Identification of Filarial Vector Mosquito, Culex Quinquefasciatus, and Infection Using PCR Assays
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Saint Louis Encephalitis (SLE)
Encephalitis, SLE Annual Report 2018 Saint Louis Encephalitis (SLE) Saint Louis Encephalitis is a Class B Disease and must be reported to the state within one business day. St. Louis Encephalitis (SLE), a flavivirus, was first recognized in 1933 in St. Louis, Missouri during an outbreak of over 1,000 cases. Less than 1% of infections manifest as clinically apparent disease cases. From 2007 to 2016, an average of seven disease cases were reported annually in the United States. SLE cases occur in unpredictable, intermittent outbreaks or sporadic cases during the late summer and fall. The incubation period for SLE is five to 15 days. The illness is usually benign, consisting of fever and headache; most ill persons recover completely. Severe disease is occasionally seen in young children but is more common in adults older than 40 years of age, with almost 90% of elderly persons with SLE disease developing encephalitis. Five to 15% of cases die from complications of this disease; the risk of fatality increases with age in older adults. Arboviral encephalitis can be prevented by taking personal protection measures such as: a) Applying mosquito repellent to exposed skin b) Wearing protective clothing such as light colored, loose fitting, long sleeved shirts and pants c) Eliminating mosquito breeding sites near residences by emptying containers which hold stagnant water d) Using fine mesh screens on doors and windows. In the 1960s, there were 27 sporadic cases; in the 1970s, there were 20. In 1980, there was an outbreak of 12 cases in New Orleans. In the 1990s, there were seven sporadic cases and two outbreaks; one outbreak in 1994 in New Orleans (16 cases), and the other in 1998 in Jefferson Parish (14 cases). -

Downloadable Data Collection
Smetzer et al. Movement Ecology (2021) 9:36 https://doi.org/10.1186/s40462-021-00275-5 RESEARCH Open Access Individual and seasonal variation in the movement behavior of two tropical nectarivorous birds Jennifer R. Smetzer1* , Kristina L. Paxton1 and Eben H. Paxton2 Abstract Background: Movement of animals directly affects individual fitness, yet fine spatial and temporal resolution movement behavior has been studied in relatively few small species, particularly in the tropics. Nectarivorous Hawaiian honeycreepers are believed to be highly mobile throughout the year, but their fine-scale movement patterns remain unknown. The movement behavior of these crucial pollinators has important implications for forest ecology, and for mortality from avian malaria (Plasmodium relictum), an introduced disease that does not occur in high-elevation forests where Hawaiian honeycreepers primarily breed. Methods: We used an automated radio telemetry network to track the movement of two Hawaiian honeycreeper species, the ʻapapane (Himatione sanguinea) and ʻiʻiwi (Drepanis coccinea). We collected high temporal and spatial resolution data across the annual cycle. We identified movement strategies using a multivariate analysis of movement metrics and assessed seasonal changes in movement behavior. Results: Both species exhibited multiple movement strategies including sedentary, central place foraging, commuting, and nomadism , and these movement strategies occurred simultaneously across the population. We observed a high degree of intraspecific variability at the individual and population level. The timing of the movement strategies corresponded well with regional bloom patterns of ‘ōhi‘a(Metrosideros polymorpha) the primary nectar source for the focal species. Birds made long-distance flights, including multi-day forays outside the tracking array, but exhibited a high degree of fidelity to a core use area, even in the non-breeding period. -

Potentialities for Accidental Establishment of Exotic Mosquitoes in Hawaii1
Vol. XVII, No. 3, August, 1961 403 Potentialities for Accidental Establishment of Exotic Mosquitoes in Hawaii1 C. R. Joyce PUBLIC HEALTH SERVICE QUARANTINE STATION U.S. DEPARTMENT OF HEALTH, EDUCATION, AND WELFARE HONOLULU, HAWAII Public health workers frequently become concerned over the possibility of the introduction of exotic anophelines or other mosquito disease vectors into Hawaii. It is well known that many species of insects have been dispersed by various means of transportation and have become established along world trade routes. Hawaii is very fortunate in having so few species of disease-carrying or pest mosquitoes. Actually only three species are found here, exclusive of the two purposely introduced Toxorhynchites. Mosquitoes still get aboard aircraft and surface vessels, however, and some have been transported to new areas where they have become established (Hughes and Porter, 1956). Mosquitoes were unknown in Hawaii until early in the 19th century (Hardy, I960). The night biting mosquito, Culex quinquefasciatus Say, is believed to have arrived by sailing vessels between 1826 and 1830, breeding in water casks aboard the vessels. Van Dine (1904) indicated that mosquitoes were introduced into the port of Lahaina, Maui, in 1826 by the "Wellington." The early sailing vessels are known to have been commonly plagued with mosquitoes breeding in their water supply, in wooden tanks, barrels, lifeboats, and other fresh water con tainers aboard the vessels, The two day biting mosquitoes, Aedes ae^pti (Linnaeus) and Aedes albopictus (Skuse) arrived somewhat later, presumably on sailing vessels. Aedes aegypti probably came from the east and Aedes albopictus came from the western Pacific. -
Apapane (Himatione Sanguinea)
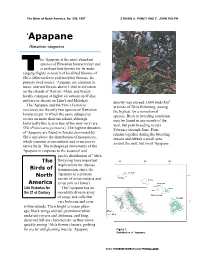
The Birds of North America, No. 296, 1997 STEVEN G. FANCY AND C. JOHN RALPH 'Apapane Himatione sanguinea he 'Apapane is the most abundant species of Hawaiian honeycreeper and is perhaps best known for its wide- ranging flights in search of localized blooms of ō'hi'a (Metrosideros polymorpha) flowers, its primary food source. 'Apapane are common in mesic and wet forests above 1,000 m elevation on the islands of Hawai'i, Maui, and Kaua'i; locally common at higher elevations on O'ahu; and rare or absent on Lāna'i and Moloka'i. density may exceed 3,000 birds/km2 The 'Apapane and the 'I'iwi (Vestiaria at times of 'ōhi'a flowering, among coccinea) are the only two species of Hawaiian the highest for a noncolonial honeycreeper in which the same subspecies species. Birds in breeding condition occurs on more than one island, although may be found in any month of the historically this is also true of the now very rare year, but peak breeding occurs 'Ō'ū (Psittirostra psittacea). The highest densities February through June. Pairs of 'Apapane are found in forests dominated by remain together during the breeding 'ōhi'a and above the distribution of mosquitoes, season and defend a small area which transmit avian malaria and avian pox to around the nest, but most 'Apapane native birds. The widespread movements of the 'Apapane in response to the seasonal and patchy distribution of ' ōhi'a The flowering have important implications for disease Birds of transmission, since the North 'Apapane is a primary carrier of avian malaria and America avian pox in Hawai'i. -

Host Preference of Mosquitoes in Bernalillo County New Mexico'''
Joumal of the American Mosquito Control Association, l3(l):71J5' L99'l Copyright @ 1997 by the American Mosquito Control Association' Inc. HOST PREFERENCE OF MOSQUITOES IN BERNALILLO COUNTY NEW MEXICO''' K. M. LOF[IN,3j R. L. BYFORD,3 M. J. LOF[IN,3 M. E. CRAIG,T t'ro R. L. STEINERs ABSTRACT. Host preference of mosquitoes was determined using animal-baited traps. Hosts used in the study were cattle, chickens, dogs, and horses. Ten mosquito species representing 4 genera were collected from the animal-baited traps. Aedes vexans, Aedes dorsalis, Culex quinquefasciatus, Culex tarsalis, and Culiseta inomata were used as indicator species for data analysis. Greater numbers of Ae. vexans, Ae. dorsalis, and C.s. inornata were collected from cattle and horses than from chickens or dogs. In addition, engorgement rates were higher on mammals than on chickens. Engorgement and attraction data for Cx. quinquefasciatrs suggested a preference for chickens and dogs over cattle and horses. A slight preference for chickens and dogs was seen with Cx. tarsalis, but the degree of host preference of C.r. tarsalis was less than that in either Ae. vexans or Cx. quinquefasciatus. INTRODUCTION used cattle-baited traps to determine the biting flies and mosquitoes attacking cattle in Canada. Host preference is an important aspect of arthro- Studiesin the USA comparing relative attraction pod-borne diseases. Determining the host prefer- of multiple host species in traps are limited. In a ence of mosquitoes can aid in understanding the Texas rice-growing area, Kuntz et al. (1982) used transmissionof diseaseswithin a geographicalarea multiple, paired host speciesto determine that cattle (Defoliart et al. -
An Odorant Receptor from Anopheles Sinensis in China Is Sensitive To
Liu et al. Malar J (2018) 17:348 https://doi.org/10.1186/s12936-018-2501-4 Malaria Journal RESEARCH Open Access An odorant receptor from Anopheles sinensis in China is sensitive to oviposition attractants Hongmei Liu1* , Luhong Liu2, Peng Cheng1, Xiaodan Huang1 and Maoqing Gong1* Abstract Background: Anopheles sinensis is an important vector for the spread of malaria in China. Olfactory-related behav- iours, particularly oviposition site seeking, ofer opportunities for disrupting the disease-transmission process. Results: This is the frst report of the identifcation and characterization of AsinOrco and AsinOR10 in An. sinensis. AsinOrco and AsinOR10 share 97.49% and 90.37% amino acid sequence identity, respectively, with related sequences in Anopheles gambiae. A functional analysis demonstrated that AsinOrco- and AsinOR10-coexpressing HEK293 cells were highly sensitive to 3-methylindole, but showed no signifcant diferences in response to other test odorants when compared to DMSO. Conclusions: AsinOrco was characterized as a new member of the Orco ortholog subfamily. AsinOR10, which appears to be a member of the OR2-10 subfamily, is directly involved in identifcation of oviposition sites. This fnding will help to elucidate the molecular mechanisms underlying olfactory signaling in An. sinensis and provide many more molecular targets for eco-friendly pest control. Keywords: Anopheles sinensis, AsinOrco, AsinOR10, 3-Methylindole Background malaria in some regions; even if the source of infection Malaria is one of the most important infectious diseases can be discovered and cleared in a timely, there is still a seriously endangering human health and safety. Te risk of local transmission and epidemic rebound. With World Health Organization (WHO) lists malaria with rapid globalization and implementation of the national AIDS and tuberculosis as the top three public health “Belt and Road” initiative, the number of people visit- problems globally. -

Genetic Diversity of Culex Pipiens Mosquitoes in Distinct Populations from Europe: Contribution of Cx
Shaikevich et al. Parasites & Vectors (2016) 9:47 DOI 10.1186/s13071-016-1333-8 RESEARCH Open Access Genetic diversity of Culex pipiens mosquitoes in distinct populations from Europe: contribution of Cx. quinquefasciatus in Mediterranean populations Elena V. Shaikevich1, Elena B. Vinogradova2, Ali Bouattour3 and António Paulo Gouveia de Almeida4,5* Abstract Background: Mosquitoes of the Culex pipiens complex are cosmopolitan, and important vectors of neglected tropical diseases, such as arbovirosis and lymphatic filariasis. Among the complex taxa, Cx. pipiens (with two forms pipiens and molestus) and Cx. quinquefasciatus are the most ubiquitous mosquitoes in temperate and tropical regions respectively. Mosquitoes of this taxa lack of morphological differences between females, but have frank behavioral and physiological differences and have different trophic preferences that influence their vectorial status. Hybridization may change the vectorial capacity of these mosquitoes, increasing vector efficiency and medical importance of resulting hybrids. Methods: Culex pipiens s.l. from 35 distinct populations were investigated by the study of mtDNA, symbiotic bacterium Wolbachia pipientis, nuclear DNA and flanking region of microsatellite CQ11 polymorphism using PCR with diagnostic primers, RFLP analysis and sequencing. Results: Six different mitochondrial haplotypes were revealed by sequencing of the cytochrome oxidase subunit I (COI) gene and three different Wolbachia (wPip) groups were identified. A strong association was observed between COI haplotypes/groups, wPip groups and taxa; haplogroup A and infection with wPipII appear to be typical for Cx. pipiens form pipiens, haplotype D and infection with wPipIV for form molestus, while haplogroup E, characteristic of Cx. quinquefasciatus, were correlated with wPipI and found in Cx. -

Embryo Polarity in Moth Flies and Mosquitoes Relies on Distinct Old
RESEARCH ARTICLE Embryo polarity in moth flies and mosquitoes relies on distinct old genes with localized transcript isoforms Yoseop Yoon1, Jeff Klomp1†, Ines Martin-Martin2, Frank Criscione2, Eric Calvo2, Jose Ribeiro2, Urs Schmidt-Ott1* 1Department of Organismal Biology and Anatomy, University of Chicago, Chicago, United States; 2Laboratory of Malaria and Vector Research, National Institute of Allergy and Infectious Diseases, Rockville, United States Abstract Unrelated genes establish head-to-tail polarity in embryos of different fly species, raising the question of how they evolve this function. We show that in moth flies (Clogmia, Lutzomyia), a maternal transcript isoform of odd-paired (Zic) is localized in the anterior egg and adopted the role of anterior determinant without essential protein change. Additionally, Clogmia lost maternal germ plasm, which contributes to embryo polarity in fruit flies (Drosophila). In culicine (Culex, Aedes) and anopheline mosquitoes (Anopheles), embryo polarity rests on a previously unnamed zinc finger gene (cucoid), or pangolin (dTcf), respectively. These genes also localize an alternative transcript isoform at the anterior egg pole. Basal-branching crane flies (Nephrotoma) also enrich maternal pangolin transcript at the anterior egg pole, suggesting that pangolin functioned as ancestral axis determinant in flies. In conclusion, flies evolved an unexpected diversity of anterior determinants, and alternative transcript isoforms with distinct expression can adopt fundamentally distinct developmental roles. *For correspondence: [email protected] DOI: https://doi.org/10.7554/eLife.46711.001 Present address: †University of North Carolina, Lineberger Comprehensive Cancer Center, Introduction Chapel Hill, United States The specification of the primary axis (head-to-tail) in embryos of flies (Diptera) offers important Competing interests: The advantages for studying how new essential gene functions evolve in early development. -

Seasonal Abundance and Molecular Identification of West Nile Virus
Seasonal abundance and molecular identification of West Nile virus vectors, Culex pipens and Culex quinquefasciatus (diptera: culicidae) in Abeokuta, South-West, Nigeria. Babatunde Olanrewaju Motayo1, Bernard Aneibe Onoja2, Adedayo Omotayo Faneye2, Johnson Adekunle Adeniji2 1. Federal Medical Centre, Microbiology Unit, Pathology Department. 2. University of Ibadan, Virology. Abstract: Background: West Nile virus (WNV) infection, is an arbovirus infection with high morbidity and mortality, the vector respon- sible for both human and animal transmission is Culex pipens complex. Objective: To determine the species distribution and seasonal abundance of Culex pipens and Culex quinquefasciatus mosquitoes in Abeokuta, Nigeria. Methods: Mosquitoes belonging to the Culex pipens complex were captured in three different locations located within Abeokuta Metropolis between March 2012 and January 2013. Individual species were identified using morphometric methods. Amplifica- tion of the Ace2 gene by PCR confirmed morphormetric identification of the mosquitoes. Results: A total of 751 mosquitoes were captured. Culex quinquefaciatus recorded the highest distribution of vectors with 56.6% and Culex pipens 43.4% (P > 0.05). Idi aba community recorded the highest distribution of mosquito vectors with 42.9% (n=322) and Culex quinqueaciatus was more abundantly distributed with 183 mosquitoes. Aro community recorded 32% (n=240) of cap- tured mosquitoes with Culex quinquefaciatus having a higher level of abundance and lastly Kemta with a distribution of 25.1% (n=189). Conclusion: Results from this study show that potential vectors of WNV abound within Abeokuta, putting residents at high risk of West Nile infection. We advocate for introduction of routine testing of WNV in Abeokuta and Nigeria. Keywords: West Nile Virus, Culex pipens complex, PCR, Abeokuta. -

Environmental and Biological Factors Influencing Culex Pipiens Quinquefasciatus Say (Diptera: Culicidae) Vector Competence for Saint Louis Encephalitis Virus
Am. J. Trop. Med. Hyg., 81(2), 2009, pp. 264–272 Copyright © 2009 by The American Society of Tropical Medicine and Hygiene Environmental and Biological Factors Influencing Culex pipiens quinquefasciatus Say (Diptera: Culicidae) Vector Competence for Saint Louis Encephalitis Virus Stephanie L. Richards , * Cynthia C. Lord , Kendra Pesko , and Walter J. Tabachnick Florida Medical Entomology Laboratory, University of Florida, Vero Beach, Florida Abstract. Complex interactions between environmental and biological factors influence the susceptibility of Culex pipiens quinquefasciatus to St. Louis encephalitis virus and could affect the epidemiology of virus transmission. Similar interactions could have epidemiologic implications for other vector-virus systems. We conducted an experiment to exam- ine four such factors in combination: mosquito age, extrinsic incubation temperature (EIT), virus dose, and colony. The proportion of mosquitoes with body infections or disseminated infections varied between colonies, and was dependant on age, EIT, and dose. We also show that the probability of a body or leg infection interacted in complex ways between colonies, ages, EITs, and doses. The complex interactive effects of environmental and biological factors must be taken into account for studies of vector competence and epidemiology, especially when laboratory studies are used to generalize to natural transmission dynamics where the extent of variation is largely unknown. INTRODUCTION quefasciatus . 10 However, the relationship between infection and dissemination changed depending on the EIT, but not Mosquito biology and the environment can play important the dose. This inconsistency and also the limited information roles in mosquito vector competence. The effect of environ- on the impact of mosquito age on vector competence was the mental factors such as extrinsic incubation temperature (EIT) basis for the current investigation. -

Optimized CRISPR Tools and Site-Directed Transgenesis in Culex Quinquefasciatus Mosquitoes for Gene Drive Development
bioRxiv preprint doi: https://doi.org/10.1101/2021.02.10.430702; this version posted February 11, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Optimized CRISPR tools and site-directed transgenesis in Culex quinquefasciatus mosquitoes for gene drive development. 1 1 2,3 1 1 Xuechun Feng , Víctor López Del Amo , Enzo Mameli , Megan Lee , Alena L. Bishop , 2,4 1* Norbert Perrimon , Valentino M. Gantz . 1 Section of Cell and Developmental Biology, University of California San Diego, La Jolla, CA 92093. 2 Department of Genetics, Blavatnik Institute, Harvard Medical School, Boston, MA 02115. 3 National Emerging Infectious Diseases Laboratories (NEIDL), Boston University, Boston, MA 02118. 4 HHMI, Harvard Medical School, Boston, MA 02115. *Correspondence: [email protected] Keywords: population engineering, insect control, mosquito, Culex, CRISPR, HDR, gene drive. ABSTRACT Culex mosquitoes are a global vector for multiple human and animal diseases, including West Nile virus, lymphatic filariasis, and avian malaria, posing a constant threat to public health, livestock, companion animals, and endangered birds. While rising insecticide resistance has threatened the control of Culex mosquitoes, advances in CRISPR genome-editing tools have fostered the development of alternative genetic strategies such as gene drive systems to fight disease vectors. However, though gene-drive technology has quickly progressed in other mosquitoes, advances have been lacking in Culex. Here, we developed a Culex-specific Cas9/gRNA expression toolkit and used site-directed homology-based transgenesis to generate and validate a Culex quinquefasciatus Cas9-expressing line. -

HSP Superfamily of Genes in the Malaria Vector Anopheles Sinensis
Si et al. Malar J (2019) 18:132 https://doi.org/10.1186/s12936-019-2770-6 Malaria Journal RESEARCH Open Access HSP superfamily of genes in the malaria vector Anopheles sinensis: diversity, phylogenetics and association with pyrethroid resistance Feng‑Ling Si1,2†, Liang Qiao2, Qi‑Yi He2, Yong Zhou2, Zhen‑Tian Yan2 and Bin Chen2*† Abstract Background: Heat shock proteins (HSPs) are molecular chaperones that are involved in many normal cellular processes and various kinds of environmental stress. There is still no report regarding the diversity and phylogenetics research of HSP superfamily of genes at whole genome level in insects, and the HSP gene association with pyrethroid resistance is also not well known. The present study investigated the diversity, classifcation, scafold location, charac‑ teristics, and phylogenetics of the superfamily of genes in Anopheles sinensis genome, and the HSP genes associated with pyrethroid resistance. Methods: The present study identifed the HSP genes in the An. sinensis genome, analysed their characteristics, and deduced phylogenetic relationships of all HSPs in An. sinensis, Anopheles gambiae, Culex quinquefasciatus and Aedes aegypti by bioinformatic methods. Importantly, the present study screened the HSPs associated with pyrethroid resist‑ ance using three feld pyrethroid‑resistant populations with RNA‑seq and RT‑qPCR, and looked over the HSP gene expression pattern for the frst time in An. sinensis on the time‑scale post insecticide treatment with RT‑qPCR. Results: There are 72 HSP genes in An. sinensis genome, and they are classifed into fve families and 11 subfamilies based on their molecular weight, homology and phylogenetics. Both RNA‑seq and qPCR analysis revealed that the expression of AsHSP90AB, AsHSP70‑2 and AsHSP21.7 are signifcantly upregulated in at least one feld pyrethroid‑resist‑ ant population.