Southend, Essex & Thurrock (SET) Safeguarding Adults Guidelines
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Chapter 2 Setting the Scene
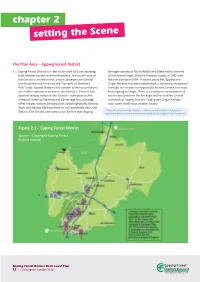
chapter 2 setting the Scene The Plan Area – Epping Forest District 2.1 Epping Forest District is in the south-west of Essex abutting through stations at North Weald and Blake Hall to the end both Greater London and Hertfordshire. The south–west of of the line at Ongar. Blake Hall station closed in 1981 with the District is served by the London Underground Central the line closing in 1994. In recent years the ‘Epping and Line (both the main line and the ‘Hainault via Newbury Ongar Railway’ has been established, a nationally recognised Park’ loop). Epping Station is the eastern terminus and there heritage rail service running on this former Central Line track are 7 other stations in service in the District 1. There is one from Epping to Ongar. There is currently no operational rail national railway station in the District – at Roydon on the connection between the heritage rail line and the Central Liverpool Street to Stansted and Cambridge line, although Line track at Epping, but the ‘Epping and Ongar Railway’ other railway stations (Broxbourne, Sawbridgeworth, Harlow runs some shuttle bus services locally. Town and Harlow Mill) are close to, and accessible from, the 2 District. The Central Line used to run further than Epping, These are Theydon Bois, Debden, Loughton and Buckhurst Hill, together with the stations on the branch line at Roding Valley, Chigwell and Grange Hill Figure 2.1 – Epping Forest District Source – Copyright Epping Forest District Council Epping Forest District Draft Local Plan 12 | Consultation October 2016 2.2 The M25 runs east-west through the District, with a local road 2.6 By 2033, projections suggest the proportion of people aged interchange at Waltham Abbey. -
The Employment Structure in Epping Forest District
The employment structure in Epping Forest District John Papadachi, Prosperica Ltd John Papadachi, Prosperica Ltd Table of Contents Executive summary .................................................................................................... 4 1. Employment in Epping Forest District ..................................................................... 5 1.1 ’Mobile’ ........................................................................................................................... 5 1.2 Dominated by small businesses ...................................................................................... 5 1.3 The high skill-high reward relationship ............................................................................ 6 1.4 ’Traditional’ ..................................................................................................................... 6 1.5 Are these characteristics connected? .............................................................................. 6 2. The district’s employment by sector........................................................................ 7 2.1 Sectoral employment in detail ........................................................................... 9 2.2 Knowledge-based sectors ............................................................................... 11 3. Enterprise ............................................................................................................. 14 3.1 How Epping Forest District performs compared with other areas ................... 14 -

Minutes from the PFCC Thurrock Online Public Meeting
Minutes of the Police, Fire and Crime Commissioner for Essex Thurrock Online Public Meeting 12th May 2020 Panel Members PFCC Roger Hirst, Dep PFCC Jane Gardner, Ch/Insp Richard Melton, Essex Police, Mark Diggory, ECFRS Station Manager Questions Answers A member of the public has consistently reported drug dealing taking place Ch/Insp Melton – drug dealing does not have a place in the district. It brings next door to them and nothing seems to be done. What was the point in all kinds of other crime with it including turf wars and knife crime. reporting? Fortunately, there are not too many rival gangs in Thurrock. The C17 who were operating out of London via county lines in Thurrock has had significant disruption through great activity thanks to the efforts of the Essex Police Op Raptor teams. It is vital people keep reporting in crime as the information is gathered as intelligence and is shared with partners where applicable, to help build a case and achieve a significant prosecution rather than a quick win. He requested for the public to keep the information coming through. How many arrests have been made in Thurrock for public not achieving PFCC – Thurrock FPNs are slightly lower than other areas. Police will only social distancing compared to reports made by the public? respond to gatherings etc in public areas as they cannot enter homes and gardens without a significant reason. To date there has been around 150 fixed penalty notices and only 18 people arrested county wide. Ch/Insp Melton advised the interaction they have had with the public has been largely positive and often just a case of educating around the lockdown measures. -

Ancestors of Phillip Pasfield of Wethersfield, Essex, England
Ancestors of Phillip Pasfield of Wethersfield, Essex, England Phillip Pasfield was born in Wethersfield about 1615 and died in early 1685 in Wethersfield. He lived there his entire life, as did his ancestors going back at least 250 years. This paper will identify and document his known ancestors. Community of Wethersfield Wethersfield is now and always has been a very small community in northwest Essex County. Its history dates back to at least 1190.[1] The earliest known map dated in 1741 shows the roads that connect Wethersfield to other nearby towns and a number of small properties on either side of those roads.[2] Although there are very few Essex County records prior to 1600, Phillip’s ancestors can be traced through them back to the early 1400s in Wethersfield. The surviving parish records in Wethersfield begin about 1650. Fortunately there are wills from 1500 and some land and court records available from the 1300s in the Essex County archives. There are also lawsuits in London Chancery courts that help the genealogical researcher trace Phillip Pasfield and his ancestors. Wethersfield Land Records Land records in early Essex County typically assign names to the various properties rather than use metes and bounds or acres. The assigned property names come from various sources, including names of previous owners of the property. Land transactions typically list the sellers and the buyers, property name, and the neighboring land owners. Many of these properties are bought and sold by groups of individuals who may or may not all be relatives. Because of the lack of wills and available vital records, property ownership plays a critical role in tracing Phillip’s ancestors. -

Valor Park Thurrock157
EASTERN AVENUE I WEST THURROCK I RM20 3LW VALOR PARK THURROCK157 AVAILABLE SUMMER 2019 M25 LOGISTICS OPPORTUNITY 156,958 SQ FT (14,582 SQ M) THURROCK157 is a modern purpose built logistics building constructed in 1999 extending to 156,958 sq ft (GIA), set on a 9-acre site area. Situated in West Thurrock, the largest regeneration area in the UK and fastest growing local economy, the property benefits from excellent transport links HIGH QUALITY and access to the A13 and M25. TO BE FULLY REFURBISHED M6 M6 A1 (M) M65 M62 M62 PORT OF M6 M61 HULL/GRIMSBY/IMMINGHAM M1 A1 (M) M60 MANCHESTER M62 M25 (2 MILES) SHEFFIELD M53 QUEEN ELIZABETH BRIDGE M1 CHESTER CHESTERFIELD A1 (M) LOCAL M6 DARTFORD TUNNEL OCCUPIERS: DRIVE TIMES M1 M54 PETERBOROUGH 0-90 MINS 90-180 MINS 180-270 MINS AMAZON M6 LEICESTER A1 (M) M6 BIRMINGHAM A14 M42 COVENTRY A14 CAMBRIDGE B186 M1 A14 M5 A6 COMMUNICATIONS NORTHAMPTON M40 A1 (M) M25 J31 1 mile Chafford Hundred Station 1.2 miles (walk) VALOR PARK CHELTENHAM M1 M11 LOGISTICS CITY PORT OF MARSTONS/SELCO/SAINT GOBAIN THURROCK157 A12 M5 A1 (M) FElIXSTOWE M25 J30 2 miles OXFORD CHELMSFORD A13 (Mar Dyke Interchange ) 2 miles M40 M25 SWANSEA WEST THURROCK BRISTOL LONDON Tilbury Docks (A13) 8 miles TRADE CITY M25 GATEWAY A282 CARDIFF M4 LONDON TILBURY London Gateway (A13) 11 miles M4 HEATHROW DOCKS HERMES M4 JAMES LATHAM BATH North Circular Rd (A406) 11 miles M5 M25 J13 PARK M3 M25 DOVER London City Airport 14 miles PORT OF DOVER Central London 20 miles M3 Luton International Airport 55 miles M5 SOUTHAMPTON BRIGHTON PORT OF FOLKESTONE -

Economic Growth Plan 2020
Economic Growth Plan 2020 - 2024 DRAFT FOR CONSULTATION Date: October 2020 – Version 21. Contents Foreword ............................................................................................................................................................................................ 3 1. Executive Summary ................................................................................................................................................................. 4 2. Our Vision ................................................................................................................................................................................. 6 3. Measures of Success ............................................................................................................................................................... 6 4. Policy Context ........................................................................................................................................................................... 7 5. Key Priorities ............................................................................................................................................................................ 9 Supporting Business Growth .................................................................................................................................................... 10 Supporting early stage, high growth businesses ................................................................................................................... -

Colchester Campus Map
Colchester Campus Map 1 2 3 4 5 6 7 8 9 10 E A133 Colchester A133 Clacton LM STE CLINGOE HILL AD ROAD Colchester Entrance A133 A Capon Road Car Park BOUNDARY CAPO O N ROAD ROAD D OA D R IEL SF NE Innovation Car Park 21 Lake House B 28 20 P 19 B Quays Bridge 27 1208 CAPON ROAD North Towers Car Park 18 26 D L 31 OA S R ER LIGHTSHIP WAY W O T 17 16 H BBQ Area 29 T R 30 O 14 N J Wivenhoe House Hotel C and Edge Hotel School 25 G 15 24 23 Brightlingsea 27 13 0 12 1 22 B Wivenhoe Park Day Nursery 11 Visitors’ Reception F A Sports Field Health Centre I D B N M Square 5 Wivenhoe Square 4 Entrance E C Valley Car Park Map Key: H Sports Pavilion Square 3 Square 2 Cycle Path Information Centre E Square 1 Cycle Parking All Weather Pitch VALLEY ROAD K D Bus Stop Essex Sport Arena BOUNDARY ROAD Main Road Tennis Courts 10 Main Squares 9 Sports Centre PARK ROAD 8 Car Park A Path Multi-deck Car Park F 28 Wivenhoe Vehicle Barrier 6 0 1 4 B Wivenhoe Trail Car Park B 1 RIVER COLNE 2 7 Area: 3 5 North Campus G B OU Central Campus ND ARY ROAD South Campus Our Learning Spaces Our Art Spaces Student Residences South Towers (9–10) The Houses (16–21) The Meadows (25–30) Disabled Visitors A Albert Sloman Library (D6) M Art Exchange – Gallery (D6) 9 Bertrand Russell (F6) 16 Anne Knight (C5) 25 Cole (C2) For information on access and parking B The Hex (D5) N Lakeside Theatre (D6) South Courts (1–8) 10 Eddington (E6/F6) 17 Swaynes (C5) 26 Arber (C2) arrangements, please contact Visitors’ C Ivor Crewe Lecture Hall (E6) 1 Harwich (F5/G5) 18 Issac Rebow (B5) 27 Godwin -

Unit 1, Southernhay Basildon Essex SS14 1DJ
Unit 1, Southernhay Basildon Essex SS14 1DJ TO LET, BASILDON ESSEX, RETAIL WAREHOUSE/SHOWROOM IN APPROX. 3,000 SQ.FT. Unit 1, Southernhay, Location: Basildon, Essex, SS14 1DJ Basildon is the largest town in the borough of with a growing population of 185,000, and lies 26 miles east of Central London, A striking building in perhaps the most visible location in 11 miles south of Chelmsford and 10 miles West of Southend. Basildon! Purpose built by our Client about 10 years ago and Basildon provides excellent connectivity to Southend, Stansted & offering some 3,000 sq.ft. of showroom/retail space with floor London City airports by train, or by road via the A127, and A13. to ceiling glazed frontage. The town enjoys the highest business growth in South Essex with a working population of some 114,500, and is second only to Iconic Landmark Location Canary Wharf as the largest economy across the entire Thames Retail Warehouse/Showroom Estuary. Approx. 3,000 Sq.Ft. Suit Numerous Similar Uses Property: Population Of 185,000 A purpose built retail Warehouse/Showroom in approx. 3,000 2nd Largest Economy In Thames Estuary sq.ft. Entirely open plan space together with a kitchen/staff mess room with fire escape and staff WC. Shared loading space/occasional parking to the front for up to 5 vehicles. In addition, there is a ‘Pay & Display’ car park to the rear. Max head height 6.12m. Min head height 4.89m. Tenure: To let on a FR&I lease, for a period to be agreed. Rent: £60,000pa + VAT if applicable. -

Announcing the South East Creative, Cultural and Digital Support Programme (SECCADS)
Announcing the South East Creative, Cultural and Digital Support programme (SECCADS) 1 Why are we running the SECCADS Programme? “The Creative Industries are a success story, playing a key role in the UK’s economic recovery. They contributed £87.4bn in GVA in 2015, 5.3% of the UK economy (comparable to the Construction and Information sectors) and between 2010 and 2015 grew by 34% - faster than any other sector. They have also outperformed other sectors in terms of employment growth: between 2011 and 2016, employment in the sector increased by 25.4% (circa 400,000 jobs) compared to 7.6% average across the wider UK. The sector is a net exporter of services (£11.3bn surplus in 2015)” Independent Review of the Creative Industries, Sir Peter Bazalgette 2017 The South East Local Enterprise Partnership (SELEP) wishes to ensure that it supports and benefits from this growth sector. Aware that the Creative, Cultural and Digital Sector does not tend to access mainstream business support, SELEP has supported the South East Creative Economy Network to develop SECCADS. SECCADS is designed to specifically attract and meet the needs of the sector. What is SECCADS? SECCADS will be a two-year business support programme designed to support Creative, Cultural and Digital Businesses (2018 – 2020). There will be three categories of support on offer: • Cluster- it: support to encourage cluster development across the SELEP area and into key markets such as London • Design-it: support for business start-ups in the sector • Grow-it: support for business growth There will be: • Local Coordinators located in each of the three areas: Essex, Kent & Medway and East Sussex. -

(Various Roads, Epping Forest) (Permitted Parking Area and Special Parking Area) (Amendment No.1) Order 201*
The Essex County Council (Various Roads, Epping Forest) (Permitted Parking Area and Special Parking Area) (Amendment No.1) Order 201* Notice is hereby given that Essex County Council proposes to make the above Order under Sections 1(1), 2(1) to (3), 3(2), 4(1), 4(2), 32, 35, 45, 46, 49 and 53 and Parts III and IV of Schedule 9 of the Road Traffic Regulation Act 1984. Effect of the order: To Introduce ‘Disabled Badge Holders Only’ on the following lengths of roads in the District of Epping Forest Road Description Roding Road, SOUTH EAST SIDE - From a point approximately 0.9 metres northeast of Loughton a point opposite the common boundary of 190/192 Roding Road, south- westwards for a distance of approximately 5.2 metres. Greenhill, SOUTH EAST SIDE - From a point approximately 2.1 metres southeast of Buckhurst Hill a point opposite the eastern most corner of 1 to 12, 14 to 17 Greenhill, south-eastwards for a distance of approximately 4.6 metres. Warren Court, NORTH SIDE - from a point approximately 5.3 metres northwest of a point Chigwell opposite the common boundary of 25 / 26 and 27 / 28 Warren Court, north-westwards for a distance of approximately 5.2 metres. Dunmow Close, NORTH EAST SIDE - From a point approximately 0.9 metres southeast of Loughton a point opposite the common boundary between 5/6 and 7/8 Dunmow Close, south-eastwards for a distance of approximately 5.1 metres. Paradise Road, EAST SIDE - From a point approximately 1.3 metres south of a point Waltham Abbey opposite the common boundary of 8/9 Paradise Road, southwards for a distance of approximately 2.9 metres. -

ESSEX and SOUTHEND-On-SEA JOINT CONSTABULARY
If you have issues viewing or accessing this file contact us at NCJRS.gov. ESSEX and SOUTHEND-on-SEA JOINT CONSTABULARY . -" ' ~ ":~~~::~, '; .~~ CHIEF CONSTABLEIS ANNUAL ~ REPORT 0 1973 0-- ~ ~ =t- ' . c;::s ~" _________________.::l' ,) To: The Essex & Southend·on-Sea Joint Police Authority Ladies and Gentlemen I present my report on the Force and its work during the calendar year 1973. This is my last report as Chief Constable of the Joint Authority as the Force after an existence of only five years will assume a new identity as the Essex Police on 1 April 1974. I would like to thank all members and officers of the Authority who have taken such an interest in its work and con!ributed to its undoubted success. The new Force will be able to bU.ild on a sure foundation. / I am, Ladies and Gentlemen, Your Obedient Servant, J. C. NIGHTINGALE Chief Constable 3 INTRODUCTION The Force continued to prosper in 1973. The strength of police officers increased by 72 - a smallcr figure than in 1972 but the growth over the past two years enabled the length of the notional working week to be reduced from 44 hours to 42. This change, together with an increase in pension contributions during the year to pay for improvements in benefits, resulted in a reduction in net take home pay for most members of the Force in a period of rising prices. Nevertheless morale remains high and wastage has been reduced. The workload, as will be seen from the report, increases constantly and a steady growth of manpower at rather more than the present rate is needed to cope with it. -

Luton Borough Council Has an 'Audit Family' of Areas with Similar
Luton and its Audit Family Comparisons using data from the 2001 Census ________________________________________________________________________________________________________ Research and Intelligence Team Department of Environment & Regeneration March 2003 Please note that Luton Borough Council is licensed by the Office for National Statistics to make available 2001 Census data to third parties. However this licence does not permit third parties to reproduce 2001 Census data without themselves obtaining a licence from the Office for National Statistics Luton Borough Council has an ‘Audit Family’ of areas with similar characteristics. Included in this Audit Family are: • Blackburn with Darwen • Leicester City • Rochdale • Bolton • Medway • Slough • Bradford • Milton Keynes • Telford and Wrekin • Coventry • Oldham • Thurrock • Derby City • Peterborough • Walsall Source: Audit Commission This paper makes comparisons across the Audit Family using the Key Statistics for Local Authorities from the 2001 Census. If you require further information on this report, please contact either Tanya Ridgeon ([email protected]) or Sharon Smith ([email protected]) ________________________________________________________________________________________________________ Research and Intelligence Team Department of Environment & Regeneration March 2003 Please note that Luton Borough Council is licensed by the Office for National Statistics to make available 2001 Census data to third parties. However this licence does not permit third parties to reproduce