WES MATTHEWS, Sr
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

O Klahoma City
MEDIA GUIDE O M A A H C L I K T Y O T R H U N D E 2 0 1 4 2 0 1 5 THUNDER.NBA.COM TABLE OF CONTENTS GENERAL INFORMATION ALL-TIME RECORDS General Information .....................................................................................4 Year-By-Year Record ..............................................................................116 All-Time Coaching Records .....................................................................117 THUNDER OWNERSHIP GROUP Opening Night ..........................................................................................118 Clayton I. Bennett ........................................................................................6 All-Time Opening-Night Starting Lineups ................................................119 2014-2015 OKLAHOMA CITY THUNDER SEASON SCHEDULE Board of Directors ........................................................................................7 High-Low Scoring Games/Win-Loss Streaks ..........................................120 All-Time Winning-Losing Streaks/Win-Loss Margins ...............................121 All times Central and subject to change. All home games at Chesapeake Energy Arena. PLAYERS Overtime Results .....................................................................................122 Photo Roster ..............................................................................................10 Team Records .........................................................................................124 Roster ........................................................................................................11 -

FOR IMMEDIATE RELEASE: August 2, 2017
FOR IMMEDIATE RELEASE: August 2, 2017 Ronnie Lester will Host Event for Kenny Arnold Foundation During Labor Day Weekend; Fans Have a Chance to Meet the Stars of Iowa’s 1980 Final Four Team IOWA CITY, IA – Ronnie Lester, widely regarded as the best basketball player in Hawkeye history, will be making one of his all-time greatest assists this Labor Day weekend in Iowa City. Lester, along with almost the entire 1980 Final Four basketball team, will be accessible to Hawk fans at a special fundraising event in Iowa City in support of the Kenny Arnold Foundation. Kenny Arnold, who led that Hawkeye team in points and assists, was diagnosed with brain cancer in 1984 and has been fighting health issues ever since. The brain tumor and several subsequent strokes have limited Arnold’s mobility, robbed him of his ability to speak and left him in a state of chronic pain. Arnold’s former Iowa teammates and coaches, and the entire Hawkeye Basketball Family, have stayed in contact with Arnold throughout his medical and financial challenges. Today, Arnold’s Hawkeye Basketball Family – his “Teammates For Life” – have dedicated their efforts to provide support for Arnold and others in need through this foundation. “We know that what happened to Kenny could happen to any of us,” said Lester, a Hawkeye All- American on Iowa’s 1979 Big Ten championship team. “All the guys have rallied around him and I’m so proud of my teammates for that. Kenny is very appreciative of all the love and support that his teammates and the Iowa fans have shown him.” Meet and Greet at the Marriott Hotel The event will be a “Meet and Greet” on Friday, September 1 at the Marriott Hotel in Coralville from 7 p.m. -

University of Cincinnati News Record. Thursday, January 26, 1967. Vol
State· Affiliation Proposed; ,UC: To Benefit Financially by Peter Franklin "The UC students.would be bene- fitted because of Iower fees coup- A plan proposin-g state affilia- led' with broader graduate and tion for UC has 'received the sup- professional offerings. The bene- port of the Ohio Board of Regents. fit to' the University would come The University would continue I from the acquisition ,of a broader under local control and retain its fina~cial base without the loss of' municipal status, but the accept- local ties and support." ance of the- proposal would result Dr.: Langsam explained that in greatly expanded financial aid ' "the City of Cincinnati would reap or the University. benefit from the proposal because l:owerTu.itlonFees of \ the lower instructional fees The most immediate benefit. to made available to its citizens as . ,,', . i '. .~'i 1...b .•...;;0. i " 'U\e uc student would be a drop in well as the millions of new -dollars that would flow into the. city ec- ,ordie Beats AII-Ameri~ci1" es:JtO?M~~~;sa~:6~iOcr.i~~i~~n.a:~:onomy., The city also would bene- r- G ,-, " . \i ~~- ~~ commenting on the proposed - fit from having a University that _ --"" " " ....• . •..•• plan Dr. Walter G. Langsam, UC was - better able to respond to f '" .. - '._, .' . ': '.~ . President, explained that the plan community. needs for 'expanded Later Drops No ..2..Lou. vOre ,. for state affiliation would-benefit and newprograms." , the students, the university, the "The state itself also would by Mike Kelly city and -the state. benefit because it means imple- University of Louisville's Cardi- menting the Regents' master plan nals could, take a tip from the in Southwestern Ohio at consider- Pinkerton police agency: the ,way F~iday/s Concert ably less expense than the· es- to cover Gordie Smith is to put tablishment of a new state uni- three men on him. -

Cardinal Tradition Louisville Basketball
Cardinal Tradition Louisville Basketball Louisville Basketball Tradition asketball is special to Kentuckians. The sport B permeates everyday life from offices to farm- lands, from coal mines to neighborhood drug stores. It is more than just a sport played in the cold winter months. It is a source of pride filled year-round with anticipation, hope and celebration. Kentuckians love their basketball, and the tradition-rich University of Louisville program has supplied its fans with one of the nation’s finest products for decades. Legendary coach Bernard “Peck” Hickman, a Basketball Hall of Fame nominee, arrived on the UofL campus in 1944 to begin a remarkable string of 46 consecutive winning seasons. For 23 seasons, Hickman laid an impressive foundation for UofL. John Dromo, an assistant coach under Hickman for 19 years, continued the Louisville program in outstanding fashion following Hickman’s retirement. For 30 years, Denny Crum followed the same path of success that Hickman and Dromo both walked, guiding the Cardinals to even higher acclaim. Now, Coach Rick Pitino energized a re-emergence in building upon the rich UofL tradition in his 16 years, guiding the Cardinals to the 2013 NCAA championship, NCAA Final Fours in 2005 and 2012 and the NCAA Elite Eight five of the past 10 sea- sons. Among the Cardinals’ past successes include national championships in the NCAA (1980,1986, 2013), NIT (1956) and the NAIB (1948). UofL is Taquan Dean kisses the Freedom Hall floor Tremendous pride is taken in the tradition the only school in the nation to have claimed the after his final game as a Cardinal. -

Renormalizing Individual Performance Metrics for Cultural Heritage Management of Sports Records
Renormalizing individual performance metrics for cultural heritage management of sports records Alexander M. Petersen1 and Orion Penner2 1Management of Complex Systems Department, Ernest and Julio Gallo Management Program, School of Engineering, University of California, Merced, CA 95343 2Chair of Innovation and Intellectual Property Policy, College of Management of Technology, Ecole Polytechnique Federale de Lausanne, Lausanne, Switzerland. (Dated: April 21, 2020) Individual performance metrics are commonly used to compare players from different eras. However, such cross-era comparison is often biased due to significant changes in success factors underlying player achievement rates (e.g. performance enhancing drugs and modern training regimens). Such historical comparison is more than fodder for casual discussion among sports fans, as it is also an issue of critical importance to the multi- billion dollar professional sport industry and the institutions (e.g. Hall of Fame) charged with preserving sports history and the legacy of outstanding players and achievements. To address this cultural heritage management issue, we report an objective statistical method for renormalizing career achievement metrics, one that is par- ticularly tailored for common seasonal performance metrics, which are often aggregated into summary career metrics – despite the fact that many player careers span different eras. Remarkably, we find that the method applied to comprehensive Major League Baseball and National Basketball Association player data preserves the overall functional form of the distribution of career achievement, both at the season and career level. As such, subsequent re-ranking of the top-50 all-time records in MLB and the NBA using renormalized metrics indicates reordering at the local rank level, as opposed to bulk reordering by era. -
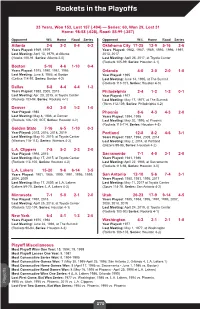
Rockets in the Playoffs
Rockets in the Playoffs 33 Years, Won 153, Lost 157 (.494) — Series: 60, Won 29, Lost 31 Home: 98-58 (.628), Road: 55-99 (.357) Opponent W-L Home Road Series Opponent W-L Home Road Series Atlanta 2-6 2-2 0-4 0-2 Oklahoma City 17-25 12-9 5-16 2-6 Years Played: 1969, 1979 Years Played: 1982, 1987, 1989, 1993, 1996, 1997, Last Meeting: April 13, 1979, at Atlanta 2013, 2017 (Hawks 100-91, Series: Atlanta 2-0) Last Meeting: April 25, 2017, at Toyota Center (Rockets 105-99, Series: Houston 4-1) Boston 5-16 4-6 1-10 0-4 Years Played: 1975, 1980, 1981, 1986 Orlando 4-0 2-0 2-0 1-0 Last Meeting: June 8, 1986, at Boston Year Played: 1995 (Celtics 114-97, Series: Boston 4-2) Last Meeting: June 14, 1995, at The Summit (Rockets 113-101, Series: Houston 4-0) Dallas 8-8 4-4 4-4 1-2 Years Played: 1988, 2005, 2015 Philadelphia 2-4 1-2 1-2 0-1 Last Meeting: Apr. 28, 2015, at Toyota Center Year Played: 1977 (Rockets 103-94, Series: Rockets 4-1) Last Meeting: May 17, 1977, at The Summit (76ers 112-109, Series: Philadelphia 4-2) Denver 4-2 3-0 1-2 1-0 Year Played: 1986 Phoenix 8-6 4-3 4-3 2-0 Last Meeting: May 8, 1986, at Denver Years Played: 1994, 1995 (Rockets 126-122, 2OT, Series: Houston 4-2) Last Meeting: May 20, 1995, at Phoenix (Rockets 115-114, Series: Houston 4-3) Golden State 7-16 6-5 1-10 0-3 Year Played: 2015, 2016, 2018, 2019 Portland 12-8 8-2 4-6 3-1 Last Meeting: May 10, 2019, at Toyota Center Years Played: 1987, 1994, 2009, 2014 (Warriors 118-113), Series: Warriors 4-2) Last Meeting: May 2, 2014, at Portland (Blazers 99-98, Series: Houston 4-2) L.A. -

2012-13 BOSTON CELTICS Media Guide
2012-13 BOSTON CELTICS SEASON SCHEDULE HOME AWAY NOVEMBER FEBRUARY Su MTWThFSa Su MTWThFSa OCT. 30 31 NOV. 1 2 3 1 2 MIA MIL WAS ORL MEM 8:00 7:30 7:00 7:30 7:30 4 5 6 7 8 9 10 3 4 5 6 7 8 9 WAS PHI MIL LAC MEM MEM TOR LAL MEM MEM 7:30 7:30 8:30 1:00 7:30 7:30 7:00 8:00 7:30 7:30 11 12 13 14 15 16 17 10 11 12 13 14 15 16 CHI UTA BRK TOR DEN CHA MEM CHI MEM MEM MEM 8:00 7:30 8:00 12:30 6:00 7:00 7:30 7:30 7:30 7:30 7:30 18 19 20 21 22 23 24 17 18 19 20 21 22 23 DET SAN OKC MEM MEM DEN LAL MEM PHO MEM 7:30 7:30 7:30 7:AL30L-STAR 7:30 9:00 10:30 7:30 9:00 7:30 25 26 27 28 29 30 24 25 26 27 28 ORL BRK POR POR UTA MEM MEM MEM 6:00 7:30 7:30 9:00 9:00 7:30 7:30 7:30 DECEMBER MARCH Su MTWThFSa Su MTWThFSa 1 1 2 MIL GSW MEM 8:30 7:30 7:30 2 3 4 5 6 7 8 3 4 5 6 7 8 9 MEM MEM MEM MIN MEM PHI PHI MEM MEM PHI IND MEM ATL MEM 7:30 7:30 7:30 7:30 7:30 7:00 7:30 7:30 7:30 7:00 7:00 7:30 7:30 7:30 9 10 11 12 13 14 15 10 11 12 13 14 15 16 MEM MEM MEM DAL MEM HOU SAN OKC MEM CHA TOR MEM MEM CHA 7:30 7:30 7:30 8:00 7:30 8:00 8:30 1:00 7:30 7:00 7:30 7:30 7:30 7:30 16 17 18 19 20 21 22 17 18 19 20 21 22 23 MEM MEM CHI CLE MEM MIL MEM MEM MIA MEM NOH MEM DAL MEM 7:30 7:30 8:00 7:30 7:30 7:30 7:30 7:30 8:00 7:30 8:00 7:30 8:30 8:00 23 24 25 26 27 28 29 24 25 26 27 28 29 30 MEM MEM BRK MEM LAC MEM GSW MEM MEM NYK CLE MEM ATL MEM 7:30 7:30 12:00 7:30 10:30 7:30 10:30 7:30 7:30 7:00 7:00 7:30 7:30 7:30 30 31 31 SAC MEM NYK 9:00 7:30 7:30 JANUARY APRIL Su MTWThFSa Su MTWThFSa 1 2 3 4 5 1 2 3 4 5 6 MEM MEM MEM IND ATL MIN MEM DET MEM CLE MEM 7:30 7:30 7:30 8:00 -

Pat Williams Co-Founder and Senior Vice President of the Orlando Magic
Pat Williams Co-Founder and Senior Vice President of the Orlando Magic Leadership. With his vast experience leading NBA teams to the finals and grooming players into great coaches, Pat Williams knows how to identify and develop the universal qualities that all great leaders share. An author of more than 60 books – some of which address leadership and public speaking, Williams is adept at giving his audience the motivation and tools they need in order to affect real change at their organizations. In his presentations, he discusses leadership and the qualities leaders must possess, all while sharing insider sports stories, addressing how he himself became a leader, motivating his audience, and acting as a catalyst for change. Teamwork. Pat Williams has led 23 teams to the NBA playoffs and five to the finals, and largely part of his success has been his ability to meld great talents—like Dr. J and Moses Malone, Charles Barkley and Maurice Cheeks, and Shaquille O’Neal and “Penny” Hardaway—into championship teams and teammates. With this incredible experience (he has spent 49 years as a player and executive in professional baseball and basketball), Williams addresses how to create great teams that act as one and work toward common goals. During his presentations, he address teamwork, how to create and maintain great teams, conflict resolution, and overcoming adversity—all while sharing insider sports stories and offering his audience the necessary tools for affecting real change at their organizations. Winning. Having led 23 teams to the NBA playoffs and five to the finals, Pat Williams knows a thing or two about winning. -

Coaching Staff Coaching Staff Head Coach Lorenzo Romar
HuskiesCoaching Staff Coaching Staff Head Coach Lorenzo Romar Washington men’s ship and finish 31-2. Cameron Dollar, an assistant • Saint Louis won their first conference tourna- basketball coach coach on Romar’s Saint Louis and Washington ment championship in the program’s history. Lorenzo Romar was staffs, was one of the stars for the Bruins during named to head up that national title contest, replacing injured point • The Billikens became the first No. 9 seed to the program at his guard Tyus Edney in the starting lineup. win the Conference USA Tournament. alma mater on April Romar built a reputation as one of the nation’s top • Saint Louis upset a No. 1 team, Cincinnati, for 3, 2002. A point recruiters while an assistant at UCLA (1992-1996) the first time since the 1951-52 season when guard for the Hus- and was credited with recruiting much of the talent the Bills knocked off top-ranked Kentucky. kies’ 1978-79 and that formed the core of the Bruins’ title team. 1979-80 teams, • The Billikens won the first Bud Light Show- Romar is the 18th In three years at Saint Louis, Romar compiled a down by knocking off intrastate rival Missouri head coach in 51-44 (.537) record, including victories over nine for the first time since the 1970-71 season. Washington’s 101- different conference champions. His 51 wins rank After reaching the NCAA Tournament in his first year history. He is the first African-American No. 7 among all-time SLU coaches and is the season, expectations were high for Romar’s 2000- coach to lead the Washington basketball program. -

Aw a Rd Wi Nners
Awar MBKB02 10/21/02 10:19 AM Page 107 Awa r d Win n e r s Division I Consensus All-American Selections.. .1 0 8 Division I Academic All-Americans By Tea m. .1 1 3 Division I Player of the Yea r .. .1 1 4 Divisions II and III Fi r s t - Te a m All-Americans By Tea m. .1 1 6 Divisions II and III Ac a d e m i c All-Americans By Tea m. .1 1 8 NCAA Postgraduate Scholarship Winners By Tea m .. .1 1 9 Awar MBKB02 10/21/02 10:19 AM Page 108 10 8 DIVISION I CONSENSUS ALL-AMERICA SELECTIONS Division I Consensus All-America Selections Second Tea m —R o b e r t Doll, Colorado; Wil f re d Un r uh, Bradley, 6-4, Toulon, Ill.; Bill Sharman, Southern By Season Do e rn e r , Evansville; Donald Burness, Stanford; George Ca l i f o r nia, 6-2, Porte r ville, Calif. Mu n r oe, Dartmouth; Stan Modzelewski, Rhode Island; Second Tea m —Charles Cooper, Duquesne; Don 192 9 John Mandic, Oregon St. Lofgran, San Francisco; Kevin O’Shea, Notre Dame; Don Charley Hyatt, Pittsburgh; Joe Schaaf, Pennsylvania; Rehfeldt, Wisconsin; Sherman White, Long Island. Charles Murphy, Purdue; Ver n Corbin, California; Thomas 1943 Ch u r chill, Oklahoma; John Thompson, Montana St. First Te a m— A n d rew Phillip, Illinois; Georg e 1951 193 0 Se n e s k y , St. Joseph’s; Ken Sailors, Wyoming; Harry Boy- First Tea m —Bill Mlkvy, Temple, 6-4, Palmerton, Pa.; ko f f, St. -
1980-89 NBA Finals
NBA FINALS 198 0 - 1 9 8 9 Detroit Pistons sweep Los Angeles Lakers 1 63-19 1E under Chuck Daly 57-25 1W under Pat Riley June 6, 8, 11, 13 9 Joe Dumars DET Finals MVP 27.3 pts, 6.0 ast, 1.8 reb 8 Pistons win their first-ever NBA championship 9 During season, Pat Riley trademarked phrase “Three-peat” Lakers 97 @ Pistons 109 at The Palace of Auburn Hills – Isiah Thomas DET 24 pts, 9 ast; Joe Dumars DET 22 pts Lakers 105 @ Pistons 108 – Joe Dumars DET 33 pts; Magic Johnson LAL injures hamstring, plays only 5 more mins in series Pistons 114 @ Lakers 110 at Great Western Forum – Joe Dumars DET 31 pts; Dennis Rodman DET 19 reb Pistons 105 @ Lakers 97 – Joe Dumars DET 23 pts; James Worthy LAL 40 pts Pistons’ starters – G Isiah Thomas, G Joe Dumars, C Bill Laimbeer, F Mark Aguirre, F Rick Mahorn Lakers’ starters – G Magic Johnson, G Michael Cooper, C Kareem Abdul-Jabbar, F A.C. Green, F James Worthy 1 Los Angeles Lakers defeat Detroit Pistons in 7 9 62-20 1W under Pat Riley 54-28 2E under Chuck Daly June 7, 9, 12, 14, 16, 19, 21 8 James Worthy LAL Finals MVP 22.0 pts, 4.4 ast, 7.4 reb 8 Pistons 105 @ Lakers 93 at Great Western Forum – Adrian Dantley DET 34 pts; Isiah Thomas DET 19 pts, 12 ast Pistons 96 @ Lakers 108 – James Worthy LAL 26 pts, 10 reb, 6 ast; Byron Scott LAL 24 pts; Magic Johnson LAL 11 ast Lakers 99 @ Pistons 86 at Pontiac Silverdome – James Worthy LAL 24 pts; Magic Johnson LAL 18 pts, 14 ast Lakers 86 @ Pistons 111 – Adrian Dantley DET 27 pts; Isiah Thomas DET 9 rb, 12 as; Vinnie Johnson DET 16 pts off bench Lakers 94 @ Pistons 104 – Adrian Dantley DET 25 pts; Bill Laimbeer DET 11 reb; John Salley DET 10 reb Pistons 102 @ Lakers 103 – James Worthy LAL 28 pts; Magic Johnson LAL 19 pts, 22 ast Pistons 105 @ Lakers 108 – James Worthy LAL 36 pts, 16 reb, 10 ast; Magic Johnson LAL 19 pts, 14 ast Lakers’ starters – G Magic Johnson, G Byron Scott, C Kareem Abdul-Jabbar, F A.C. -

Weber State Men's Basketball 50Th Anniversary Team
WEBER STATE MEN’S BASKETBALL 50TH ANNIVERSARY TEAM Player Years played Lance Allred 2003-05 Harold Arceneaux 1998-00 Nolan Archibald 1966-68 Scott Bamforth 2010-13 Jermaine Boyette 2000-03 Alan Campbell 1984-86 Shawn Campbell 1983-85 Bruce Collins 1976-80 Richard Cooper 1970-73 Ryan Cuff 1995-97 Bob Davis 1970-72 Jimmy Degraffenried 1990-96 Al DeWitt 1972-76 Royal Edwards 1979-83 Alex Fisher 1995-98 Eddie Gill 1998-00 Al Hamilton 1990-93 John Hamilton 2000-04 Sessions Harlan 1968-70 Todd Harper 1978-82 Greg Harrop 1964-67 David Johnson 1976-80 Robbie Johnson 1991-94 Jonnie Knoble 1969-72 Damian Lillard 2008-12 Jim Lyon 1962-64 Mark Mattos 1976-80 Stan Mayhew 1976-77 Kellen McCoy 2007-09 Ruben Nembhard 1993-95 Slobodan Ockoljic 2002-04 David Patten 2004-07 John Price 1982-84 Stan Rose 1992-93 Mike Sivulich 1962-64 Brady Small 1970-73 Kirk Smith 1993-95 Richard Smith 1976-80 Willie Sojourner 1968-71 Dan Sparks 1966-68 Nic Sparrow 1997-04 Justus Thigpen 1967-69 Eddie Tillman 1964-66 Jerry Trice 1963-66 Walt Tyler 1985-87 Gene Visscher 1964-66 Rico Washington 1987-89 Jimmie Watts 1972-76 Harry Willis 1985-87 Randy Worster 1982-85 WEBER STATE MEN’S BASKETBALL 50TH ANNIVERSARY TEAM LANCE ALLRED • Played two seasons from 2003-05. • Earned First Team All-Big Sky honors as a senior in 2004-05. • Ranks 25th in school history in career scoring. • Ranks eighth in WSU history in career rebounding average at 9.1 per game.