition • Heavy menstrual bleeding (HMB) is defined as excessive menstrual blood loss which interferes with a woman's physical, social, emotional and/or material quality of life. Heavy Menstrual Bleeding (HMB): Replaced ‘menorrhagia’ Objective definition of HMB >80mL/ cycle or duration of >7 days Causes and Management • It can occur alone or in combination with other symptoms (e.g. intermenstrual bleeding, pelvic pain, pressure symptoms) Dr. William (Wee-Liak) Hoo, MD MRCOG Consultant Gynaecologist Prevalence King’s College Hospital NHS FT • The prevalence of HMB in objective studies (9 to 14%) and subjective studies 20 to 52%) in studies based on subjective assessment. • In the UK, almost 1.5 million women consult their General Practitioners UKCPA Women’s Health Group Masterclass (GPs) each year with menstrual complaints and the annual treatment cost Friday 22nd June 2018 exceeds £65 million. Causes • Uterine: Uterine fibroids (dysmenorrhoea, palpable mass, pressure symptoms) Adenomyosis (dysmenorrhoea, subfertility) Endometrial polyps (intermenstrual bleeding) Pelvic inflammatory disease (PID)/ infection (vaginal discharge, pelvic pain, intermenstrual and postcoital bleeding and pyrexia) Malignancy or atypical hyperplasia (irregular/ postcoital/ intermenstrual bleeding, pelvic pain, weight loss). • Ovarian: Polycystic ovary syndrome (acne, hursuitism) • Systemic diseases: Hypothyroidism (fatigue, constipation, cold intolerance and hair and skin changes) Coagulation disorders (e.g. von Willebrand disease) Liver -

SNOMED CT Codes for Gynaecological Neoplasms
SNOMED CT codes for gynaecological neoplasms Authors: Brian Rous1 and Naveena Singh2 1Cambridge University Hospitals NHS Trust and 2Barts Health NHS Trusts Background (summarised from NHS Digital): • SNOMED CT is a structured clinical vocabulary for use in an electronic health record. It forms an integral part of the electronic care record, and serves to represent care information in a clear, consistent, and comprehensive manner. • The move to a single terminology, SNOMED CT, for the direct management of care of an individual, across all care settings in England, is recommended by the National Information Board (NIB), in “Personalised Health and Care 2020: A Framework for Action”. • SNOMED CT is owned, managed and licensed by SNOMED International. NHS Digital is the UK Member's National Release Centre for the creation of, and delegated authority to licence the SNOMED CT Edition and derivatives. • The benefits of using SNOMED CT in electronic care records are that it: • enables sharing of vital information consistently within and across health and care settings • allows comprehensive coverage and greater depth of details and content for all clinical specialities and professionals • includes diagnosis and procedures, symptoms, family history, allergies, assessment tools, observations, devices • supports clinical decision making • facilitates analysis to support clinical audit and research • reduces risk of misinterpretations of the record in different care settings • Implementation plans for England: • SNOMED CT must be implemented across primary care and deployed to GP practices in a phased approach from April 2018. • Secondary care, acute care, mental health, community systems, dentistry and other systems used in direct patient care must use SNOMED CT as the clinical terminology, before 1 April 2020. -

Polypoid Adenomyoma of the Uterus
Open Access Case Report DOI: 10.7759/cureus.4044 Polypoid Adenomyoma of the Uterus Nida Sajjad 1 , Hina Iqbal 1 , Kumail Khandwala 1 , Shaista Afzal 1 1. Radiology, Aga Khan University Hospital, Karachi, PAK Corresponding author: Kumail Khandwala, [email protected] Abstract Polypoid adenomyoma is a rare uterine endometrial polypoid tumor of mixed epithelial and mesenchymal origin. Although the clinical and pathologic features of polypoid adenomyomas have been described extensively, imaging findings for these tumors have not been frequently reported in the literature. On imaging, their features may be confused with prolapsed leiomyomas or malignancy. Hemorrhagic cystic spaces in a prolapsed uterine tumor within the vagina should raise consideration of a diagnosis of polypoid adenomyoma. Such blood-containing cystic spaces would be unusual findings in leiomyomas and malignancy. Diagnosing polypoid adenomyoma is vital because it can potentially be managed by hysteroscopic resection, unlike an ordinary form of adenomyosis. Categories: Obstetrics/Gynecology, Radiology Keywords: mesenchymal tumor, atypical polypoid adenomyoma, uterus Introduction Polypoid adenomyoma of the uterus is an endometrial polyp in which the stromal component is made up of smooth muscle [1]. These are benign tumors and account for 1.3% of all endometrial polyps. Polypoid adenomyomas are of mixed epithelial and mesenchymal origin [2]. Although their clinical and pathological features have been described well in literature, imaging findings for these tumors have been seldom reported. We report a case of a 44-year-old woman with urinary retention who had a prolapsed polypoidal uterine lesion on imaging which was confirmed to be polypoid adenomyoma on histopathology. We aim to review the imaging findings and the relevant literature on this rare entity. -
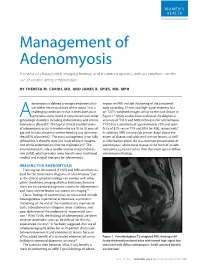
Management of Adenomyosis a Review of Characteristic Imaging Findings and Treatment Options, with an Emphasis on the Use of Uterine Artery Embolization
WOMEN’S HEALTH Management of Adenomyosis A review of characteristic imaging findings and treatment options, with an emphasis on the use of uterine artery embolization. BY THERESA M. CARIDI, MD, AND JAMES B. SPIES, MD, MPH denomyosis is defined as ectopic endometrial tis- myosis on MRI include thickening of the junctional sue within the musculature of the uterus.1 It is a zone exceeding 12 mm and high-signal-intensity foci challenging condition in that it often overlaps in on T2/T1-weighted images similar to the case shown in symptoms and is found in conjunction with other Figure 1.4 Many studies have evaluated the diagnostic Agynecologic disorders, including endometriosis and uterine accuracy of TVUS and MRI techniques for adenomyosis. leiomyoma (fibroids).2 The typical clinical manifestations TVUS has a sensitivity of approximately 72% and speci- of adenomyosis occur in women who are 40 to 50 years of ficity of 81% versus 77% and 89% for MRI, respectively.8 age and include abnormal uterine bleeding and dysmenor- In addition, MRI can provide greater detail about the rhea (65% of patients).1 The exact pathogenesis is not fully extent of disease and additional uterine lesions, as well defined but is thought to be the result of direct invagina- as information about the less common presentation of tion of the endometrium into the myometrium.3 The adenomyosis, where focal disease in the form of an ade- interventionalist’s role is to offer uterine artery emboliza- nomyoma is present rather than the more typical diffuse tion (UAE), which provides some benefits over traditional adenomyosis findings. -

Conversion of Morphology of ICD-O-2 to ICD-O-3
NATIONAL INSTITUTES OF HEALTH National Cancer Institute to Neoplasms CONVERSION of NEOPLASMS BY TOPOGRAPHY AND MORPHOLOGY from the INTERNATIONAL CLASSIFICATION OF DISEASES FOR ONCOLOGY, SECOND EDITION to INTERNATIONAL CLASSIFICATION OF DISEASES FOR ONCOLOGY, THIRD EDITION Edited by: Constance Percy, April Fritz and Lynn Ries Cancer Statistics Branch, Division of Cancer Control and Population Sciences Surveillance, Epidemiology and End Results Program National Cancer Institute Effective for cases diagnosed on or after January 1, 2001 TABLE OF CONTENTS Introduction .......................................... 1 Morphology Table ..................................... 7 INTRODUCTION The International Classification of Diseases for Oncology, Third Edition1 (ICD-O-3) was published by the World Health Organization (WHO) in 2000 and is to be used for coding neoplasms diagnosed on or after January 1, 2001 in the United States. This is a complete revision of the Second Edition of the International Classification of Diseases for Oncology2 (ICD-O-2), which was used between 1992 and 2000. The topography section is based on the Neoplasm chapter of the current revision of the International Classification of Diseases (ICD), Tenth Revision, just as the ICD-O-2 topography was. There is no change in this Topography section. The morphology section of ICD-O-3 has been updated to include contemporary terminology. For example, the non-Hodgkin lymphoma section is now based on the World Health Organization Classification of Hematopoietic Neoplasms3. In the process of revising the morphology section, a Field Trial version was published and tested in both the United States and Europe. Epidemiologists, statisticians, and oncologists, as well as cancer registrars, are interested in studying trends in both incidence and mortality. -

Chronic Vulvar Irritation, Itching, and Pain. What Is the Diagnosis?
SECOND OF 2 PARTS ON OFFICE MANAGEMENT OF BENIGN VULVAR CONDITIONS Chronic vulvar irritation, itching, and pain. What is the diagnosis? Five cases of dermatoses, vaginal abnormalities, and pain syndromes that may masquerade as infection Libby Edwards, MD, and Beth E. Goldbaum, MD hronic irritation, itching, and pain CASE 1 Introital burning and a fear are only rarely due to infection. of breast cancer C These symptoms are more likely to A 56-year-old woman visits your office for be caused by dermatoses, vaginal abnormali- management of recent-onset introital burn- ties, and pain syndromes that may be difficult ing during sexual activity. She reports that to diagnose. Careful evaluation should in- her commercial lubricant causes irritation. clude a wet mount and culture to eliminate Topical and oral antifungal therapies have not infection as a cause so that the correct diag- been beneficial. She has a strong family his- IN THIS nosis can be ascertained and treated. tory of breast cancer. ARTICLE In Part 2 of this two-part series, we focus On examination, she exhibits small, When a woman on five cases of vulvar dermatologic disrup- smooth labia minora and experiences pain is reluctant to use tions: when a cotton swab is pressed against the local estrogen • atrophic vagina vestibule. The vagina is also smooth, with page 32 • irritant and allergic contact dermatitis scant secretions. Microscopically, these • complex vulvar aphthosis secretions are almost acellular, with no • desquamative inflammatory vaginitis increase in white blood cells and no clue A teenager • inverse psoriasis. cells, yeast forms, or lactobacilli. The pH is with vulvar pain greater than 6.5, and most epithelial cells are and sores parabasal (FIGURE 1, page 32). -

Managing Infertility When Adenomyosis and Endometriosis Co-Exist
Managing infertility when adenomyosis and endometriosis co-exist Jinhua Leng Beijing,China 27th April 2018 • IPSEN symposium Endometriosis • Endometriosis (EM) is a common, benign, ovary hormone-dependent gynecologic disorder which affects mainly reproductive-age women • Endometriosis is considered to be responsible for infertility and pelvic pain • May affect 10% of women of reproductive age • Three types of pelvic endometriosis • Peritoneal Endometriosis • Ovarian Endometrioma • Deeply Infiltrating Endometriosis (DIE) 27th April 2018 • IPSEN symposium Adenomyosis • Adenomyosis (AD) is defined by the presence of endometrial glands and stroma in the myometrium • Prevalence: varies significantly between studies (from 5% to 70%), generally underestimated • Most frequent symptoms: dysmenorrhea, abnormal uterine bleeding, etc. • Two types: diffuse form, focal form 27th April 2018 • IPSEN symposium PEM DIE OEM AD+EM 27th April 2018 • IPSEN symposium Macroscopic and microscopic appearance of AD 27th April 2018 • IPSEN symposium MRI Features of AD—focal and diffuse 27th April 2018 • IPSEN symposium Prevalence of EM in patients with AD Adenomyosis Endometriosis Author N N(%) Leng JH et al.(2011) 72(histology) 24(33.3%) Di Donato et al. (2014) 217(ultrasound) 165(76.0%) Chapron et al. (2017) 175(MRI) 153(87.4%) Leyendecker et al. (2015) 67(MRI) 54(80.6%) Em and AD often coexist Several authors reported the prevalence of EM in patients with AD. Our study showed in 72 histologically diagnosed AD, 33.3% had concomitant EM. Chapron and another 2 authors reported in US/MRI diagnosed AD, 76-87% had coexistant EM 27th April 2018 • IPSEN symposium What is the relationship between endometriosis phenotypes and adenomyosis? EM subtype N Diffuse form Focal form PEM 40 8(20.0%) 3(7.5%) OEM 31 14(45.2%) 6(19.3%) DIE 166 59(35.5%) 110(66.3%) • Surgery findings of 175 preoperatively MRI diagnosed AD and histologically diagnosed of EM • Among EM women, diffuse AD had no correlation with EM phenotypes. -

Adenomyosis and Infertility
Reproductive BioMedicine Online (2012) 24,35– 46 www.sciencedirect.com www.rbmonline.com REVIEW Adenomyosis and infertility Sebastiano Campo a, Vincenzo Campo a,*, Giuseppe Benagiano b a Institute of Obstetrics and Gynaecology, Catholic University of Sacred Heart, Rome, Italy; b Department of Obstetrics, Gynaecology and Urology, Sapienza, University of Rome, Rome, Italy * Corresponding author. E-mail address: [email protected] (V Campo). Prof Sebastiano Campo has been associate professor in the Department of Obstetrics and Gynecology at the Catholic University of the Sacred Heart in Rome since 1984. His special interests include ovarian physiology, infertility, endometriosis and polycystic ovary syndrome. Abstract Today an accurate diagnosis of adenomyosis can be made thanks to progress in imaging techniques: sonography and mag- netic resonance imaging (MRI). This has made it possible to clinically correlate the presence of adenomyosis to infertility. At the same time, a series of pathogenetic hypotheses have been presented to explain this correlation. First, the identification of the myo- metrial junctional zone (JZ) and of its disruption and thickening has been linked to poor reproductive performance mainly through perturbed uterine peristalsis, a phenomenon that originates exclusively from the JZ in the nonpregnant uterus. In addition, a number of biochemical and functional alterations in both eutopic and heterotopic endometrium in women with adenomyosis have now been found to lead to lower receptivity, indicated by the presence of ‘implantation marker’ defects. In these patients there is also an altered decidualization and abnormal concentrations of intrauterine free radicals. All these abnormalities in the endometrial envi- ronment seem to contribute to subfertility. Several attempts have been made to restore fertility in adenomyosis patients, the oldest being gonadotrophin-releasing hormone agonists coupled to conservative surgery. -

Atypical Stromal Cells As a Diagnostic Pitfall in Lesions of the Lower Female Genital Tract and Uterus: a Review and Presentation of Some Unusual Cases
Patología 2009;47(2):103-7 Revista latinoamericana 2ULJLQDODUWLFOH Atypical stromal cells as a diagnostic pitfall in lesions of the lower female genital tract and uterus: a review and presentation of some unusual cases MI Rodrigues,* E Goez,** K Larios K,*** M Cuevas,**** J Aneiros Fernandez,**** S Stolnicu,1 FF Nogales**** RESUMEN Antecedentes: las células estromales atípicas (CEAts) en el conducto genital femenino son un hallazgo poco frecuente en lesiones polipoides de vulva, vagina, cuello uterino y endometrio, lo que con frecuencia genera errores diagnósticos. Objetivo: mostrar los hallazgos de 12 casos enviados a consulta por la sospecha de una lesión maligna. Material y métodos: estudio clínico-patológico de 12 casos con inmunohistoquímica de actina, desmina, S100, Ki67, RE y RP. Resultados: las células estromales atípicas se encontraron en un patrón multifocal, en tres casos de lesiones de vulva (incluido un caso de liquen escleroso), dos pólipos vaginales, dos casos de cuello uterino, incluido uno prolapsado y un carcinoma escamoso y, por último, cuatro casos de pólipos endometriales y un caso de adenomiosis. Los marcadores de inmunohistoquímica en las células estromales atí- picas fueron positivos para receptores hormonales de estrógenos y progesterona y sólo focalmente para actina. El índice de proliferación Ki67 fue bajo. ConclusionesODVFpOXODVHVWURPDOHVDWtSLFDVVRQUHDFWLYDVQRHVSHFt¿FDVRGHJHQHUDWLYDVFRQXQtQGLFHGHSUROLIHUDFLyQPX\EDMRFRQ receptores hormonales y capacidad para expresar marcadores de músculo liso y de estroma endometrial. Presentamos casos, hasta ahora no publicados, de células estromales atípicas asociadas a un liquen escleroso en la vulva, un carcinoma escamoso del cuello uterino y un cuello uterino prolapsado. Se plantean además, como diagnósticos diferenciales, sitio de implantación exagerado y nevo azul, ya que las células trofoblásticas y névicas presentan características similares a las células estromales atípicas. -

BMC Medical Informatics and Decision Making Biomed Central
BMC Medical Informatics and Decision Making BioMed Central Software Open Access Automatic extraction of candidate nomenclature terms using the doublet method Jules J Berman* Address: Cancer Diagnosis Program, National Cancer Institute, National Institutes of Health, Bethesda, MD, USA Email: Jules J Berman* - [email protected] * Corresponding author Published: 18 October 2005 Received: 07 January 2005 Accepted: 18 October 2005 BMC Medical Informatics and Decision Making 2005, 5:35 doi:10.1186/1472-6947-5-35 This article is available from: http://www.biomedcentral.com/1472-6947/5/35 © 2005 Berman; licensee BioMed Central Ltd. This is an Open Access article distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/2.0), which permits unrestricted use, distribution, and reproduction in any medium, provided the original work is properly cited. Abstract Background: New terminology continuously enters the biomedical literature. How can curators identify new terms that can be added to existing nomenclatures? The most direct method, and one that has served well, involves reading the current literature. The scholarly curator adds new terms as they are encountered. Present-day scholars are severely challenged by the enormous volume of biomedical literature. Curators of medical nomenclatures need computational assistance if they hope to keep their terminologies current. The purpose of this paper is to describe a method of rapidly extracting new, candidate terms from huge volumes of biomedical text. The resulting lists of terms can be quickly reviewed by curators and added to nomenclatures, if appropriate. The candidate term extractor uses a variation of the previously described doublet coding method.