Summary Report Icd-9-Cm Coordination And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Presence of ROS in Inflammatory Environment of Peri-Implantitis Tissue
Journal of Clinical Medicine Article Presence of ROS in Inflammatory Environment of Peri-Implantitis Tissue: In Vitro and In Vivo Human Evidence 1, 2, 2, 3 4 Eitan Mijiritsky y, Letizia Ferroni y, Chiara Gardin y, Oren Peleg , Alper Gultekin , Alper Saglanmak 4, Lucia Gemma Delogu 5, Dinko Mitrecic 6, Adriano Piattelli 7, 8, 2,9, , Marco Tatullo z and Barbara Zavan * z 1 Head and Neck Maxillofacial Surgery, Department of Otoryngology, Tel-Aviv Sourasky Medical Center, Sackler Faculty of Medicine, Tel-Aviv University, Weizmann street 6, 6423906 Tel-Aviv, Israel; [email protected] 2 Maria Cecilia Hospital, GVM Care & Research, Cotignola, 48033 Ravenna, Italy; [email protected] (L.F.); [email protected] (C.G.) 3 Department of Otolaryngology Head and Neck Surgery and Maxillofacial Surgery, Tel-Aviv Sourasky Medical Center, Sackler School of Medicine, Tel Aviv University, 701990 Tel-Aviv, Israel; [email protected] 4 Istanbul University, Faculty of Dentistry, Department of Oral Implantology, 34093 Istanbul, Turkey; [email protected] (A.G.); [email protected] (A.S.) 5 University of Padova, DpT Biomedical Sciences, 35133 Padova, Italy; [email protected] 6 School of Medicine, Croatian Institute for Brain Research, University of Zagreb, Šalata 12, 10 000 Zagreb, Croatia; [email protected] 7 Department of Medical, Oral, and Biotechnological Sciences, University of Chieti-Pescara, via dei Vestini 31, 66100 Chieti, Italy; [email protected] 8 Marrelli Health-Tecnologica Research Institute, Biomedical Section, Street E. Fermi, 88900 Crotone, Italy; [email protected] 9 Department of Medical Sciences, University of Ferrara, via Fossato di Mortara 70, 44123 Ferara, Italy * Correspondence: [email protected] Co-first author. -
Overview of Biomaterials and Their Use in Medical Devices
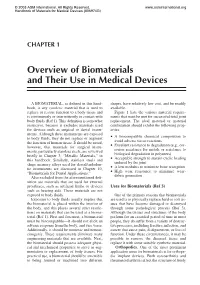
© 2003 ASM International. All Rights Reserved. www.asminternational.org Handbook of Materials for Medical Devices (#06974G) CHAPTER 1 Overview of Biomaterials and Their Use in Medical Devices A BIOMATERIAL, as defined in this hand- shapes, have relatively low cost, and be readily book, is any synthetic material that is used to available. replace or restore function to a body tissue and Figure 1 lists the various material require- is continuously or intermittently in contact with ments that must be met for successful total joint body fluids (Ref 1). This definition is somewhat replacement. The ideal material or material restrictive, because it excludes materials used combination should exhibit the following prop- for devices such as surgical or dental instru- erties: ments. Although these instruments are exposed A biocompatible chemical composition to to body fluids, they do not replace or augment • avoid adverse tissue reactions the function of human tissue. It should be noted, Excellent resistance to degradation (e.g., cor- however, that materials for surgical instru- • rosion resistance for metals or resistance to ments, particularly stainless steels, are reviewed biological degradation in polymers) briefly in Chapter 3, “Metallic Materials,” in Acceptable strength to sustain cyclic loading this handbook. Similarly, stainless steels and • endured by the joint shape memory alloys used for dental/endodon- A low modulus to minimize bone resorption tic instruments are discussed in Chapter 10, • High wear resistance to minimize wear- “Biomaterials for Dental Applications.” • debris generation Also excluded from the aforementioned defi- nition are materials that are used for external prostheses, such as artificial limbs or devices Uses for Biomaterials (Ref 3) such as hearing aids. -

CASODEX (Bicalutamide)
HIGHLIGHTS OF PRESCRIBING INFORMATION • Gynecomastia and breast pain have been reported during treatment with These highlights do not include all the information needed to use CASODEX 150 mg when used as a single agent. (5.3) CASODEX® safely and effectively. See full prescribing information for • CASODEX is used in combination with an LHRH agonist. LHRH CASODEX. agonists have been shown to cause a reduction in glucose tolerance in CASODEX® (bicalutamide) tablet, for oral use males. Consideration should be given to monitoring blood glucose in Initial U.S. Approval: 1995 patients receiving CASODEX in combination with LHRH agonists. (5.4) -------------------------- RECENT MAJOR CHANGES -------------------------- • Monitoring Prostate Specific Antigen (PSA) is recommended. Evaluate Warnings and Precautions (5.2) 10/2017 for clinical progression if PSA increases. (5.5) --------------------------- INDICATIONS AND USAGE -------------------------- ------------------------------ ADVERSE REACTIONS ----------------------------- • CASODEX 50 mg is an androgen receptor inhibitor indicated for use in Adverse reactions that occurred in more than 10% of patients receiving combination therapy with a luteinizing hormone-releasing hormone CASODEX plus an LHRH-A were: hot flashes, pain (including general, back, (LHRH) analog for the treatment of Stage D2 metastatic carcinoma of pelvic and abdominal), asthenia, constipation, infection, nausea, peripheral the prostate. (1) edema, dyspnea, diarrhea, hematuria, nocturia, and anemia. (6.1) • CASODEX 150 mg daily is not approved for use alone or with other treatments. (1) To report SUSPECTED ADVERSE REACTIONS, contact AstraZeneca Pharmaceuticals LP at 1-800-236-9933 or FDA at 1-800-FDA-1088 or ---------------------- DOSAGE AND ADMINISTRATION ---------------------- www.fda.gov/medwatch The recommended dose for CASODEX therapy in combination with an LHRH analog is one 50 mg tablet once daily (morning or evening). -

A Mini-Review of Dental Implant Biomaterials
Mini Review Modifying an Implant: A Mini-review of Dental Implant Biomaterials Oliver K. Semisch-Dieter1, Andy H. Choi1, Besim Ben-Nissan1 and Martin P. Stewart1,* Abstract 1School of Life Sciences, Faculty of Science, University Dental implants have been used as far back as 2000BC, and since then have developed into highly sophisti- of Technology Sydney, Ultimo, cated solutions for tooth replacement. It is becoming increasingly important for the materials used in dental implants to exhibit and maintain favorable long-term mechanical, biological and more recently, aesthetic NSW, Australia properties. This review aims to assess the biomaterials used in modern dental implants, introducing their properties, and concentrating on modifications to improve these biomaterials. Focus is drawn to the promi- nent biomaterials, titanium (Ti) and zirconia due to their prevalence in implant dentistry. Additionally, novel coatings and materials with potential use as viable improvements or alternatives are reviewed. An effective *Correspondence to: dental biomaterial should osseointegrate, maintain structural integrity, resist corrosion and infection, and not Martin P. Stewart cause systemic toxicity or cytotoxicity. Current materials such as bioactive glass offer protection against bio- E-mail: martin.stewart@uts. film formation, and when combined with a titanium–zirconium (TiZr) alloy, provide a reliable combination edu.au of properties to represent a competitive alternative. Further long-term clinical studies are needed to inform the development of next-generation materials. Received: September 7 2020 Revised: December 7 2020 Keywords Accepted: January 4 2021 Biocompatibility, biomaterials, dental implant, titanium, zirconia. Published Online: March 19 2021 Significance Statement Available at: Biomaterials have become essential for modern implants. -

Scientific Summary, Digital Implant Solutions
Atlantis® Simplant® Scientific Summary Digital Implant Solutions Comprehensive solutions for all phases of implant dentistry Welcome Are you looking for information about the excellent results with our individually designed Atlantis abutments and suprastructures and how to achieve simplicity, freedom, esthetics, and reliability when treating your patients? Or do you want to explore the research findings behind Simplant, a comprehensive digitial 3D system developed to accomplish more accurate and predictable implant treatment? You will find the answers here, and much more. This Scientific Summary provides a synopsis of the key research findings supporting our digital solutions including Atlantis patient-specific prosthetic solutions and computer guided implant treatment with Simplant. Each summary is based on facts retrieved from the original research article. The Scientific Summary focuses on the following topics: Atlantis® 9 Simplant® 23 References 30 Summary by Dentsply Sirona Implants of facts retrieved from the original articles. For a more comprehensive view of the documentation and research on our products, please refer to our Scientific Reviews. The Scientific Reviews are available for download at www.dentsplyimplants.com/science To improve readability for our customers, Dentsply Sirona does not use ® or ™ in body copy. However, Dentsply Sirona Implants does not waive any right to the trademark and nothing herein shall be interpreted to the contrary. Ongoing innovation For two decades, the Atlantis products and services have been -

The Costs and Benefits of Moving to the ICD-10 Code Sets
CHILDREN AND ADOLESCENTS This PDF document was made available from www.rand.org as a public CIVIL JUSTICE service of the RAND Corporation. EDUCATION ENERGY AND ENVIRONMENT Jump down to document HEALTH AND HEALTH CARE 6 INTERNATIONAL AFFAIRS POPULATION AND AGING The RAND Corporation is a nonprofit research PUBLIC SAFETY SCIENCE AND TECHNOLOGY organization providing objective analysis and effective SUBSTANCE ABUSE solutions that address the challenges facing the public TERRORISM AND HOMELAND SECURITY and private sectors around the world. TRANSPORTATION AND INFRASTRUCTURE U.S. NATIONAL SECURITY Support RAND Purchase this document Browse Books & Publications Make a charitable contribution For More Information Visit RAND at www.rand.org Explore RAND Science and Technology View document details Limited Electronic Distribution Rights This document and trademark(s) contained herein are protected by law as indicated in a notice appearing later in this work. This electronic representation of RAND intellectual property is provided for non-commercial use only. Permission is required from RAND to reproduce, or reuse in another form, any of our research documents for commercial use. This product is part of the RAND Corporation technical report series. Reports may include research findings on a specific topic that is limited in scope; present discus- sions of the methodology employed in research; provide literature reviews, survey instruments, modeling exercises, guidelines for practitioners and research profes- sionals, and supporting documentation; -

Frequently Asked Questions
LEARNING ABOUT THE CARDIOMEMS™ HF SYSTEM FREQUENTLY ASKED QUESTIONS WHAT IS THE CARDIOMEMS HF SYSTEM? CAN A MAGNETIC RESONANCE IMAGING (MRI) The CardioMEMS™ HF System is the first and SCAN BE DONE WITH THE PA SENSOR? only FDA-approved heart failure monitor proven to Patients can have an MRI scan under certain significantly reduce heart failure hospital admissions conditions. Talk with the doctor ordering the MRI and improve quality of life.1 scan to ensure that he or she knows that you have a CardioMEMS PA Sensor. HOW DOES THE CARDIOMEMS HF SYSTEM HELP A HEART FAILURE PATIENT? WILL THE PA SENSOR INTERFERE WITH AN MRI, Changes in PA pressures are an early indicator of A PACEMAKER OR AN IMPLANTABLE worsening heart failure. This can occur even before CARDIOVERTER DEFIBRILLATOR (ICD)? the patient notices symptoms such as shortness of No, the PA sensor will not interfere with a pacemaker breath or weight gain. or an ICD, even when a reading is being taken. Patients can have an MRI scan under certain conditions. Talk The CardioMEMS HF System comes with an with the doctor ordering the MRI scan to ensure that electronics unit used at home to take daily he or she knows that you have a PA sensor. measurements of PA pressures. These PA pressure readings are sent wirelessly to a secure website CAN PATIENTS TRAVEL WITH THE CARDIOMEMS for the clinician to review. This allows the care team HF SYSTEM? to confidently adjust medications without a patient Yes, patients can travel with the CardioMEMS HF feeling symptoms or needing a hospital or clinic visit. -

Science First Volume 5, Issue 1 2018
Science First Volume 5, Issue 1 2018 NobelActive® Over 10 years of clinical experience Cover NobelActive is an implant like no other. The back-tapered coronal design of NobelActive is designed to optimize bone and soft tissue volume for natural-looking esthetics. This is highlighted in the image in the foreground and the left inset. The right inset image focuses on a mesenchymal stem cell adhered to the proven TiUnite® implant surface. The background image shows the 3D mesh of the upper surface fading into a 2D outline illustration, combined with a NobelActive rendering focusing on the upper part of the implant. Contents NobelActive Over ten years of clinical experience with NobelActive® 4 Scientific evidence backs NobelActive® implants 5 Key studies 6 Clinical cases 9 Overview of studies 12 References 15 NobelActive Over ten years of clinical experience with NobelActive® The innovation of NobelActive represented a breakthrough in implant design, harmonizing biomedical engineering expertise with the clinical needs and the wisdom of clinicians. NobelActive’s expanding tapered implant body condenses bone gradually while the apex with drilling blades enables a smaller osteotomy. These features help to achieve good primary stability in demanding situations, such as soft bone or extraction sockets. Perfect harmony of drilling protocol, geometric design Good primary stability in demanding situations, and implant surface such as soft bone or extraction sockets The NobelActive surgical protocol and implant design are designed to provide good primary stability and support immediate loading. Reverse-cutting flutes with drilling blades on the apex enable experienced clinicians to adjust the implant position during placement for an optimized restorative orientation, particularly in extraction sites. -

Which Antibiotic Regimen Prevents Implant Failure Or Infection After Dental Implant Surgery? a Systematic Review and Meta-Analysis
Journal of Cranio-Maxillo-Facial Surgery 46 (2018) 722e736 Contents lists available at ScienceDirect Journal of Cranio-Maxillo-Facial Surgery journal homepage: www.jcmfs.com Review Which antibiotic regimen prevents implant failure or infection after dental implant surgery? A systematic review and meta-analysis * Fabio Rodríguez Sanchez a, , Carlos Rodríguez Andres b, Iciar Arteagoitia c, d a Epidemiology and Public Health Department, School of Medicine and Nursing, University of the Basque Country (UPV/EHU), Barrio Sarriena, s/n, 48940, Bilbao, Spain b School of Medicine and Nursing, University of the Basque Country (UPV/EHU) (Professor and Head of Epidemiology and Public Health Department), Barrio Sarriena, s/n, 48940, Bilbao, Spain c Department of Stomatology, School of Medicine and Nursing, University of the Basque Country (UPV/EHU), Barrio Sarriena, s/n, 48940, Bilbao, Spain d BioCruces Health Research Institute Member, Cruces University Hospital, Plaza de Cruces, 48903, Barakaldo, Spain article info abstract Article history: Objective: To assess which antibiotic regimen prevents dental implant failures or postoperative in- Paper received 8 January 2018 fections following dental implant placement. Accepted 8 February 2018 Materials and methods: Systematic review and meta-analysis. Data sources: Pubmed, Cochrane, Science Available online 26 February 2018 Direct, and EMBASE via OVID were searched up to August 2017. Only randomized controlled clinical trials (RCT) using antibiotics were included. Outcome measures were set on dental implant failures or post- Keywords: operative infection incidence after dental implant surgery. Three reviewers independently undertook Dental-implant surgery risk of bias assessment and data extraction. Stratified meta-analyses of binary data using fixed-effects Antibiotics fi Amoxicillin models were performed using Stata 14.0. -

Contraindications to Magnetic Resonance Imaging
Downloaded from heart.bmj.com on 8 November 2009 Contraindications to magnetic resonance imaging T Dill Heart 2008;94;943-948 doi:10.1136/hrt.2007.125039 Updated information and services can be found at: http://heart.bmj.com/cgi/content/full/94/7/943 These include: Data supplement "web only appendix" http://heart.bmj.com/cgi/content/full/94/7/943/DC1 References This article cites 23 articles, 9 of which can be accessed free at: http://heart.bmj.com/cgi/content/full/94/7/943#BIBL 1 online articles that cite this article can be accessed at: http://heart.bmj.com/cgi/content/full/94/7/943#otherarticles Rapid responses You can respond to this article at: http://heart.bmj.com/cgi/eletter-submit/94/7/943 Email alerting Receive free email alerts when new articles cite this article - sign up in the box at service the top right corner of the article Topic collections Articles on similar topics can be found in the following collections Clinical diagnostic tests (18476 articles) Drugs: cardiovascular system (22273 articles) Epidemiology (4597 articles) Notes To order reprints of this article go to: http://journals.bmj.com/cgi/reprintform To subscribe to Heart go to: http://journals.bmj.com/subscriptions/ Downloaded from heart.bmj.com on 8 November 2009 Education in Heart NON-INVASIVE IMAGING Contraindications to magnetic resonance imaging T Dill c Additional references are Magnetic resonance imaging (MRI) is a method turned on and off the rapid changing magnetic published online only at http:// that has evolved continuously during the past fields can induce electrical currents in electri- heart.bmj.com/content/vol94/ cally conductive devices and may directly cause issue7 20 years, yielding MR systems with stronger static magnetic fields, faster and stronger gradient neuromuscular stimulation. -

Architecture and Low Power Management of a Deep-Tissue Medical Implant System Powered by Human Body Energy Harvesting
Architecture and Low Power Management of a Deep-tissue Medical Implant System Powered by Human Body Energy Harvesting Elisabeth Benke1a, Adrian Fehrle1b, Johannes Ollech2c, Simon Schrampfer2d and Jörg Franke1e 1Institute for Factory Automation and Production Systems, Friedrich-Alexander-Universität Erlangen-Nürnberg, Germany 2Sentinum UG, Nürnberg, Germany {elisabeth.benke, adrian.fehrle, joerg.franke}@faps.fau.de, {j.ollech, s.schrampfer}@sentinum.de Keywords: Implantable Medical Devices, Energy Harvesting, Power Management, Hybrid Energy Storage Systems. Abstract: Active mechatronic implants applied to provide therapy of insufficient bodily functions and acquisition of biomedical data are an emerging field in the context of Medicine 4.0. Wireless data transmission between the implant and out-body devices enables patients and health care professionals to access physiological data as well as take technical control and also allows for home monitoring solutions. Due to the limitations associated with primary batteries or conventional wireless power transferring methods in deep-tissue layers, human body energy harvesting is a promising alternative or complement for power supply. A high efficient power management in order to reduce the implanted device’s energy consumption is not only requested to effectively use the limited amounts of energy harvested but also contributes to extend implantation times and thus avoid invasive surgical procedures. This paper presents solution approaches for both software- and hardware-based low power management and storage options for active deep-tissue implants using hybrid energy storage systems and considering miniaturisation requirements of devices powered by energy harvesting. 1 INTRODUCTION limitations, especially regarding size, bio- compatibility and the implantation depth power can While battery-powered medical implant devices such be transferred into. -

Artificial Organs: an Overview Evanjali Pradhan* Department of Biomedical Engineering, Utkal University, University in Bhubaneswar, Odisha, India
Engineer OPEN ACCESS Freely available online al ing ic & d e M m e d o i i c B a f l o D l e a v Journal of Biomedical Engineering and n i r c u e s o J ISSN: 2475-7586 Medical Devices Editorial Artificial Organs: An Overview Evanjali Pradhan* Department of Biomedical Engineering, Utkal University, University in Bhubaneswar, Odisha, India EDITORIAL have probably been around since ancient times, with the simple peg leg being the most well-known. An artificial organ is human made organ device or tissue that is implanted into a human collaborating with living tissue, to The development of artificial limbs has accelerated since then. replicate or augment a particular function or functions in order New plastics and other materials, such as carbon fibre, have made it for the patient to return to a normal life as soon as possible. For possible to make artificial limbs stronger and lighter, reducing the example- Artificial organs may also be used to replace bones and amount of extra energy required to operate the limbs. Additional joints, such as those used in hip replacements. materials have made it possible to look much more natural for artificial limbs. [nine] Prostheses can be classified approximately Purpose as upper- and lower-extremity and can take many shapes and sizes. New developments in artificial limbs provide additional stages of Artificial organ design and installation, which is initially a very human body incorporation. time-consuming and costly operation, may require several years Bladder: Neural prostheses are a set of devices that can replace of ongoing maintenance services that a natural organ does not a motor, sensory or cognitive mode that may have been affected require.