Bacterial Transfer from Mouth to Different Utensils and from Utensils to Food Chaitali Purohit Clemson University, [email protected]
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Slow Cooking Free Download
SLOW COOKING FREE DOWNLOAD The Australian Women's Weekly | 192 pages | 02 Jul 2011 | Australian Consolidated Press UK | 9781907428234 | English | Northampton, United Kingdom New York Times bestselling author & Slow Living Expert Slow Roast Lamb Prep Time. The long, moist cooking is particularly suitable for tough and cheap cuts of meat including pork shoulderbeef chuck and brisket. By Janiece Mason. To Slow Cooking a slow cooker, the cook places raw food and a liquid, such as Slow Cookingwater, or wine, in the slow cooker. Alexandra Folino. These are the best I've had, short of the actual grilling method of course! Advertisement - Continue Reading Below. Slow Cooking temperature of the contents rises until it reaches boiling point, at which point the energy goes into gently boiling the liquid closest to the hot surface. By Chandrav. By Buckwheat Queen. It will take a bit longer for the dish inside to get up to temperature, but your food will cook just fine. Slow-Cooker Paella. List of cooking appliances List of cooking vessels Outdoor cooking Food preparation Food preservation Food safety. The cooker was then reintroduced under the name "Crock-Pot" Slow Cooking Skip Slow Cooking Skip to content Skip to primary sidebar Skip to secondary sidebar. Mississippi pot roast is a perfect dish perfect Slow Cooking the Slow Cooker. The affordable crock pots can do everything — if Slow Cooking really wanted, you could make breakfast, lunch, dinner, and dessert in these things. This recipe is so simple, you will love it! You'll love 'em on busy weeknights The contents Slow Cooking enclosed by the crock and the lid, and attain an essentially constant temperature. -

Chopsticks Is a Divine Art of Chinese Culture
INTERNATIONAL JOURNAL OF RESEARCH CULTURE SOCIETY ISSN: 2456-6683 Volume - 2, Issue - 11, Nov – 2018 Monthly, Peer-Reviewed, Refereed, Indexed Journal Impact Factor: 4.526 Publication Date: 30/11/2018 Chopsticks is a Divine Art of Chinese Culture Md. Abu Naim Shorkar School of Economics, Shanghai University, 99, Shangda Road, Shanghai, China, 200444, Email – [email protected] Abstract: Chopsticks are the primary eating instrument in Chinese culture, and every youngster has to adopt using technique and controlling of chopsticks. A couple of chopsticks is the main instrument for eating, and the physical movements of control are familiar with Chinese. The Chinese use chopsticks as natural as Caucasians use knives and forks. An analogy of chopsticks is as an extension of one’s fingers. Chinese food is prepared so that it may be easily handled with chopsticks. In fact, many traditional Chinese families do not have forks at home. The usage of chopsticks has been deeply mixed into Chinese culture. In any occasions, food has become a cultural show in today’s society. When food from single nation becomes in another, it leads to a sort of cultural interchange. China delivers a deep tradition of food culture which has spread around the globe. As a company rises, food culture too evolves resulting in mutations. Each geographical location makes its own food with unparalleled taste and smell. Sullen, sweet, bitter and hot are the preferences of several food items. Apart from being good, they tell us about the people who make it, their culture and nation. The creatures which people apply to eat are not only creatures, but also symbols, relics of that civilization. -

Korean Food and American Food by Yangsook
Ahn 1 Yangsook Ahn Instructor’s Name ENGL 1013 Date Korean Food and American Food Food is a part of every country’s culture. For example, people in both Korea and America cook and serve traditional foods on their national holidays. Koreans eat ddukguk, rice cake soup, on New Year’s Day to celebrate the beginning of a new year. Americans eat turkey on Thanksgiving Day. Although observing national holidays is a similarity between their food cultures, Korean food culture differs from American food culture in terms of utensils and appliances, ingredients and cooking methods, and serving and dining manners. The first difference is in utensils and appliances. Koreans’ eating utensils are a spoon and chopsticks. Koreans mainly use chopsticks and ladles to cook side dishes and soups; also, scissors are used to cut meats and other vegetables, like kimchi. Korean food is based on rice; therefore, a rice cooker is an important appliance. Another important appliance in Korean food culture is a kimchi refrigerator. Koreans eat many fermented foods, like kimchi, soybean paste, and red chili paste. For this reason, almost every Korean household has a kimchi refrigerator, which is designed specifically to meet the storage requirements of kimchi and facilitate different fermentation processes. While Koreans use a spoon and chopsticks, Americans use a fork and a knife as main eating utensils. Americans use various cooking utensils like a spatula, tongs, spoon, whisk, peeler, and measuring cups. In addition, the main appliance for American food is an oven since American food is based on bread. A fryer, toaster, and blender are also important equipment to Ahn 2 prepare American foods. -
2013.01-06 New Korin Items
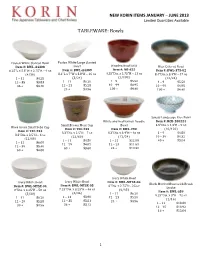
NEW$KORIN$ITEMS$JANUARY$–$JUNE$2013$ Limited'Quantities'Available' ' TABLEWARE:"Bowls" " " " Fusion"White"Slanted"Bowl" Fusion"White"Large"Slanted" " " Item%#:%BWL+A4308% Bowl" Wooden"Bowl"RED" Blue"Colored"Bowl" 6.25"L"x"5.5"W"x"2.75"H"–"9"oz" Item%#:%BWL+A4309% Item%#:%NR+625% Item%#:%BWL+375+02% (4/36)" 8.1”L"x"7”W"x"3.8"H"–"16"oz" 4.25"Dia."x"2.75"H"–"11"oz" 8.4"Dia."x"3.4"H"–"47"oz" 1"–"11" $4.25" (3/24)" (1/100)" (12/24)" 12"–"35" $3.83" 1"–"11" $6.20" 1"–"9" $5.50" 1"–"9" $5.50" 36"+" $3.40" 12"–"23" $5.58" 10"–"99" $4.95" 10"–"99" $4.95" " " 24"+" $4.96" 100"+" $4.40" 100"+" $4.40" " " " " " " " " " " " " Sansui"Landscape"Rice"Bowl" " White"and"Red"Ramen"Noodle" Item%#:%RCB+200224% " Small"Brown"Moss"Cup" Bowl" 4.5"Dia."x"1.3"H"–"9"oz" Hiwa"Green"Small"Soba"Cup" Item%#:%TEC+233% Item%#:%BWL+290% (10/120)" Item%#:%TEC+234% 3.3”Dia."x"2.5"H"–"7"oz" 8.3”Dia."x"3.4"H"–"46"oz" 1"–"9" $4.80" 3.3”Dia."x"2.5"H"–"6"oz" (12/60)" (12/24)" 10"–"39" $4.32" (12/60)" 1"–"11" $4.50" 1"–"11" $12.90" 40"+" $3.84" 1"–"11" $6.00" " " 12"–"59" $4.05" 12"–"23" $11.61" " 12"–"59" $5.40" 60"+" $3.60" 24"+" $10.32" 60"+" $4.80" " " " " " " Ivory"White"Bowl" Ivory"White"Bowl" Item%#:%BWL+MTSX+06% " Ivory"White"Bowl" Black"Mottled"Bowl"with"Brush" Item%#:%BWL+MTSX+05% 6"Dia."x"2.75"H"\"25"oz" Item%#:%BWL+MTSX+04% Stroke" 7.25"Dia."x"3.25"H"–"46"oz" (6/48)" 8"Dia."x"3.25"H"–"58"oz" Item%#:%BWL+S59% (6/36)" 1"–"11" $6.20" (5/30)" 9.25"Dia."x"3"H"–"72"oz" 1"–"11" $3.90" 12"–"23" $5.58" 1"–"11" $6.20" (1/16)" 12"–"35" $3.51" 24"+" $4.96" 12"–"29" $5.58" 1"–"11" -

Chopsticks and the Land of the Five Flavors
History in the Making Volume 9 Article 14 January 2016 Comparative Book Review: Chopsticks and The Land of the Five Flavors Jacob P, Banda CSUSB Follow this and additional works at: https://scholarworks.lib.csusb.edu/history-in-the-making Part of the Asian History Commons, and the Social History Commons Recommended Citation Banda, Jacob P, (2016) "Comparative Book Review: Chopsticks and The Land of the Five Flavors," History in the Making: Vol. 9 , Article 14. Available at: https://scholarworks.lib.csusb.edu/history-in-the-making/vol9/iss1/14 This Review is brought to you for free and open access by the History at CSUSB ScholarWorks. It has been accepted for inclusion in History in the Making by an authorized editor of CSUSB ScholarWorks. For more information, please contact [email protected]. Reviews Comparative Book Review: Chopsticks and The Land of the Five Flavors By Jacob P. Banda Food and foodways provide a valuable window into Chinese history and culture. Scholars have, until recently, not sufficiently explored them as great potential frameworks for analyzing Chinese history. They are rich potential sources of insights on a wide range of important themes that are crucial to the understanding of Chinese society, both past and present. Historians have tended to favor written sources and particularly those of social and political elites, often at the expense of studying important cultural practices and the history of daily life. The creative use of unconventional sources can reward the scholar with a richer view of daily life, with food and foodways as one of the most important dimensions. -

Chopsticks: a Chinese Invention 507 Sopris West Six Minute Solutions Passage
Curriculum-Based Measurement: Maze Passage: Examiner Copy Student/Classroom: _____________________ Examiner: ____________ Assessment Date: _______ Chopsticks: A Chinese Invention 507 Sopris West Six Minute Solutions Passage Chopsticks were invented in China more than 5,000 years ago. Long ago, food was chopped into (little) pieces so it would cook faster. (The) faster food cooked, the more fuel (it) would save. Since food was eaten (in) small pieces, there was no need (for) knives. Rather, chopsticks were used to (move) food from the plate to the (mouth). Confucius was a Chinese philosopher. He (was) a vegetarian. It is believed that (Confucius) did not like knives. Knives reminded (him) of the slaughterhouse. He favored chopsticks. (By) A.D.500, the use of chopsticks (had) spread to other countries. The people (in) present day Vietnam, Korea, and Japan, (as) well as China, use chopsticks today. (Chinese) chopsticks are about 9 or 10 inches long. (They) are square at the top, have (a) blunt end, and are thinner on (the) bottom. The Chinese call them kuai-ai. (This) means "quick little fellows." Chopsticks have (been) made of many materials. Bamboo is (a) popular choice since it is available, (and) inexpensive. Bamboo is also heat resistant. (Other) types of wood such as sandalwood, (cedar), and teak have also been used. (Long) ago, rich people had chopsticks made (from) jade, gold, or silver. In the (days) of the Chinese dynasty, silver chopsticks (were) used. People believed that silver would (turn) black if it touched poisoned food. (We) know now that silver will not (react) to poison. -

Okonomiyaki by Chef Philli
Okonomiyaki By Chef Philli Serves Prep time Cook time Total time 2-3 20 mins 20 mins 40 mins Chef Skills: Learn how to make Japan’s answer to a pizza Ingredients Equipment ● ½ tsp salt ● Pallet knife ● ½ tsp white sugar ● Baking parchment ● 80g plain flour ● Pizza tray or large tray ● 1 tsp bicarbonate of soda ● Mandoline ● 80ml water ● Whisk or chopsticks ● 2 eggs - lightly whisked ● Piping bag ● 2 handfuls spring onions - thinly ● Large frying pan with lid sliced ● 1 small white cabbage - thinly sliced ● 30g pink pickled ginger Before you click play ● 1 tsp rice wine vinegar ● Get out all equipment & ● 4-6 rashers of streaky bacon measure ingredients ● Handful of furikake (see ● Slice cabbage and spring onions furikake episode) as described ● Mayonnaise ● Make the takoyaki sauce by Ingredients for takoyaki sauce combining all ingredients ● 1 tbsp ketchup ● 1 tbsp oyster sauce ● 1 tsp worcestershire sauce ● 1 tbsp brown sugar 1 of 3 - Next Okonomiyaki By Chef Philli Method 1. To make the batter add the plain flour, sugar, a pinch of salt and baking soda in large mixing bowl. Mix the ingredients with a whisk or a pair of chopsticks. 2. Add the water and the eggs and whisk to incorporate all the ingredients. 3. Add the cabbage, spring onions and the pickled ginger. Mix together, ensuring that the cabbage is fully coated with the batter. 4. Cut two round pieces of baking paper and place one into your frying pan - this is your cartouche - save the other for later. 5. Add rice wine vinegar and place into the mixing bowl with the okonomiyaki batter. -

Silent Auction Items (As of 3/13/17) Art & Home
Silent Auction Items (as of 3/13/17) Art & Home Item # Description Value Donor 100 Red & Black Crocheted Heart Blanket $65 Kathy Peterson 101 102 4 Homemade Soy Jar Candles $30 Rebecca Stearns - RMS Candle Co. 103/104 Asian Placemats w/ Chopsticks- 2 offers $25 Jason Lee & Sharon Wilmans 105 Beautiful Korean Lacquer Ware Tray w/ Mother of $75 Jason Lee Family Pearl Inlay 106 Beautiful Korean Lacquer Ware w/ Mother of Pearl $75 Jason Lee Family Inlay 107 108 Felt Basket w/ Penguin and Bird Ornaments, VT Towel $75 PURE Original & VT Bracelet 109 Pledge of Allegiance Wall Hanging $15 Judy Weisgerber- Hobby Lobby 110 Handmade Blue & Gray 4ft x 5 ft Crocheted Afghan $50 Ethel Fennick (Judy’s mom) 111 Handmade Blue, Brown & Beige 3ft x 7 ft Crocheted $50 Ethel Fennick Afghan 112 Mikasa Glass Candy Dish Adrianne Weisgerber 113 RedKen Products $88 Heidi Senecal- Artistic Styles 114 Framed Oil Painting - Valley View $250 Steve & Ruth Hall 115 “A Friend Loves At All Times” Proverbs 17:17 Mug w/ $12 Judy Weisgerber Attached Tea Bag Holder 116 2 “Live Well, Laugh Often, Love Much” Flower Vases $25 Jennifer Brooks w/ 2 Cherubs 117 Large Canvas Picture - “Bicycle w/ Basket of Flowers” $35 The Burchfield’s 118/119 1 Liter of Maple Syrup - 2 offers $25 Severy Brothers - Severy Family Maple 120 6 Stuart Crystal Hand Cut Goblets $50 The Deibler’s 121 “Joy of a Summer Garden” Table Runner - $125 Susan Hansen One-of-a-kind hand sewn wool primitive table runner collaboratively designed by RACS student Rosie Nop. -

Chopsticks As a Cultural Symbol in China
IOSR Journal of Research & Method in Education (IOSR-JRME) e-ISSN: 2320–7388,p-ISSN: 2320–737X Volume 1, Issue 4 (May. –Jun. 2013), PP 01-02 www.iosrjournals.org Chopsticks as a Cultural Symbol in China Chen Desheng & Tang Zheng Ph.D. Scholar,Department of English and Foreign Languages,Bharathiar University,Coimbatore-641046 II M.A English literature, Department of English, R.V.S College of Arts & Science, Coimbatore-641402 Abstract: Food is the soul of health. On such occasions as birthday, food becomes a cultural show in today’s society. When food from one country becomes in another, it leads a kind of cultural exchange. China has a rich tradition of food culture which has spread around the world. As a society develops, food culture too evolves resulting in variety. Each geographical location makes its own food with unique taste and flavor. Sour, sweet, bitter and hot are the tastes of various food items. Apart from being food, they tell us about the people who make it, their culture and nation. The tools which people use to eat are not only tools, but also symbols, tokens of that culture. The practice of using chopsticks has existed from ancient times among the East Asians, especially the Chinese. Made of different materials like gold, silver, copper, wood and bamboo, the chopsticks also express the artistic and aesthetic sensibility of the Chinese people. History tells us that the different colors, sizes and materials of chopsticks have specific meanings. They may stand for position, treasure, luck and so on. This paper attempts to study the importance of chopsticks as a dominant cultural symbol in China. -
Skill-A-Thon Booklet
Foods And Cooking id 1 Apple Corer — This tool has a circular cutting edge that is forced down into the Apple Slicer — This apple, allowing the apple to remain whole so professional-quality tool is it can then be easily sliced into sections for pressed down over the apple to eating it out of hand or baking it whole with make eight uniform slices and the outer skin. A tool used to extract the core remove the core. from the apple without cutting the apple into sections and then individually cutting out each part of the core. Chef’s Knife — A large knife with a wide blade, generally BBQ Tongs — A utensil with considered all-purpose knives long handles used to grip and that are used for cutting and turn food while cooking. dicing. BBQ Spatula — A utensil with long handle and flat bottom used to turn food while cooking. Chopper — A utensil used to cut food into smaller pieces. 2 Chopsticks — A pair of slender sticks made especially of wood or ivory, held between the thumb and fingers and used as an eating utensil in Asian countries and in Cookie Cutter — A shaped template restaurants serving Asian food. with a sharp edge used to cut cookies or biscuits from rolled dough Decorative Slicer, Ripple — A utensil Decorative Slicer, Vee — A utensil used used to cut food that leaves a rippled edge. to cut food that leaves a vee shape Egg Slicer — A kitchen tool with a Egg Separator — A spoon shaped utensil, slatted , egg-shaped hollow on the bottom which has a hole in the bottom and is used and a hinged top consisting of 10 fine steel to separate the white from the yolk of the wires. -

Learn to Use Chopsticks はし
THE JAPANESE HOUSE KYO NO MACHIYA はし ACTIVITIES Learn to Use Chopsticks ACTIVITIES Learn chopsticks culture and etiquette in Japan and try it yourself! TIME: 25 minutes MATERIALS: • Video: Many Homes in Kyoto, Japan—Shiori • A pair of chopsticks • Small items to pick up 1. Learn about Hashi—Chopsticks Chopsticks in Japanese are called hashi; o-hashi is the more polite way to PRONUNCIATION say it. They are made from a variety of materials: wood (including GUIDE: lacquered wood), bamboo, metals, and plastics, but wooden chopsticks Hashi: Hah-she are the most common. There are different kinds of chopsticks for different uses: for eating, for cooking, and for picking up or serving cakes O-hashi: oh hah-she and sweets. Mai-hashi: mah-ee hah- At home, each person has his or her own pair of chopsticks for daily she use. Many people also have a second pair of chopsticks called mai-hashi (my chopsticks) that they would carry with them all the time for use at work or at restaurants. Even though disposable wooden chopsticks are still commonly used at fast food stores and restaurants, people like to have their mai-hashi because it minimizes waste and is better for the environment. Children in Japan usually start learning to use chopsticks by the age of 4 or 5. There are various training chopsticks available for beginner users. 1 © 2013 Boston Children’s Museum KYO NO MACHIYA ACTIVITIES 2. How to Hold a Pair of Hashi Before you start—Watch the chapter “Shiori” in the video: “Many Homes in Kyoto, Japan.” Shiori and her mom prepare hamburger and eat it with rice. -

Cookware | Kitchenware | Houseware | Utensils Cookware Sets 546 8 Piece Tri-Ply Copper Cookware Set
2017 CATALOG COOKWARE | KITCHENWARE | HOUSEWARE | UTENSILS COOKWARE SETS 546 8 PIECE TRI-PLY COPPER COOKWARE SET < SET INCLUDES 1.5 Qt Covered Sauce Pan 3.25 Qt Covered Sauce Pan 5.5 Qt Covered Dutch Oven 9.5” Covered Fry Pan This tri-ply set consists of the basics every kitchen needs and in a tasteful copper mirror-polished finish. Long riveted stainless steel cast handles for effortless handling as you work and tempered vented glass lids allow visual monitoring of your food as it cooks. Elegant and modern, this is a high quality cookware set for the professional chef at home. 506 7 PIECE TRI-PLY COOKWARE SET < SET INCLUDES 1 Qt Covered Saucepan 2 Qt Covered Saucepan 5.5 Qt Covered Dutch Oven 10” Open Frypan (Dutch oven lid fits frypan) This 7 piece professional quality tri-ply 18/10 stainless steel cookware set provides superior heat distribution. Features stay cool cast knobs and handles with glass lids to allow you to monitor your cooking. Induction stovetop ready. 01 2017 COOK PRO CATALOG 503 7 PIECE STAINLESS STEEL COOKWARE SET W/ ENCAPSULATED BASE SET INCLUDES > 1 Qt Covered Sauce Pan 2 Qt Covered Sauce Pan 5 Qt Covered Dutch Oven 9.5" Open Frypan (Dutch oven lid fits frypan) This 7 piece 18/10 stainless steel cookware set includes an encapsulated base for even heat distribution. Stay cool hollow handles and knobs allow easier handling. Features two tone polished exterior and satin finished interior. Induction stovetop ready. 500 7 PIECE STAINLESS STEEL COOKWARE SET W/ ENCAPSULATED BASE SET INCLUDES > 1 Qt Covered Sauce Pan 2 Qt Covered Sauce Pan 5 Qt Covered Dutch Oven 9.5" Open Frypan (Dutch oven lid fits frypan) This 7 piece stainless steel cookware set features an encapsulated base for even heat distribution.