Targeted Lung Health Checks Report.Pdf
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

121 Residential Properties in Bedfordshire and Buckinghamshire 1 Executive Summary Milton Keynes
121 RESIDENTIAL PROPERTIES IN BEDFORDSHIRE AND BUCKINGHAMSHIRE 1 EXECUTIVE SUMMARY MILTON KEYNES The portfolio comprises four modern freehold residential assets. Milton Keynes is a ‘new town’ built in the 1960s. The area Geographically, the properties are each connected to the major incorporates the existing towns of Bletchley, Wolverton and economic centres of Luton or Milton Keynes as well as being Stony Stratford. The population in the 2011 Census totalled commutable to Central London. 248,800. The government have pledged to double the population by 2026. Milton Keynes is one of the more successful (per capita) The current owners have invested heavily in the assets economies in the South East. It has a gross value added per during their ownership including a high specification rolling capita index 47% higher than the national average. The retail refurbishment of units, which is ongoing. sector is the largest contributor to employment. The portfolio offers an incoming investor the opportunity KEY FACTS: to acquire a quality portfolio of scale benefitting from • Britain’s fastest growing city by population. The population management efficiencies, low running costs, a low entry price has grown 18% between 2004 and 2013, the job base having point into the residential market, an attractive initial yield and expanded by 24,400 (16%) over the same period. excellent reversionary yield potential. • Milton Keynes is home to some of the largest concentrations PORTFOLIO SUMMARY AND PERFORMANCE of North American, German, Japanese and Taiwanese firms in the UK. No. of Assets 4 No. of Units 121 • Approximately 18% of the population can be found in the PRS, Floor area (sq m / sq ft) 5,068 / 54,556 with growth of 133% since 2001. -

Luton & Central Bedfordshire
Luton & Central Bedfordshire Strategic Housing Market Assessment Refresh 2014 Report of Findings June 2014 Opinion Research Services | The Strand • Swansea • SA1 1AF | 01792 535300 | www.ors.org.uk | [email protected] Opinion Research Services | Luton & Central Bedfordshire SHMA Refresh 2014 – Report of Findings June 2014 Opinion Research Services The Strand, Swansea SA1 1AF Jonathan Lee | David Harrison | Nigel Moore enquiries: 01792 535300 · [email protected] · www.ors.org.uk © Copyright June 2014 2 Opinion Research Services | Luton & Central Bedfordshire SHMA Refresh 2014 – Report of Findings June 2014 Contents Summary of Key Findings ................................................................................... 6 Luton and Central Bedfordshire SHMA Refresh 2014 6 Key Challenges ............................................................................................................................................. 6 Private Rented Sector .................................................................................................................................. 6 Local Economy ............................................................................................................................................. 6 Housing Delivery .......................................................................................................................................... 6 Benefit Reform ........................................................................................................................................... -

Urban Capacity Report July 2017
Central Bedfordshire Council www.centralbedfordshire.gov.uk Urban Capacity Report July 2017 - 1 - Central Bedfordshire Urban Capacity Report Central Bedfordshire Urban Capacity Report 1. Introduction 1.1 The Urban Capacity Report sets out the different strands of policy and practice that, as a combined approach, demonstrate the Council are seeking every opportunity across Central Bedfordshire to maximise the use of available land within settlements, before looking to greenfield sites within the countryside in order to accommodate future growth requirements. This will ensure the Local Plan meets the requirements of the NPPF and the emerging direction of future policy as set out in the Housing White Paper. 2. Key Findings 2.1 The Urban Capacity Report discusses the following strands of policy and practice: Luton, Dunstable and Houghton Regis Urban Capacity Potential Study (2016) 2.2 Luton, Dunstable and Houghton Regis have a significant role to play in contributing towards growth within the Luton Housing Market Area (HMA). The Council commissioned Nexus Planning to prepare an Urban Capacity Study to identify the potential for achieving additional capacity from developments within the Luton, Dunstable and Houghton Regis conurbation. The Study conducted a two stage assessment: Stage One – A baseline assessment confirming the sites identified in the SHLAAs and ELRs for Central Bedfordshire and Luton Borough were still suitable for residential development. No new sites were considered. Stage Two – Testing the sites against alternative densities to see whether they could be increased to deliver additional homes. 2.3 The study concluded there may be an opportunity to increase development capacity by 148-496 dwellings within Central Bedfordshire, achieved through increasing density. -
What Industries Have Put Reading on the Map? Beer, Bulbs and Biscuits Reading Is Best Known for the ‘3Bs’ – Biscuits, Beer and Bulbs
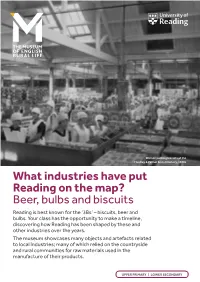
Women packing biscuits at the Huntley & Palmer biscuit factory, 1920s What industries have put Reading on the map? Beer, bulbs and biscuits Reading is best known for the ‘3Bs’ – biscuits, beer and bulbs. Your class has the opportunity to make a timeline, discovering how Reading has been shaped by these and other industries over the years. The museum showcases many objects and artefacts related to local industries; many of which relied on the countryside and rural communities for raw materials used in the manufacture of their products. UPPER PRIMARY | LOWER SECONDARY Learning outcomes By the end of this activity students will: THEMES AND TOPICS • be more aware of some of the industries that put Reading • A local history study. on the map and the town’s relationship with rural areas • be able to discuss when Reading’s industries first arrived LINKS WITH in the town by producing a timeline that outlines key dates OTHER ACTIVITIES ready to take to the museum to find out more. This activity could also be used in conjunction with the ‘What was farming like before modern Before you visit technology’ and ‘Making and manufacturing’ resources. Introduce your students to six businesses that have had an impact on Reading. There are archives online and the opportunities to find out more details about each business (see below). Making a timeline Students should create a timeline ready to take to the museum to add in key dates and events for the different industries. Finding archives such as photos on our database: • Visit merl.reading.ac.uk/research/using-collections/ databases • Click on the Enterprise database. -

Cambridgeshire Community Services NHS Trust: Providing Services Across Bedfordshire, Cambridgeshire, Luton, Milton Keynes, Norfolk, Peterborough & Suffolk
Cambridgeshire Community Services NHS Trust: providing services across Bedfordshire, Cambridgeshire, Luton, Milton Keynes, Norfolk, Peterborough & Suffolk Cambridgeshire Community Services NHS Trust: providing services across Bedfordshire, Cambridgeshire, Luton, Milton Keynes, Norfolk, Peterborough & Suffolk Contents Map of Trust geographical area and summary of services ......................................... 2 Part 1: Information about the Quality Account ........................................................... 3 Statement on Quality from the Chief Executive .................................................... 3 Statement from the Chief Nurse & Medical Director ............................................. 5 About the Quality Account ...................................................................................... 6 Part 2: Priorities for Improvement & Statement of Assurance from the Board ....... 7 Quality Improvement Priorities for 2021-22 ........................................................... 7 Statement of Assurance from the Board.............................................................. 11 2.1 Review of services ......................................................................................... 11 2.2 Learning from deaths ..................................................................................... 11 2.3 Participation in clinical audits and national confidential enquiries .................. 13 2.4 Participation in clinical research ................................................................... -

General Health and Limiting Long Term Illness in Luton
General Health and Limiting Long Term Illness in Luton Analysis of 2001 Census Data for Luton and the East of England Region Research and Intelligence Team Department of Environment & Regeneration Luton Borough Council Please note that Luton Borough Council is licensed by the Office for National Statistics to make available 2001 Census data to third parties. However this licence does not permit third parties to reproduce 2001 Census data without themselves obtaining a licence from the Office for National Statistics Contents Gender and Age by General Health and Limiting Long Term Illness Hours of care provided Source: 2001 Census [Key Statistics for Local Authorities; Key Statistics for Wards] © Crown Copyright Research and Intelligence Team Department of Environment & Regeneration Luton Borough Council Please note that Luton Borough Council is licensed by the Office for National Statistics to make available 2001 Census data to third parties. However this licence does not permit third parties to reproduce 2001 Census data without themselves obtaining a licence from the Office for National Statistics Introduction This paper aims to give a detailed insight into health in Luton within the context of the East of England region, and also of Luton’s wards within the Borough. It considers limiting long-term illness, general health, and hours of care. The paper draws upon detailed information from the 2001 Census, and alongside tables of data, charts and text, aims to highlight key trends. Please note that all information presented in this report is © Crown copyright data, and is reproduced with the permission of the Controller of HMSO. Luton Borough Council is permitted by licence to reproduce data from the 2001 Census for inclusion within presentations and internal reports. -

Sustainable Travel Plan
Sustainable Travel Plan for the period 2011 - 2015 Road Safety www.luton.gov.uk/roadsafety Luton Borough Council Sustainable Travel Plan 2011 - 2015 August 2011 Chris Padgin Planning and Transport Highways and Street Services CONTENTS PAGE 1.0 Introduction 1 2.0 Consultation 1 3.0 Working in Partnership 2 4.0 General 3 5.0 Walking 3 6.0 Cycling 6 7.0 Public Transport (bus) 8 8.0 Public Transport (rail) 10 9.0 Motorised Travel 11 10.0 Action Plan 12 11.0 LTP Indicators 18 12.0 Monitoring and Evaluation 18 13.0 Financial Implications 19 Sustainable Travel Plan 1.0 INTRODUCTION 1.1 It is generally acknowledged that sustainable travel is becoming more and more important. With the ever increasing population and the need to travel it is not possible to build enough roads to tackle congestion. There is also the concern about climate change. Both these have brought the need to change travel habits into more sustainable ways such as walking, cycling, use of public transport and car sharing. 1.2 Sustainable travel can offer a form of physical activity that can improve health at any stage in life, from childhood through to old age and is cost effective. Where people are inactive, encouraging people to undertake sustainable travel such as walking and cycling will help contribute to the reduction of illnesses and diseases such as obesity, diabetes, and mental health. 1.3 Everyone who lives, works or travels in Luton has a part to play in reducing congestion and carbon emissions. 1.4 The strategic direction is covered in the Local Transport Plan and this Sustainable Travel Plan covers the implementation of the Sustainable Travel Strategy (walking, cycling and public transport) to enable Luton residents and visitors to make Smarter Choices when considering their mode of travel. -

Proud Vibrant Ambitious Innovative
Appendix 2 PROUD VIBRANT AMBITIOUS INNOVATIVE A fresh and modern brand for Luton PROUD VIBRANT AMBITIOUS INNOVATIVE LUTON BRAND Luton’s proud, hardworking and resilient character has evolved over many decades. Hardworking and Skilful People and Passion Throughout the ages Luton has benefitted from a Above all, it’s the people that make Luton! Whether hardworking skilled workforce. Its Hat Making tradition, which supporting troops before they left for battle, celebrating began in the 17th century, is still celebrated today through cultural spectacles or sporting successes, or its communities its football team (The Hatters) and its iconic cultural building uniting to speak passionately against those attempting to (The Hat Factory). divide them, Lutonians have always demonstrated enormous A number of manufacturing firms flourished in Luton pride by joining together to support their own. throughout the 1900s. While its car production plant moved in the early 2000s, Vauxhall still has a very firm stamp on the town’s identity and its commercial vehicle operation is still thriving today. Location, location, location The Future Since its central train station opened in the 1800s and the Building on these strengths, Luton’s Investment Framework airport in the mid-1900s, Luton has become a connection outlines how the town will thrive and transform over the ‘hub’ to London, the UK and now the whole of Europe. This next 20 years. By creating a skilled, aspiring workforce and has been further enhanced by recent airport expansion plans attracting investment and business, Luton will become and major regeneration successes such as M1 Junction10a a centre for excellence in learning and creativity and an improvements and the Luton Dunstable Busway. -
Core Strategy: Preferred Options Summary Document April 2009
Luton and South Bedfordshire Joint Committee Local Development Framework Core Strategy: Preferred Options Summary Document April 2009 …shape your future… Luton and South Bedfordshire Joint Committee Core Strategy Preferred Options Summary Document 1. INTRODUCTION In 2007, the Luton and South Bedfordshire Joint Committee sought views on the delivery of Document development, to help inform future planning. Options sought to respond to some of the challenges this area faces. The Joint Committee want your views on its preferred options. Summary 2. BACKGROUND Options The Government's growth agenda requires that significant new development is delivered in Luton and southern Bedfordshire. In total, we need to The Committee is planning for 43,000 new homes between referred 2001 and 2031, and 35,000 new jobs, together with significant new supporting infrastructure. P The Core Strategy is the first planning document to address this agenda. Earlier public consultation and over twenty technical studies have informed this document. Strategy This leaflet is seeking views on the document to help the Committee plan growth sustainably. The Core full document: The Luton and South Bedfordshire Joint Committee Core Strategy: Preferred Options April 2009, and associated questionnaire are available to viewonline at www.shapeyourfuture.org.uk. We encourage you to read this and complete the questionnaire. Committee 3. THE SPATIAL STRATEGY: A SUMMARY Joint A key matter for the document is where should development go. The resulting Spatial Development Principles and associated policy, taken from the full document, is set out below for your consideration. Bedfordshire A) A Framework of Strategic Transport Infrastructure South To deliver sustainable development, it is important to ensure as much as possible is accessible by and public transport and other alternatives to the private car as well as responsibly planning for car use. -
Luton Hoo Location
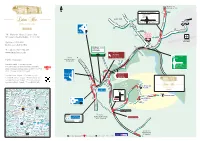
A505 TO HITCHIN, A1(M) N AIRPORT ROUNDABOUT Other routes A Parkway 6 A505 LUTON Vauxhall Motors HOTEL, GOLF & SPA Airport TERMINAL IBC Vehicles 5 W T 0 I C N 5 P A U D R D A K V I A M I Y L L A Luton W R K I M P TO D N A I R P O R T The Mansion House & R D Luton Hoo A1081 LUTON The Mansion House | Luton Hoo G PARKWAY Nr Luton I P S STATION Nr Luton Bedfordshire| Bedfordshire | LU1 3TQ Y L LU1 3TQ A LUTON SatNav - LU1SatNav 4LE3TQ - LU1 3TQ Deliveries - LU1 3TG AIRPORT Y A W Deliveries - LU1 3TG T: +44 (0)1582 734 437 T R St Albans O www.lutonhoo.com A1081 A I R P M6Harpenden LO T: +44 (0) 1582 734 437 Local traffic W E R Luton Hoo www.lutonhoo.co.uk H Woodside 1 A Public Transport 8 R Animal Farm 0 P M1 A1081 L 1 E O M1 TO N Stockwood Park A N St. Albans By Rail, D MILTON KEYNES, O D N E Public TransportLuton Parkway - approximately 5 minutes by taxi. R THE NORTH N O A For information on train operators and times phone D R Luton ParkwayNational - 5Rail minutes Enquiries by ontaxi. 0845 7484950 or check D Town Centre www.nationalrail.co.uk Dunstable A505 For information on train operators and times, M B Wheathampstead 1 6 phone NationalBy Air, Rail Enquiries on 0845 7484950 5 (B653) London 3 or check www.nationalrail.co.ukLondon Luton Airport - approximately 15 minutes L by taxi. -

Valor Park Thurrock157
EASTERN AVENUE I WEST THURROCK I RM20 3LW VALOR PARK THURROCK157 AVAILABLE SUMMER 2019 M25 LOGISTICS OPPORTUNITY 156,958 SQ FT (14,582 SQ M) THURROCK157 is a modern purpose built logistics building constructed in 1999 extending to 156,958 sq ft (GIA), set on a 9-acre site area. Situated in West Thurrock, the largest regeneration area in the UK and fastest growing local economy, the property benefits from excellent transport links HIGH QUALITY and access to the A13 and M25. TO BE FULLY REFURBISHED M6 M6 A1 (M) M65 M62 M62 PORT OF M6 M61 HULL/GRIMSBY/IMMINGHAM M1 A1 (M) M60 MANCHESTER M62 M25 (2 MILES) SHEFFIELD M53 QUEEN ELIZABETH BRIDGE M1 CHESTER CHESTERFIELD A1 (M) LOCAL M6 DARTFORD TUNNEL OCCUPIERS: DRIVE TIMES M1 M54 PETERBOROUGH 0-90 MINS 90-180 MINS 180-270 MINS AMAZON M6 LEICESTER A1 (M) M6 BIRMINGHAM A14 M42 COVENTRY A14 CAMBRIDGE B186 M1 A14 M5 A6 COMMUNICATIONS NORTHAMPTON M40 A1 (M) M25 J31 1 mile Chafford Hundred Station 1.2 miles (walk) VALOR PARK CHELTENHAM M1 M11 LOGISTICS CITY PORT OF MARSTONS/SELCO/SAINT GOBAIN THURROCK157 A12 M5 A1 (M) FElIXSTOWE M25 J30 2 miles OXFORD CHELMSFORD A13 (Mar Dyke Interchange ) 2 miles M40 M25 SWANSEA WEST THURROCK BRISTOL LONDON Tilbury Docks (A13) 8 miles TRADE CITY M25 GATEWAY A282 CARDIFF M4 LONDON TILBURY London Gateway (A13) 11 miles M4 HEATHROW DOCKS HERMES M4 JAMES LATHAM BATH North Circular Rd (A406) 11 miles M5 M25 J13 PARK M3 M25 DOVER London City Airport 14 miles PORT OF DOVER Central London 20 miles M3 Luton International Airport 55 miles M5 SOUTHAMPTON BRIGHTON PORT OF FOLKESTONE -

Announcing the South East Creative, Cultural and Digital Support Programme (SECCADS)
Announcing the South East Creative, Cultural and Digital Support programme (SECCADS) 1 Why are we running the SECCADS Programme? “The Creative Industries are a success story, playing a key role in the UK’s economic recovery. They contributed £87.4bn in GVA in 2015, 5.3% of the UK economy (comparable to the Construction and Information sectors) and between 2010 and 2015 grew by 34% - faster than any other sector. They have also outperformed other sectors in terms of employment growth: between 2011 and 2016, employment in the sector increased by 25.4% (circa 400,000 jobs) compared to 7.6% average across the wider UK. The sector is a net exporter of services (£11.3bn surplus in 2015)” Independent Review of the Creative Industries, Sir Peter Bazalgette 2017 The South East Local Enterprise Partnership (SELEP) wishes to ensure that it supports and benefits from this growth sector. Aware that the Creative, Cultural and Digital Sector does not tend to access mainstream business support, SELEP has supported the South East Creative Economy Network to develop SECCADS. SECCADS is designed to specifically attract and meet the needs of the sector. What is SECCADS? SECCADS will be a two-year business support programme designed to support Creative, Cultural and Digital Businesses (2018 – 2020). There will be three categories of support on offer: • Cluster- it: support to encourage cluster development across the SELEP area and into key markets such as London • Design-it: support for business start-ups in the sector • Grow-it: support for business growth There will be: • Local Coordinators located in each of the three areas: Essex, Kent & Medway and East Sussex.