When Anthropological Considerations Influence Our Attitude About the Chin and Orthognathic Surgery
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Assessment of Digital Panoramic Radiograph Magnification on Vertical Measurement Accuracy in Posterior Mandibular Regions
International Journal of Medical and Health Research Original Research Article International Journal of Medical and Health Research ISSN: 2454-9142; Impact Factor: RJIF 5.54 Received: 26-10-2018; Accepted: 28-11-2018 www.medicalsciencejournal.com Volume 4; Issue 12; December 2018; Page No. 184-186 Assessment of digital panoramic radiograph magnification on vertical measurement accuracy in posterior mandibular regions Dr. Kumar Gaurav Dubey1, Dr. Richa Dubey2 1 Senior Resident, Department of Dentistry, Anugrah Narayan Magadh Medical College and Hospital, Gaya, Bihar, India 2 Senior Resident, Department of Dentistry, Sri Krishna Medical College and Hospital, Muzaffarpur, Bihar, India * Corresponding Author: Dr. Richa Dubey Abstract Panoramic radiography is often the first choice method for the placement of implants because it provides information on the overall shape of the jaws, the position of the maxillary sinus floor and the nasal cavity floor, and the proximal distal as well as vertical position of the mandibular canal and the mental foramen. The measurements on digital radiography are quite acceptable and reliable for clinical use as long as the structures do not traverse the midline. Repeated measurements lead to a reduction in the systematic error and magnification to a loss of accuracy. The study was planned on the Department of Dentistry Anugrah Narayan Magadh Medical College and Hospital, Gaya.on 30 implants in the posterior mandibular regions. The digital panoramic radiographic images were taken using implants in the posterior mandibular regions. The digital panoramic radiographic equipment used. All digital panoramic radiographs were taken by technicians according to standard protocol provided by the manufacturer. This study is aimed to determine the accuracy of the vertical and horizontal measurements on digital panoramic radiographic images using implants in the posterior mandibular regions. -

Morfofunctional Structure of the Skull
N.L. Svintsytska V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 Ministry of Public Health of Ukraine Public Institution «Central Methodological Office for Higher Medical Education of MPH of Ukraine» Higher State Educational Establishment of Ukraine «Ukranian Medical Stomatological Academy» N.L. Svintsytska, V.H. Hryn Morfofunctional structure of the skull Study guide Poltava 2016 2 LBC 28.706 UDC 611.714/716 S 24 «Recommended by the Ministry of Health of Ukraine as textbook for English- speaking students of higher educational institutions of the MPH of Ukraine» (minutes of the meeting of the Commission for the organization of training and methodical literature for the persons enrolled in higher medical (pharmaceutical) educational establishments of postgraduate education MPH of Ukraine, from 02.06.2016 №2). Letter of the MPH of Ukraine of 11.07.2016 № 08.01-30/17321 Composed by: N.L. Svintsytska, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor V.H. Hryn, Associate Professor at the Department of Human Anatomy of Higher State Educational Establishment of Ukraine «Ukrainian Medical Stomatological Academy», PhD in Medicine, Associate Professor This textbook is intended for undergraduate, postgraduate students and continuing education of health care professionals in a variety of clinical disciplines (medicine, pediatrics, dentistry) as it includes the basic concepts of human anatomy of the skull in adults and newborns. Rewiewed by: O.M. Slobodian, Head of the Department of Anatomy, Topographic Anatomy and Operative Surgery of Higher State Educational Establishment of Ukraine «Bukovinian State Medical University», Doctor of Medical Sciences, Professor M.V. -

Chapter 2 Implants and Oral Anatomy
Chapter 2 Implants and oral anatomy Associate Professor of Maxillofacial Anatomy Section, Graduate School of Medical and Dental Sciences, Tokyo Medical and Dental University Tatsuo Terashima In recent years, the development of new materials and improvements in the operative methods used for implants have led to remarkable progress in the field of dental surgery. These methods have been applied widely in clinical practice. The development of computerized medical imaging technologies such as X-ray computed tomography have allowed detailed 3D-analysis of medical conditions, resulting in a dramatic improvement in the success rates of operative intervention. For treatment with a dental implant to be successful, it is however critical to have full knowledge and understanding of the fundamental anatomical structures of the oral and maxillofacial regions. In addition, it is necessary to understand variations in the topographic and anatomical structures among individuals, with age, and with pathological conditions. This chapter will discuss the basic structure of the oral cavity in relation to implant treatment. I. Osteology of the oral area The oral cavity is composed of the maxilla that is in contact with the cranial bone, palatine bone, the mobile mandible, and the hyoid bone. The maxilla and the palatine bones articulate with the cranial bone. The mandible articulates with the temporal bone through the temporomandibular joint (TMJ). The hyoid bone is suspended from the cranium and the mandible by the suprahyoid and infrahyoid muscles. The formation of the basis of the oral cavity by these bones and the associated muscles makes it possible for the oral cavity to perform its various functions. -

Lab Manual Axial Skeleton Atla
1 PRE-LAB EXERCISES When studying the skeletal system, the bones are often sorted into two broad categories: the axial skeleton and the appendicular skeleton. This lab focuses on the axial skeleton, which consists of the bones that form the axis of the body. The axial skeleton includes bones in the skull, vertebrae, and thoracic cage, as well as the auditory ossicles and hyoid bone. In addition to learning about all the bones of the axial skeleton, it is also important to identify some significant bone markings. Bone markings can have many shapes, including holes, round or sharp projections, and shallow or deep valleys, among others. These markings on the bones serve many purposes, including forming attachments to other bones or muscles and allowing passage of a blood vessel or nerve. It is helpful to understand the meanings of some of the more common bone marking terms. Before we get started, look up the definitions of these common bone marking terms: Canal: Condyle: Facet: Fissure: Foramen: (see Module 10.18 Foramina of Skull) Fossa: Margin: Process: Throughout this exercise, you will notice bold terms. This is meant to focus your attention on these important words. Make sure you pay attention to any bold words and know how to explain their definitions and/or where they are located. Use the following modules to guide your exploration of the axial skeleton. As you explore these bones in Visible Body’s app, also locate the bones and bone markings on any available charts, models, or specimens. You may also find it helpful to palpate bones on yourself or make drawings of the bones with the bone markings labeled. -

Morphometric Analysis of Chin Shape in Inverted Mandible and Mid Symphysis Menti Angle
Dental Communication Biosc.Biotech.Res.Comm. Special Issue Vol 13 No 8 2020 Pp-104-107 Morphometric Analysis of Chin Shape in Inverted Mandible and Mid Symphysis Menti Angle Sachin Aditya B1 and Yuvaraj Babu K2* 1Saveetha Dental college and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai - 600077, India 2Assistant professor, Department of Anatomy, Saveetha Dental college and Hospitals, Saveetha Institute of Medical and Technical Sciences, Saveetha University, Chennai - 600077, India ABSTRACT In human anatomy, the skull 's facial skeleton, the outer surface of the mandible, is distinguished by a slight ridge in the median line, suggesting the mandibular symphysis or junction line in which the two lateral halves of the mandible usually unite at an early life (1-2 years). This is not a true symphysis, since there is no cartilage between the mandible's two hands. The main aim of the study is to measure the mid symphysis menti angle in the inverted aspect. 30 unsexed dry human skulls were taken from the Department of Anatomy, Saveetha Dental College and Hospital. Protractor was used to measure the mid symphysis menti angle in the inverted aspect of the mandible. The average measurement of mid symphysis menti angle was 76.16° and the shape of the mental protuberance for most of the samples were oval shaped. Our study has tried to analyse the mid symphysis menti angle and chin shape in the inverted aspect of mandibles, this data may be useful for surgeons in planning their surgery in the mandibular region. KEY WORDS: MID SYMPHYSIS MENTI ANGLE, MENtaL PROTUBERANCE, MANDIBLE, CHIN SHAPE. -
The Axial Skeleton Visual Worksheet
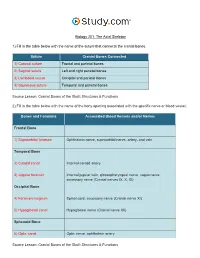
Biology 201: The Axial Skeleton 1) Fill in the table below with the name of the suture that connects the cranial bones. Suture Cranial Bones Connected 1) Coronal suture Frontal and parietal bones 2) Sagittal suture Left and right parietal bones 3) Lambdoid suture Occipital and parietal bones 4) Squamous suture Temporal and parietal bones Source Lesson: Cranial Bones of the Skull: Structures & Functions 2) Fill in the table below with the name of the bony opening associated with the specific nerve or blood vessel. Bones and Foramina Associated Blood Vessels and/or Nerves Frontal Bone 1) Supraorbital foramen Ophthalmic nerve, supraorbital nerve, artery, and vein Temporal Bone 2) Carotid canal Internal carotid artery 3) Jugular foramen Internal jugular vein, glossopharyngeal nerve, vagus nerve, accessory nerve (Cranial nerves IX, X, XI) Occipital Bone 4) Foramen magnum Spinal cord, accessory nerve (Cranial nerve XI) 5) Hypoglossal canal Hypoglossal nerve (Cranial nerve XII) Sphenoid Bone 6) Optic canal Optic nerve, ophthalmic artery Source Lesson: Cranial Bones of the Skull: Structures & Functions 3) Label the anterior view of the skull below with its correct feature. Frontal bone Palatine bone Ethmoid bone Nasal septum: Perpendicular plate of ethmoid bone Sphenoid bone Inferior orbital fissure Inferior nasal concha Maxilla Orbit Vomer bone Supraorbital margin Alveolar process of maxilla Middle nasal concha Inferior nasal concha Coronal suture Mandible Glabella Mental foramen Nasal bone Parietal bone Supraorbital foramen Orbital canal Temporal bone Lacrimal bone Orbit Alveolar process of mandible Superior orbital fissure Zygomatic bone Infraorbital foramen Source Lesson: Facial Bones of the Skull: Structures & Functions 4) Label the right lateral view of the skull below with its correct feature. -

Variation in Chin and Mandibular Symphysis Size and Shape in Males and Females: a CT-Based Study
International Journal of Environmental Research and Public Health Article Variation in Chin and Mandibular Symphysis Size and Shape in Males and Females: A CT-Based Study Tatiana Sella Tunis 1,2,3,* , Israel Hershkovitz 1,2 , Hila May 1,2, Alexander Dan Vardimon 3, Rachel Sarig 2,3,4 and Nir Shpack 3 1 Department of Anatomy and Anthropology, Sackler Faculty of Medicine, Tel Aviv University, Ramat Aviv 69978, Israel; [email protected] (I.H.); [email protected] (H.M.) 2 Dan David Center for Human Evolution and Biohistory Research, Shmunis Family Anthropology Institute, Sackler Faculty of Medicine, Tel Aviv University, Ramat Aviv 69978, Israel; [email protected] 3 Department of Orthodontics, The Maurice and Gabriela Goldschleger School of Dental Medicine, Sackler Faculty of Medicine, Tel Aviv University, Ramat Aviv 69978, Israel; [email protected] (A.D.V.); [email protected] (N.S.) 4 Department of Oral Biology, The Maurice and Gabriela Goldschleger School of Dental Medicine, Sackler Faculty of Medicine, Tel Aviv University, Ramat Aviv 69978, Israel * Correspondence: [email protected]; Tel.: +972-3-640-7310 Received: 12 May 2020; Accepted: 11 June 2020; Published: 14 June 2020 Abstract: The chin is a unique anatomical landmark of modern humans. Its size and shape play an important role from the esthetic perspective. However, disagreement exists in the dental and anthropological literature regarding the sex differences in chin and symphysis morphometrics. The “sexual selection” theory is presented as a possible reason for chin formation in our species; however, many other contradictory theories also exist. -

1 TERMINOLOGIA ANTHROPOLOGICA Names of The
TERMINOLOGIA ANTHROPOLOGICA Names of the parts of the human body, terms of aspects and relationships, and osteological terminology are as in Terminologia Anatomica. GENERAL TERMS EXPLANANTION ADAPTATION Adjustment and change of an organism to a specific environment, due primarily to natural selection. ADAPTIVE RADIATION Divergence of an ancestral population through adaption and speciation into a number of ecological niches. ADULT Fully developed and mature individual ANAGENESIS The progressive adaption of a single evolutionary line, where the population becomes increasingly specialized to a niche that has remained fairly constant through time. ANCESTRY One’s family or ethnic descent, the evolutionary or genetic line of descent of an animal or plant / Ancestral descent or lineage ANTEMORTEM Biological processes that can result in skeletal modifications before death ANTHROPOCENTRICISM The belief that humans are the most important elements in the universe. ANTHROPOLOGY The study of human biology and behavior in the present and in the past ANTHROPOLOGIST BIOLOGICAL A specialist in the subfield of anthropology that studies humans as a biological species FORENSIC A specialist in the use of anatomical structures and physical characteristics to identify a subject for legal purposes PHYSICAL A specialist in the subfield of anthropology dealing with evolutionary changes in the human bodily structure and the classification of modern races 1 SOCIAL A specialist in the subfield of anthropology that deals with cultural and social phenomena such as kingship systems or beliefs ANTHROPOMETRY The study of human body measurement for use in anthropological classification and comparison ARCHETYPE That which is taken as the blueprint for a species or higher taxonomic category ARTIFACT remains of past human activity. -

Splanchnocranium
splanchnocranium - Consists of part of skull that is derived from branchial arches - The facial bones are the bones of the anterior and lower human skull Bones Ethmoid bone Inferior nasal concha Lacrimal bone Maxilla Nasal bone Palatine bone Vomer Zygomatic bone Mandible Ethmoid bone The ethmoid is a single bone, which makes a significant contribution to the middle third of the face. It is located between the lateral wall of the nose and the medial wall of the orbit and forms parts of the nasal septum, roof and lateral wall of the nose, and a considerable part of the medial wall of the orbital cavity. In addition, the ethmoid makes a small contribution to the floor of the anterior cranial fossa. The ethmoid bone can be divided into four parts, the perpendicular plate, the cribriform plate and two ethmoidal labyrinths. Important landmarks include: • Perpendicular plate • Cribriform plate • Crista galli. • Ala. • Ethmoid labyrinths • Medial (nasal) surface. • Orbital plate. • Superior nasal concha. • Middle nasal concha. • Anterior ethmoidal air cells. • Middle ethmoidal air cells. • Posterior ethmoidal air cells. Attachments The falx cerebri (slide) attaches to the posterior border of the crista galli. lamina cribrosa 1 crista galli 2 lamina perpendicularis 3 labyrinthi ethmoidales 4 cellulae ethmoidales anteriores et posteriores 5 lamina orbitalis 6 concha nasalis media 7 processus uncinatus 8 Inferior nasal concha Each inferior nasal concha consists of a curved plate of bone attached to the lateral wall of the nasal cavity. Each consists of inferior and superior borders, medial and lateral surfaces, and anterior and posterior ends. The superior border serves to attach the bone to the lateral wall of the nose, articulating with four different bones. -
Axial Skeleton 214 7.7 Development of the Axial Skeleton 214
SKELETAL SYSTEM OUTLINE 7.1 Skull 175 7.1a Views of the Skull and Landmark Features 176 7.1b Sutures 183 7.1c Bones of the Cranium 185 7 7.1d Bones of the Face 194 7.1e Nasal Complex 198 7.1f Paranasal Sinuses 199 7.1g Orbital Complex 200 Axial 7.1h Bones Associated with the Skull 201 7.2 Sex Differences in the Skull 201 7.3 Aging of the Skull 201 Skeleton 7.4 Vertebral Column 204 7.4a Divisions of the Vertebral Column 204 7.4b Spinal Curvatures 205 7.4c Vertebral Anatomy 206 7.5 Thoracic Cage 212 7.5a Sternum 213 7.5b Ribs 213 7.6 Aging of the Axial Skeleton 214 7.7 Development of the Axial Skeleton 214 MODULE 5: SKELETAL SYSTEM mck78097_ch07_173-219.indd 173 2/14/11 4:58 PM 174 Chapter Seven Axial Skeleton he bones of the skeleton form an internal framework to support The skeletal system is divided into two parts: the axial skele- T soft tissues, protect vital organs, bear the body’s weight, and ton and the appendicular skeleton. The axial skeleton is composed help us move. Without a bony skeleton, we would collapse into a of the bones along the central axis of the body, which we com- formless mass. Typically, there are 206 bones in an adult skeleton, monly divide into three regions—the skull, the vertebral column, although this number varies in some individuals. A larger number of and the thoracic cage (figure 7.1). The appendicular skeleton bones appear to be present at birth, but the total number decreases consists of the bones of the appendages (upper and lower limbs), with growth and maturity as some separate bones fuse. -

Skull / Cranium
Important! 1. Memorizing these pages only does not guarantee the succesfull passing of the midterm test or the semifinal exam. 2. The handout has not been supervised, and I can not guarantee, that these pages are absolutely free from mistakes. If you find any, please, report to me! SKULL / CRANIUM BONES OF THE NEUROCRANIUM (7) Occipital bone (1) Sphenoid bone (1) Temporal bone (2) Frontal bone (1) Parietal bone (2) BONES OF THE VISCEROCRANIUM (15) Ethmoid bone (1) Maxilla (2) Mandible (1) Zygomatic bone (2) Nasal bone (2) Lacrimal bone (2) Inferior nasalis concha (2) Vomer (1) Palatine bone (2) Compiled by: Dr. Czigner Andrea 1 FRONTAL BONE MAIN PARTS: FRONTAL SQUAMA ORBITAL PARTS NASAL PART FRONTAL SQUAMA Parietal margin Sphenoid margin Supraorbital margin External surface Frontal tubercle Temporal surface Superciliary arch Zygomatic process Glabella Supraorbital margin Frontal notch Supraorbital foramen Internal surface Frontal crest Sulcus for superior sagittal sinus Foramen caecum ORBITAL PARTS Ethmoidal notch Cerebral surface impresiones digitatae Orbital surface Fossa for lacrimal gland Trochlear notch / fovea Anterior ethmoidal foramen Posterior ethmoidal foramen NASAL PART nasal spine nasal margin frontal sinus Compiled by: Dr. Czigner Andrea 2 SPHENOID BONE MAIN PARTS: CORPUS / BODY GREATER WINGS LESSER WINGS PTERYGOID PROCESSES CORPUS / BODY Sphenoid sinus Septum of sphenoid sinus Sphenoidal crest Sphenoidal concha Apertura sinus sphenoidalis / Opening of sphenoid sinus Sella turcica Hypophyseal fossa Dorsum sellae Posterior clinoid process Praechiasmatic sulcus Carotid sulcus GREATER WINGS Cerebral surface • Foramen rotundum • Framen ovale • Foramen spinosum Temporal surface Infratemporalis crest Infratemporal surface Orbital surface Maxillary surface LESSER WINGS Anterior clinoid process Superior orbital fissure Optic canal PTERYGOID PROCESSES Lateral plate Medial plate Pterygoid hamulus Pterygoid fossa Pterygoid sulcus Scaphoid fossa Pterygoid notch Pterygoid canal (Vidian canal) Compiled by: Dr. -

Split Fracture and Displacement of Mandibular Lingual Cortical Plate of Mandibular Symphysis Requires Fixation Masaki Fujioka1*, Kenji Hayashida2 and Hiroto Saijo2
Fujioka et al. Trauma Cases Rev 2015, 1:4 ISSN: 2469-5777 Trauma Cases and Reviews Case Report: Open Access Split Fracture and Displacement of Mandibular Lingual Cortical Plate of Mandibular Symphysis Requires Fixation Masaki Fujioka1*, Kenji Hayashida2 and Hiroto Saijo2 1Clinical Professor, Department of Plastic and Reconstructive Surgery, Nagasaki University, Nagasaki, Japan 2Staff surgeon, Department of Plastic and Reconstructive Surgery, National Hospital Organization Nagasaki Medical Center, Japan *Corresponding author: Masaki Fujioka, Clinical Professor, Department of Plastic and Reconstructive Surgery, Nagasaki University, Nagasaki, and Director of the Department of Plastic and Reconstructive Surgery, Clinical Research Center, National Hospital Organization Nagasaki Medical Center, Nagasaki, Japan, E-mail: [email protected] complaining of marked neck swelling and airway obstruction Abstract resulting from a car accident. As the patient had extensive oral The first priority in the management of comminuted mandibular bleeding, he immediately underwent intra-tracheal intubation. An fractures is the prevention of acute upper airway obstruction. emergent cerebral angiogram revealed extravasation of the mental Each division of mandibular fractures may cause respiratory artery; thus, transcatheter arterial embolization was performed. obstruction. Among the variety of such fractures, split fracture of the Computed tomography (CT) showed both maxillary and mandibular symphyseal lingual cortical plate has a significant influence on the oropharyngeal and laryngopharyngeal airway spaces, and causes open fractures (Figure 1a). The menton had fractured into pieces, a markedly restricted ventilatory function. As the bony fragment is pedicled to the geniohyoid and genioglossus muscles, this type of fracture restricts hyoid movements, which may result in disturbance of deglutition. We present two cases of split fracture and displacement of the mandibular lingual cortical plate of the mandibular symphysis, which were successfully treated with open reduction.