Comparator Report on Patient Access to Cancer Medicines in Europe Revisited
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Investigator Initiated Study IRB-29839 an Open-Label Pilot Study To
Investigator Initiated Study IRB-29839 An open-label pilot study to evaluate the efficacy and safety of a combination treatment of Sonidegib and BKM120 for the treatment of advanced basal cell carcinomas Version 05 September 2016 NCT02303041 DATE: 12Dec2018 1 Coordinating Center Stanford Cancer Center 875 Blake Wilbur Drive Stanford, CA 94305 And 450 Broadway, MC 5334 Redwood City, CA 94603 Protocol Director and Principal Investigator Anne Lynn S Chang, MD, Director of Dermatological Clinical Trials 450 Broadway St, MC 5334 Redwood City, CA 94603 [email protected] Co-Investigator Anthony Oro, MD PhD 450 Broadway St, MC 5334 Redwood City, CA 94603 [email protected] Biostatistician Shufeng Li, MS 450 Broadway St, MC 5334 Redwood City, CA 94603 [email protected] Study Coordinator Ann Moffat 450 Broadway St, MC 5334 Redwood City, CA 94603 [email protected] 2 Table of Contents 1 Background ................................................................. 7 1.1 Disease Background ..................................................... 7 1.2 Hedgehog Pathway and mechanism of action ............................... 7 1.3 PI3K Pathway and mechanism of action ................................... 9 1.4 Sonidegib Compound Information ............ Error! Bookmark not defined. 1.4.1 Preclinical Studies for Sonidegib ....................................................................11 1.4.2 Muscular system...............................................................................................13 1.4.3 Skeletal system ................................................................................................13 -

And High-Dose Cyclophosphamide
141-146 6/6/06 13:01 Page 141 ONCOLOGY REPORTS 16: 141-146, 2006 141 Different mechanisms for anti-tumor effects of low- and high-dose cyclophosphamide YASUHIDE MOTOYOSHI1,2, KAZUHISA KAMINODA1,3, OHKI SAITOH1, KEISUKE HAMASAKI2, KAZUHIKO NAKAO3, NOBUKO ISHII3, YUJI NAGAYAMA1 and KATSUMI EGUCHI2 Departments of 1Medical Gene Technology, Atomic Bomb Disease Institute; 2Division of Immunology, Endocrinology and Metabolism, Department of Medical and Dental Sciences, and 3Division of Clinical Pharmaceutics and Health Research Center, Nagasaki University Graduate School of Biomedical Sciences, 1-12-4 Sakamoto, Nagasaki 852-8501, Japan Received February 3, 2006; Accepted April 7, 2006 Abstract. It is known that, besides its direct cytotoxic effect appear to be highly crucial in a clinical setting of combined as an alkylating chemotherapeutic agent, cyclophosphamide chemotherapy and immunotherapy for cancer treatment. also has immuno-modulatory effects, such as depletion of CD4+CD25+ regulatory T cells. However, its optimal concen- Introduction tration has not yet been fully elucidated. Therefore, we first compared the effects of different doses of cyclophosphamide Chemotherapy and immunotherapy are generally regarded on T cell subsets including CD4+CD25+ T cells in mice. as unrelated or even mutually exclusive in cancer treatment, Cyclophosphamide (20 mg/kg) decreased the numbers of because chemotherapy kills not only target cancer cells but splenocytes, CD4+ and CD8+ T cells by ~50%, while a decline also immune cells, inducing systemic immune suppression in CD4+CD25+ T cell number was more profound, leading to and dampening the therapeutic efficacy of immunotherapy. the remarkably lower ratios of CD4+CD25+ T cells to CD4+ In this regard, however, cyclophosphamide appears an T cells. -

Intratumoral Immunotherapy for Early Stage Solid Tumors
Author Manuscript Published OnlineFirst on February 18, 2020; DOI: 10.1158/1078-0432.CCR-19-3642 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. 1 Intratumoral immunotherapy for early-stage solid tumors 2 3 Wan Xing Hong1,2*, Sarah Haebe2,3*, Andrew S. Lee4,5, C. Benedikt Westphalen3,6,7, 4 Jeffrey A. Norton1,2, Wen Jiang8, Ronald Levy2# 5 6 1. Department of Surgery, Stanford University School of Medicine 7 2. Stanford Cancer Institute, Division of Oncology, Department of Medicine, Stanford University 8 3. Department of Medicine III, University Hospital, LMU Munich, Germany 9 4. Department of Pathology, Stanford University School of Medicine 10 5. Shenzhen Bay Labs, Cancer Research Institute, Shenzhen, China 11 6. Comprehensive Cancer Center Munich, Munich, Germany 12 7. Deutsches Konsortium für Translationale Krebsforschung (DKTK), DKTK Partner Site Munich, 13 Germany 14 8. Department of Radiation Oncology, The University of Texas Southwestern Medical Center, Dallas, 15 Texas, USA 16 * These authors contributed equally to this work 17 # Correspondence: [email protected]. 18 CCSR 1105, Stanford, California 94305-5151 19 (650) 725-6452 (office) 20 21 Running title: Intratumoral immunotherapy for early-stage solid tumors 22 23 24 Conflict of Interest 25 Dr. Ronald Levy serves on the advisory boards for Five Prime, Corvus, Quadriga, BeiGene, GigaGen, 26 Teneobio, Sutro, Checkmate, Nurix, Dragonfly, Abpro, Apexigen, Spotlight, 47 Inc, XCella, 27 Immunocore, Walking Fish. 28 Dr. Benedikt Westphalen is on the advisory boards for Celgene, Shire/Baxalta Rafael Pharmaceuticals, 29 Redhill and Roche. He receives research support from Roche. -

AN ANTICANCER DRUG COCKTAIL of Three Kinase Inhibitors Improved Response to a DENDRITIC CELL–BASED CANCER VACCINE
Author Manuscript Published OnlineFirst on July 2, 2019; DOI: 10.1158/2326-6066.CIR-18-0684 Author manuscripts have been peer reviewed and accepted for publication but have not yet been edited. 1 AN ANTICANCER DRUG COCKTAIL OF Three Kinase Inhibitors Improved Response to a DENDRITIC CELL–BASED CANCER VACCINE Jitao Guo1, Elena Muse1, Allison J. Christians1, Steven J. Swanson2, and Eduardo Davila1, 3, 4 1Division of Medical Oncology, Department of Medicine, University of Colorado, Anschutz Medical Campus, Aurora, Colorado, United States; 2Immunocellular Therapeutics Ltd., Westlake Village, California, United States; 3 Human Immunology and Immunotherapy Initiative, University of Colorado, Anschutz Medical Campus, Aurora, Colorado, United States; and 4University of Colorado Comprehensive Cancer Center, Aurora, Colorado, United States. Running Title: REPURPOSING ANTICANCER DRUGS FOR DC CANCER VACCINE Keywords: Dendritic cell; cancer vaccine; MK2206; NU7441; Trametinib Financial supports: This work was supported by R01CA207913, a research award from ImmunoCellular Therapeutics, VA Merit Award BX002142, University of Maryland School of Medicine Marlene and Stewart Greenebaum Comprehensive Cancer Center P30CA134274 and the University of Colorado Denver Comprehensive Cancer Center P30CA046934. Corresponding author: Dr. Eduardo Davila Mail stop 8117,12801 E. 17th Avenue, Aurora, CO 80045 Email: [email protected] Phone: (303) 724-0817; Fax:(303) 724-3889 Conflict of Interest Disclosures: These studies were partly funded by a grant from ImmunoCellular Therapeutics (IMUC). S.S. currently serves as SVP Research IMUC but the remaining authors declare no competing financial interests. Counts: Abstract, 242 words; Manuscript, 4523 words; Figures, 5; References,50. Downloaded from cancerimmunolres.aacrjournals.org on October 2, 2021. © 2019 American Association for Cancer Research. -

07052020 MR ASCO20 Curtain Raiser
Media Release New data at the ASCO20 Virtual Scientific Program reflects Roche’s commitment to accelerating progress in cancer care First clinical data from tiragolumab, Roche’s novel anti-TIGIT cancer immunotherapy, in combination with Tecentriq® (atezolizumab) in patients with PD-L1-positive metastatic non- small cell lung cancer (NSCLC) Updated overall survival data for Alecensa® (alectinib), in people living with anaplastic lymphoma kinase (ALK)-positive metastatic NSCLC Key highlights to be shared on Roche’s ASCO virtual newsroom, 29 May 2020, 08:00 CEST Basel, 7 May 2020 - Roche (SIX: RO, ROG; OTCQX: RHHBY) today announced that new data from clinical trials of 19 approved and investigational medicines across 21 cancer types, will be presented at the ASCO20 Virtual Scientific Program organised by the American Society of Clinical Oncology (ASCO), which will be held 29-31 May, 2020. A total of 120 abstracts that include a Roche medicine will be presented at this year's meeting. "At ASCO, we will present new data from many investigational and approved medicines across our broad oncology portfolio," said Levi Garraway, M.D., Ph.D., Roche's Chief Medical Officer and Head of Global Product Development. “These efforts exemplify our long-standing commitment to improving outcomes for people with cancer, even during these unprecedented times. By integrating our medicines and diagnostics together with advanced insights and novel platforms, Roche is uniquely positioned to deliver the healthcare solutions of the future." Together with its partners, Roche is pioneering a comprehensive approach to cancer care, combining new diagnostics and treatments with innovative, integrated data and access solutions for approved medicines that will both personalise and transform the outcomes of people affected by this deadly disease. -
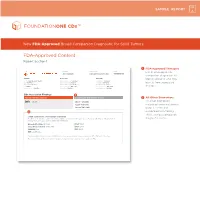
FDA-Approved Content Report Section 1
SAMPLE REPORT New FDA-Approved Broad Companion Diagnostic for Solid Tumors FDA-Approved Content Report Section 1 1 FDA-Approved Therapies PATIENT TUMOR TYPE TRF# List of FDA-approved Jane Sample Lung adenocarcinoma TRFXXXXXX companion diagnostics to PATIENT PHYSICIAN SPECIMEN identify patients who may DISEASE Lung adenocarcinoma ORDERING PHYSICIAN Not Given SPECIMEN SITE Not Given NAME Not Given MEDICAL FACILITY Not Given SPECIMEN ID Not Given benefi t from associated DATE OF BIRTH Not Given ADDITIONAL RECIPIENT Not Given SPECIMEN TYPE Not Given SEX Female MEDICAL FACILITY ID Not Given DATE OF COLLECTION Not Given therapies MEDICAL RECORD # Not Given PATHOLOGIST Not Given SPECIMEN RECEIVED Not Given CDx Associated Findings 1 GENOMIC FINDINGS DETECTED FDA-APPROVED THERAPEUTIC OPTIONS 2 All Other Biomarkers EGFR L858R Gilotrif® (Afatinib) All other biomarkers, Iressa® (Gefitinib) including tumor mutational Tarceva® (Erlotinib) burden (TMB) and 2 microsatellite instability (MSI), without companion OTHER ALTERATIONS & BIOMARKERS IDENTIFIED Results reported in this section are not prescriptive or conclusive for labeled use of any specific therapeutic product. See diagnostic claims professional services section for additional information. Microsatellite Status MS-Stable PTCH1 T416S Tumor Mutation Burden 11 Muts/Mb RBM10 Q494* CDKN2A/B loss TP53 R267P EGFR amplification § Refer to appendix for limitation statements related to detection of any copy number alterations, gene rearrangements, MSI or TMB result in this section. Please refer to appendix -

Rheumatic Immune-Related Adverse Events—A Consequence of Immune Checkpoint Inhibitor Therapy
biology Review Rheumatic Immune-Related Adverse Events—A Consequence of Immune Checkpoint Inhibitor Therapy Anca Bobircă 1,†, Florin Bobircă 2,†, Ioan Ancuta 1,†, Alesandra Florescu 3, Vlad Pădureanu 4,* , 5, 6, 7 8 Dan Nicolae Florescu *, Rodica Pădureanu * , Anca Florescu and Anca Emanuela Mus, etescu 1 Department of Internal Medicine and Rheumatology, Carol Davila University of Medicine and Pharmacy, 050474 Bucharest, Romania; [email protected] (A.B.); [email protected] (I.A.) 2 Department of General Surgery, Carol Davila University of Medicine and Pharmacy, 050474 Bucharest, Romania; fl[email protected] 3 Department of Rheumatology, Emergency Clinical County Hospital of Craiova, 200642 Craiova, Romania; [email protected] 4 Department of Internal Medicine, University of Medicine and Pharmacy of Craiova, 200349 Craiova, Romania 5 Department of Gastroenterology, University of Medicine and Pharmacy of Craiova, 200349 Craiova, Romania 6 Department of Internal Medicine, Emergency Clinical County Hospital of Craiova, 200642 Craiova, Romania 7 Department of Internal Medicine and Rheumatology, Dr. I Cantacuzino Hospital, 030167 Bucharest, Romania; anca-teodora.fl[email protected] 8 Department of Rheumatology, University of Medicine and Pharmacy of Craiova, 200349 Craiova, Romania; [email protected] * Correspondence: [email protected] (V.P.); dan.fl[email protected] (D.N.F.); [email protected] (R.P.) † All these authors contributed equally to this work. Citation: Bobirc˘a,A.; Bobirc˘a,F.; Ancuta, I.; Florescu, A.; P˘adureanu, Simple Summary: Cancer therapy has evolved over the years, immunotherapy being the most used V.; Florescu, D.N.; P˘adureanu, R.; for untreatable malignant tumors. Immune checkpoint inhibitors decrease the ability of tumor cells Florescu, A.; Mus, etescu, A.E. -
Key Enzymes in Cancer: Mechanism of Action and Inhibition with Anticancer Agents
University of Texas Rio Grande Valley ScholarWorks @ UTRGV Chemistry Faculty Publications and Presentations College of Sciences 2018 Key Enzymes in Cancer: Mechanism of Action and Inhibition With Anticancer Agents Debasish Bandyopadhyay The University of Texas Rio Grande Valley, [email protected] Gabriel Lopez The University of Texas Rio Grande Valley Stephanie Cantu The University of Texas Rio Grande Valley Samantha Balboa The University of Texas Rio Grande Valley Annabel Garcia The University of Texas Rio Grande Valley See next page for additional authors Follow this and additional works at: https://scholarworks.utrgv.edu/chem_fac Part of the Chemistry Commons, and the Life Sciences Commons Recommended Citation Debasish Bandyopadhyay, Gabriel Lopez, Stephanie Cantu, Samantha Balboa, Annabel Garcia, Christina Silva, Diandra Valdes. In Chemistry Research and Applications (Vol. 2): Organic and Medicinal Chemistry, Chapter 9; Key Enzymes in Cancer: Mechanism of Action and Inhibition with Anticancer Agents. 2018, Nova Science Publishers, Inc., Hauppauge, New York, USA (ISBN: 978-1-53614-855-8). This Book is brought to you for free and open access by the College of Sciences at ScholarWorks @ UTRGV. It has been accepted for inclusion in Chemistry Faculty Publications and Presentations by an authorized administrator of ScholarWorks @ UTRGV. For more information, please contact [email protected], [email protected]. Authors Debasish Bandyopadhyay, Gabriel Lopez, Stephanie Cantu, Samantha Balboa, Annabel Garcia, Christina Silva, and Diandra Valdes This book is available at ScholarWorks @ UTRGV: https://scholarworks.utrgv.edu/chem_fac/131 In: Organic and Medicinal Chemistry, Volume 2 ISBN: 978-1-53614-855-8 Editor: Bimal Krishna Banik © 2019 Nova Science Publishers, Inc. -

Immunostimulatory Effects of Low-Dose Cyclophosphamide Are Controlled by Inducible Nitric Oxide Synthase
Priority Report Immunostimulatory Effects of Low-Dose Cyclophosphamide Are Controlled by Inducible Nitric Oxide Synthase Markus Loeffler, Jo¨rg A. Kru¨ger, and Ralph A. Reisfeld Department of Immunology, The Scripps Research Institute, La Jolla, California Abstract and various tumor cells. Besides its effects on pericytes, it has been Cyclophosphamide is a widely used chemotherapeutic drug implicated in autocrine growth stimulation, formation of tumor that was recently applied as either an antiangiogenic/ stroma, and control of the interstitial tumor pressure therefore antivasculogenic or an immunostimulatory agent in combi- making it a promising target for tumor vaccinations (7). nation with cancer immunotherapies. It has been previously We show here for the first time that the cyclophosphamide- shown that cyclophosphamide augments the efficacy of mediated inhibition of inducible nitric oxide synthase (iNOS) is antitumor immune responses by depleting CD4+CD25+ T directly linked to its immunostimulatory but not to its anti- regulatory cells and increasing both T-lymphocyte prolife- vasculogenic effects. Furthermore, we show that the newly ration and T memory cells. Furthermore, cyclophosphamide described mechanism applies to tumor bearing mice and can be was shown to mediate killing of circulating endothelial employed in different tumor models to greatly enhance the progenitors. However, the molecular basis for these obser- antitumor effect of an oral DNA vaccine targeting PDGF-B, delivered by attenuated Salmonella typhimurium to secondary vations has not yet been elucidated. We show here that the cyclophosphamide-mediated inhibition of inducible nitric lymphoid tissue. oxide synthase is directly linked to its immunostimulatory Materials and Methods but not to its antivasculogenic effects. -
Best Practices for Implementing Cancer Immunotherapy in the Community
ASSOCIATION OF COMMUNITY CANCER CENTERS IMMUNO- ONCOLOGY INSTITUTE Best Practices for Implementing Cancer Immunotherapy in the Community The Association of Community Cancer Centers (ACCC) recently checkpoint inhibitors. Although most patients show response hosted live continuing medical education (CME)-certified learn- to treatment at approximately 6 to 10 weeks after therapy initi- ing workshops at two community cancer programs to review ation, responses can be nuanced. For instance, current barriers to immunotherapy implementation in the com- pseudoprogression can occur (e.g., in about 10 percent of munity setting. During the workshops, an expert faculty panel patients with melanoma), in which there is a transient worsening engaged participants in discussion on the challenges that they of disease prior to disease stabilization or regression. Clinicians may face as they integrate immunotherapy into their clinical prac- should be familiar with response evaluation criteria monitoring tice, as well as practical solutions and strategies they can apply parameters to measure treatment response.1 to overcome these barriers. This article summarizes the guidance Early recognition of irAEs is essential for effective manage- and information provided by the faculty on the various issues ment; therefore, clinicians need to have a high index of suspicion raised during the workshop discussions. for irAEs. The type and broad distribution of irAEs differ consid- erably from toxicities associated with chemotherapy, and Decision-Making in Therapy Selection -

An Investigator-Initiated Open-Label Trial of Sonidegib in Advanced Basal Cell Carcinoma Patients Resistant to Vismodegib Christina Danial, Kavita Y
Published OnlineFirst November 6, 2015; DOI: 10.1158/1078-0432.CCR-15-1588 Clinical Trial Brief Report Clinical Cancer Research An Investigator-Initiated Open-Label Trial of Sonidegib in Advanced Basal Cell Carcinoma Patients Resistant to Vismodegib Christina Danial, Kavita Y. Sarin, Anthony E. Oro, and Anne Lynn S. Chang Abstract Purpose: To assess the tumor response to the smoothened sive disease with sonidegib. Three patients experienced stable (SMO) inhibitor, sonidegib (LDE225), in patients with an disease and discontinued sonidegib either due to adverse events advanced basal cell carcinoma (BCC) resistant to treatment with (n ¼ 1) or due to election for surgery (n ¼ 2). The response of one vismodegib (GDC0449). patient was not evaluable. SMO mutations with in vitro data Experimental Design: Nine patients with an advanced suggesting resistance to Hh pathway inhibition were identified BCC that was previously resistant to treatment with vismode- in 5 patients, and none of these patients experienced responses gib were given sonidegib in this investigational, open- while on sonidegib. label study. Tumor response was determined using the Conclusion: Patients with advanced BCCs that were response evaluation criteria in solid tumors. SMO mutations previously resistant to treatment with vismodegib similarly were identified using biopsy samples from the target BCC demonstrated treatment resistance with sonidegib. Patients location. who have developed treatment resistance to an SMO inhibitor Results: The median duration of treatment with sonidegib was may continue to experience tumor progression in response to 6 weeks (range, 3–58 weeks). Five patients experienced progres- other SMO inhibitors. Clin Cancer Res; 1–5. Ó2015 AACR. Introduction Sonidegib (LDE225) is a new SMO inhibitor approved in 2015 by the FDA for locally advanced BCCs. -
A Review on Cancer Immunotherapy and Applications of Nanotechnology to Chemoimmunotherapy of Different Cancers
molecules Review A Review on Cancer Immunotherapy and Applications of Nanotechnology to Chemoimmunotherapy of Different Cancers Safiye Akkın 1 , Gamze Varan 2 and Erem Bilensoy 1,* 1 Department of Pharmaceutical Technology, Faculty of Pharmacy, Hacettepe University, 06100 Ankara, Turkey; akkinsafi[email protected] 2 Department of Vaccine Technology, Hacettepe University Vaccine Institute, 06100 Ankara, Turkey; [email protected] * Correspondence: [email protected] Abstract: Clinically, different approaches are adopted worldwide for the treatment of cancer, which still ranks second among all causes of death. Immunotherapy for cancer treatment has been the focus of attention in recent years, aiming for an eventual antitumoral effect through the immune system response to cancer cells both prophylactically and therapeutically. The application of nanoparticulate delivery systems for cancer immunotherapy, which is defined as the use of immune system features in cancer treatment, is currently the focus of research. Nanomedicines and nanoparticulate macro- molecule delivery for cancer therapy is believed to facilitate selective cytotoxicity based on passive or active targeting to tumors resulting in improved therapeutic efficacy and reduced side effects. Today, with more than 55 different nanomedicines in the market, it is possible to provide more effective cancer diagnosis and treatment by using nanotechnology. Cancer immunotherapy uses the body’s immune system to respond to cancer cells; however, this may lead to increased immune response Citation: Akkın, S.; Varan, G.; and immunogenicity. Selectivity and targeting to cancer cells and tumors may lead the way to safer Bilensoy, E. A Review on Cancer immunotherapy and nanotechnology-based delivery approaches that can help achieve the desired Immunotherapy and Applications of success in cancer treatment.