Comparison of Differential Pulse Voltammetry (DPV)— a New Method of Carbamazepine Analysis—With Fluorescence Polarization Immunoassay (FPIA)1 H
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Chapter 3: Experimental
Chapter 3: Experimental CHAPTER 3: EXPERIMENTAL 3.1 Basic concepts of the experimental techniques In this part of the chapter, a short overview of some phrases and theoretical aspects of the experimental techniques used in this work are given. Cyclic voltammetry (CV) is the most common technique to obtain preliminary information about an electrochemical process. It is sensitive to the mechanism of deposition and therefore provides informations on structural transitions, as well as interactions between the surface and the adlayer. Chronoamperometry is very powerful method for the quantitative analysis of a nucleation process. The scanning tunneling microscopy (STM) is based on the exponential dependence of the tunneling current, flowing from one electrode onto another one, depending on the distance between electrodes. Combination of the STM with an electrochemical cell allows in-situ study of metal electrochemical phase formation. XPS is also a very powerfull technique to investigate the chemical states of adsorbates. Theoretical background of these techniques will be given in the following pages. At an electrode surface, two fundamental electrochemical processes can be distinguished: 3.1.1 Capacitive process Capacitive processes are caused by the (dis-)charge of the electrode surface as a result of a potential variation, or by an adsorption process. Capacitive current, also called "non-faradaic" or "double-layer" current, does not involve any chemical reactions (charge transfer), it only causes accumulation (or removal) of electrical charges on the electrode and in the electrolyte solution near the electrode. There is always some capacitive current flowing when the potential of an electrode is changing. In contrast to faradaic current, capacitive current can also flow at constant 28 Chapter 3: Experimental potential if the capacitance of the electrode is changing for some reason, e.g., change of electrode area, adsorption or temperature. -

Hydrodynamic Voltammetry As a Rapid and Simple Method for Evaluating Soil Enzyme Activities
Sensors 2015, 15, 5331-5343; doi:10.3390/s150305331 OPEN ACCESS sensors ISSN 1424-8220 www.mdpi.com/journal/sensors Article Hydrodynamic Voltammetry as a Rapid and Simple Method for Evaluating Soil Enzyme Activities Kazuto Sazawa 1,* and Hideki Kuramitz 2 1 Center for Far Eastern Studies, University of Toyama, Gofuku 3190, 930-8555 Toyama, Japan 2 Department of Environmental Biology and Chemistry, Graduate School of Science and Engineering for Research, University of Toyama, Gofuku 3190, 930-8555 Toyama, Japan; E-Mail: [email protected] * Author to whom correspondence should be addressed; E-Mail: [email protected]; Tel./Fax: +81-76-445-66-69. Academic Editor: Ki-Hyun Kim Received: 26 December 2014 / Accepted: 28 February 2015 / Published: 4 March 2015 Abstract: Soil enzymes play essential roles in catalyzing reactions necessary for nutrient cycling in the biosphere. They are also sensitive indicators of ecosystem stress, therefore their evaluation is very important in assessing soil health and quality. The standard soil enzyme assay method based on spectroscopic detection is a complicated operation that requires the removal of soil particles. The purpose of this study was to develop a new soil enzyme assay based on hydrodynamic electrochemical detection using a rotating disk electrode in a microliter droplet. The activities of enzymes were determined by measuring the electrochemical oxidation of p-aminophenol (PAP), following the enzymatic conversion of substrate-conjugated PAP. The calibration curves of β-galactosidase (β-gal), β-glucosidase (β-glu) and acid phosphatase (AcP) showed good linear correlation after being spiked in soils using chronoamperometry. -

Square Wave Voltammetry
Application Note S-7 Subject: Square Wave Voltammetry INTRODUCTION reverse pulse of the square wave occurs half way through the staircase step. The primary advantage of the pulse voltammetric techniques, such as normal pulse or differential pulse voltammetry, is their ability to discriminate against charging (capacitance) current. As a result, the pulse techniques are more sensitive to oxidation or reduction currents (faradaic currents) than conventional dc PLUS voltammetry. Differential pulse voltammetry yields peaks for faradaic currents rather than the sigmoidal waveform obtained with dc or normal pulse techniques. This results in improved resolution for multiple analyte systems and more convenient quantitation. Square wave voltammetry has received growing attention as a voltammetric technique for routine quantitative analyses. Although square wave voltammetry was E reported as long ago as 1957 by Barker1, the utility of the EQUALS technique was limited by electronic technology. Recent advances in both analog and digital electronics have made it feasible to incorporate square wave voltammetry into the PAR Model 394 Polarographic Analyzer. Square wave voltammetry can be used to perform an experiment much faster than normal and differential pulse techniques, which typically run at scan rates of 1 to 10 mV/sec. Square wave voltammetry employs scan rates TIME up to 1 V/sec or faster, allowing much faster determinations. A typical experiment requiring three minutes by normal or differential pulse techniques can be performed in a matter of seconds by square wave voltammetry. FIGURE 1: Applied excitation in square wave voltammetry. THEORY The timing and applied potential parameters for square The waveform used for square wave voltammetry is wave voltammetry are depicted in Figure 2. -

Reaction Mechanism of Electrochemical Oxidation of Coo/Co(OH)2 William Prusinski Valparaiso University
Valparaiso University ValpoScholar Chemistry Honors Papers Department of Chemistry Spring 2016 Solar Thermal Decoupled Electrolysis: Reaction Mechanism of Electrochemical Oxidation of CoO/Co(OH)2 William Prusinski Valparaiso University Follow this and additional works at: http://scholar.valpo.edu/chem_honors Part of the Physical Sciences and Mathematics Commons Recommended Citation Prusinski, William, "Solar Thermal Decoupled Electrolysis: Reaction Mechanism of Electrochemical Oxidation of CoO/Co(OH)2" (2016). Chemistry Honors Papers. 1. http://scholar.valpo.edu/chem_honors/1 This Departmental Honors Paper/Project is brought to you for free and open access by the Department of Chemistry at ValpoScholar. It has been accepted for inclusion in Chemistry Honors Papers by an authorized administrator of ValpoScholar. For more information, please contact a ValpoScholar staff member at [email protected]. William Prusinski Honors Candidacy in Chemistry: Final Report CHEM 498 Advised by Dr. Jonathan Schoer Solar Thermal Decoupled Electrolysis: Reaction Mechanism of Electrochemical Oxidation of CoO/Co(OH)2 College of Arts and Sciences Valparaiso University Spring 2016 Prusinski 1 Abstract A modified water electrolysis process has been developed to produce H2. The electrolysis cell oxidizes CoO to CoOOH and Co3O4 at the anode to decrease the amount of electric work needed to reduce water to H2. The reaction mechanism through which CoO becomes oxidized was investigated, and it was observed that the electron transfer occurred through both a species present in solution and a species adsorbed to the electrode surface. A preliminary mathematical model was established based only on the electron transfer to species in solution, and several kinetic parameters of the reaction were calculated. -

Redox Potential Measurements M.J
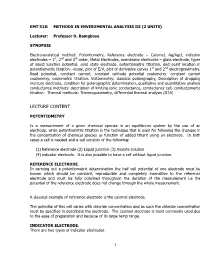
Redox Potential Measurements M.J. Vepraskas NC State University December 2002 Redox potential is an electrical measurement that shows the tendency of a soil solution to transfer electrons to or from a reference electrode. From this measurement we can estimate whether the soil is aerobic, anaerobic, and whether chemical compounds such as Fe oxides or nitrate have been chemically reduced or are present in their oxidized forms. Making these measurements requires three basic pieces of equipment: 1. Platinum electrode 2. Voltmeter 3. Reference electrode The basic set-up is shown below: Voltmeter 456 mv Soil surface Reference Pt wire electrode Fig. 1. The Pt wire is buried into the soil to be in contact with the soil solution. The reference electrode must also be in contact with the soil solution. It has a ceramic tip, which can be placed in the soil, or the electrode can be placed in a salt bridge, which is itself placed in the soil. Wires from both the Pt electrode and reference electrode are connected to the voltmeter. Pt Electrodes Platinum electrodes consist of a small piece of platinum wire that is soldered or fused to wire made another metal. Platinum conducts electrons from the soil solution to the wire to which it is attached. Platinum is used because it is assumed to be an inert metal. This means it does not give up its own electrons (does not oxidize) to the wire or soil solution. Iron containing materials such as steel will oxidize themselves and send their own electrons to the voltmeter. As a result the voltage we measure will not result solely from electrons being transferred to or from the soil. -

Using Chronoamperometry to Rapidly Measure and Quantitatively Analyse Rate- Performance in Battery Electrodes
Using chronoamperometry to rapidly measure and quantitatively analyse rate- performance in battery electrodes Ruiyuan Tian,1,2 Paul J. King,3 Joao Coelho,2,4 Sang-Hoon Park,2,4 Dominik V Horvath,1,2 Valeria Nicolosi,2,4 Colm O’Dwyer,2,5 Jonathan N Coleman1,2* 1School of Physics, Trinity College Dublin, Dublin 2, Ireland 2AMBER Research Center, Trinity College Dublin, Dublin 2, Ireland 3Efficient Energy Transfer Department, Bell Labs Research, Nokia, Blanchardstown Business & Technology Park, Snugborough Road, Fingal, Dublin 15, Ireland 4School of Chemistry, Trinity College Dublin, Dublin 2, Ireland 5 School of Chemistry, University College Cork, Tyndall National Institute, and Environmental Research Institute, Cork T12 YN60, Ireland *[email protected] (Jonathan N. Coleman); Tel: +353 (0) 1 8963859. ABSTRACT: For battery electrodes, measured capacity decays as charge/discharge current is increased. Such rate-performance is important from a practical perspective and is usually characterised via galvanostatic charge-discharge measurements. However, such measurements are very slow, limiting the number of rate experiments which are practical in a given project. This is a particular problem during mechanistic studies where many rate measurements are needed. Here, building on work by Heubner at al., we demonstrate chronoamperometry (CA) as a relatively fast method for measuring capacity-rate curves with hundreds of data points down to C-rates below 0.01C. While Heubner et al. reported equations to convert current transients to capacity vs. C-rate curves, we modify these equations to give capacity as a function of charge/discharge rate, R. We show that such expressions can be combined with a basic model to obtain simple equations which can fit data for both capacity vs. -
Lecture Content
EMT 518: METHODS IN ENVIROMENTAL ANALYSIS III (2 UNITS) Lecturer: Professor O. Bamgbose SYNOPSIS Electro-analytical method: Potentiometry, Reference electrode – Calomel, Ag/Agcl, indicator electrodes – 1st, 2nd and 3rd order, Metal Electrodes, membrane electrodes – glass electrode, types of liquid junction potential, solid state electrode, potentiometric titration, end point location in potentiometric titration –visual, plot of E/V, plot of derivative curves 1st and 2nd electrogravimetry, fixed potential, constant current, constant cathode potential coulometry: constant current coulometry, coulometric titration. Voltammetry: classical polarography, Description of dropping mercury electrode, condition for polarographic determination, qualitative and quantitative analysis conductance methods: description of limiting ionic conductance, conductance cell, conductomertic titration. Thermal methods: Thermogravimetry, differential thermal analysis (DTA) LECTURE CONTENT POTENTIOMETRY Is a measurement of a given chemical species in an equilibrium system by the use of an electrode, while potentiometric titration is the technique that is used for following the changes in the concentration of chemical species as function of added titrant using an electrode. In both cases a cell is needed and a cell consists of the following: (1) Reference electrode (2) Liquid junction (3) Analyte solution (4) indicator electrode. It is also possible to have a cell without liquid junction. REFERENCE ELECTRODE. In carrying out a potentiometric determination the half cell potential of one electrode must be known which should be constant, reproducible and completely insensitive to the reference electrode and must be fully polarised throughout the duration of the measurement i.e the potential of the reference electrode does not change through the whole measurement. A classical example of reference electrode is the calomel electrode. -

Stationary Electrode Voltammetry and Chronoamperometry in an Alkali Metal Carbonate-Borate Melt
AN ABSTRACT OF THE THESIS OF DARRELL GEORGE PETCOFF for the Doctor of Philosophy (Name of student) (Degree) in Analytical Chemistry presented onC (O,/97 (Major) (Date) Title: STATIONARY ELECTRODE VOLTAMMETRY AND CHRONOAMPEROMETRY IN AN ALKALI METAL CARBONATE - BORATE. MFT T Abstract approved: Redacted for Privacy- Drir. reund The electrochemistry of the lithium-potassium-sodium carbonate-borate melt was explored by voltammetry and chrono- amperometry. In support of this, a controlled-potential polarograph and associated hardware was constructed.Several different types of reference electrodes were tried before choosing a porcelain mem- brane electrode containing a silver wire immersed in a silver sulfate melt.The special porcelain compounded was used also to construct a planar gold disk electrode.The theory of stationary electrode polarography was summarized and denormalized to provide an over- all view. A new approach to the theory of the cyclic background current was also advanced. A computer program was written to facilitate data processing.In addition to providing peak potentials, currents, and n-values, the program also resolves overlapping peaks and furnishes plots of both processed and unprocessed data. Rapid-scan voltammetry was employed to explore the electro- chemical behavior of Zn, Co, Fe, Tl, Sb, As, Ni, Sn, Cd, Te, Bi, Cr, Pb, Cu, and U in the carbonate-borate melt. Most substances gave reasonably well-defined peaks with characteristic peak potentials and n-values.Metal deposition was commonly accompanied by adsorp- tion prepeaks indicative of strong adsorption, and there was also evi- dence of a preceding chemical reaction for several elements, sug- gesting decomplexation before reduction. -

Microfluidic Reference Electrode for Applications
MICROFLUIDIC REFERENCE ELECTRODES FOR APPLICATIONS IN BIOSENSING S. Safari-Mohsenabad1, P.R. Selvaganapathy1*, and M.J. Deen2# 1Mechanical Engineering, 2Electrical& Computer Engineering, McMaster University, Hamilton, ON L8S 4L7, Canada ABSTRACT A microfluidic Silver/Silver Chloride (Ag/AgCl) reference electrode was fabricated and operated in various modes. This micro-scale reference electrode design includes all the features of the macro-scale version including, Ag/AgCl elec- trode, inner standard solution and nanoporous membrane separator in a small form factor. This miniature reference elec- trode could also be operated in modes where the liquid junction potential can be stabilized to provide a stable potential. In one such mode, the microfluidic reference electrode with a free diffusion liquid junction shows < 0.1 mV stability over a 100-hour lifespan and no sensitivity to pH and chlorine concentration of the external solution. KEYWORDS: Ag/AgCl reference electrode, free-diffusion liquid junction, microfabrication, microfluidics INTRODUCTION Reference electrodes are used in situations where electrical sensors interface with ionic solutions and are typically used to impose or measure an electric potential in a solution [1]. Reference electrodes are used in many applications including pH sensing, corrosion monitoring, environmental sensing and blood gas analysis [2]. In addition, the reference electrode has a pronounced influence on the measurement accuracy of electrochemical bio-sensors [3], bio-impedance probes [4] and biological field-effect transistors (BioFETs) [5], especially for low analyte concentrations. For example, a reference electrode is used to impose a bias voltage on the gate of a BioFET that has been functionalized with a biorecognition probe molecule such as a DNA [6]. -

Assessment of an Ultramicroelectrode Array (UMEA) Sensor for The
Assessmentofanultramicroelectrodearray(UMEA)sensorfor thedeterminationoftraceconcentrationsofheavymetalsinwater ZurErlangungdesakademischenGradeseines DoktorsderNaturwissenschaften anderFakultätfürBauingenieur-,Geo-undUmweltwissenschaften der UniversitätKarlsruhe genehmigte DISSERTATION von XudongXie ausVRChina 2004 TagdermündlichenPrüfung:02.06.2004 Referentin:Prof.Dr.DorisStüben Korreferent:Prof.Dr.Rolf-DieterWilken Abstract Abstract Rapid development in silicon technology and microelectronics has nowadays enabled the mass fabrication of microelectrode arrays with well-defined and reproduciblegeometriesonmicronscalesbyusingthin-filmtechnology.Comparedto conventional macroelectrodes, microelectrodes possess several attractive features, suchashighmasstransport,reducedchargingcurrent,immunitytoohmicdrop,high signal-to-noiseratio,etc.,whichareveryadvantageousfordevelopingdecentralised analyticalequipmentsintracemetalanalysis. A novel iridium-based ultramicroelectrode array chip (Ir-UMEAs) was recently designed and fabricated by means of microlithographic techniques by one of the partners (Fraunhofer Institute of Silicon Technology, ISIT, Germany) of this joint research project. The Ir-UMEA chip is made up of 4048 individual ultramicroelectrodes (working electrodes) arranged in four separate arrays. Each arrayconsistsof46x22=1012discshapedmicroelectrodeswithadiameterof1.8 µmeach,givingatotalelectrodeareaof2575µm².Theelectrodesarerecessedby 0.2µmandarespacedwithaninterelectrodedistanceof25µm. Thisstudyismainlyaimedat(i)investigatingtheelectrochemicalbehaviorandthe -

Electrochemical Instrumentation
Electrochemical Instrumentation ______________________________________________________________________________ CH Instruments 1 Overview CH Instruments was established in 1994. Our first instrument series, the Model 600 series electrochemical analyzer/workstation, was introduced at the end of 1994. Since then, new products have been added to provide a full line of electrochemical instrumentation: Model 400A Series Time-Resolved Electrochemical Quartz Crystal Microbalance (EQCM): for electro-deposition, adsorption, and chemical and biological sensor studies. Model 600D Series Potentiostat/Galvanostat: for general purpose electrochemical measurements, such as kinetic measurements, electroanalysis, fundamental research, corrosion, and battery studies. Model 700D Series Bipotentiostat: for rotating ring-disk electrodes (RRDE) and other cases where dual channel measurements are essential. Model 800C Series Electrochemical Detector: for either single or dual channel electrochemical detection of flow cell, capillary electrophoresis and liquid chromatography, for chemical and biological sensors, and conventional electroanalysis. Model 920C Scanning Electrochemical Microscope (SECM): for electrode surface, corrosion, biological samples, solid dissolution, liquid/liquid interfaces and membranes studies. Model 1000A Series Multi-potentiostat: 8-channel potentiostat for array electrode characterization and sensor studies. It can be used for eight independent cells or for eight working electrodes in a same solution. Model 1100A Power Potentiostat/Galvanostat: for applications involving higher current and compliance voltage. Model 1200A Handheld Potentiostat/Bipotentiostat: for electroanalysis, sensor studies, and field applications. Model 1550A Pico Liter Solution Dispenser: for making high density and high accuracy solution arrays. All models are controlled by an external PC under the Windows 95/98/NT/Me/2000/XP environment. The instruments are easy to install and use. No plug-in card or other hardware is required on the PC side. -

Quasi-Reference Electrodes in Confined Electrochemical Cells Can
www.nature.com/scientificreports OPEN Quasi-reference electrodes in confned electrochemical cells can result in in situ production of Received: 13 September 2017 Accepted: 15 January 2018 metallic nanoparticles Published: xx xx xxxx Rukshan T. Perera & Jacob K. Rosenstein Nanoscale working electrodes and miniaturized electroanalytical devices are valuable platforms to probe molecular phenomena and perform chemical analyses. However, the inherent close distance of metallic electrodes integrated into a small volume of electrolyte can complicate classical electroanalytical techniques. In this study, we use a scanning nanopipette contact probe as a model miniaturized electrochemical cell to demonstrate measurable side efects of the reaction occurring at a quasi-reference electrode. We provide evidence for in situ generation of nanoparticles in the absence of any electroactive species and we critically analyze the origin, nucleation, dissolution and dynamic behavior of these nanoparticles as they appear at the working electrode. It is crucial to recognize the implications of using quasi-reference electrodes in confned electrochemical cells, in order to accurately interpret the results of nanoscale electrochemical experiments. New insights into nanoscale chemical systems have come hand in hand with experimental techniques that can probe ever-smaller volumes, but traditional physiochemical models cannot necessarily be applied to systems with nanoscale dimensions. Tis fact, combined with the availability of new fabrication methods to prepare nano- scale electrodes and nanoconfned electrochemical devices, has inspired a new branch of study referred to as “nanoelectrochemistry”1–6. Physical size reductions yield important benefts such as reduced background noise, reduced iR drop, and fast mass transport rates, and these features can be used to study phenomena at length scales approaching the dimensions of single molecules7–15.