Purbi Champaran (Motihari)
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

DISTRICT : Champaran-W
District District District District District Sl. No. Name of Husband's/Father,s AddressDate of Catego Full Marks Percent Choice-1 Choice-2 Choice-3 Choice-4 Choice-5 Candidate Name Birth ry Marks Obtained age (With Rank) (With Rank) (With Rank) (With Rank) (With Rank) DISTRICT : Champaran-W 1 PUSHPASRI NARENDRA w/o- narendra kumar 06-Feb-72 BC 900 675 75 Nawada (21) Saharsa (6) Champaran-W Patna (35) Purnia (6) KUMAR vill- jagatpur (1) post- harnaut dist- nalanda pin code- 803110 2 RENU KUMARISRI SURENDRA c/o sri surendra prasad 05-Feb-69 BC 900 672 74.67 Nalanda (32) Kaimur (3) Jahanabad (25) Gaya (24) Champaran-W (2) PRASAD SINGH singh, village+post khaddi lodipur, via- akanger sarai, district- nalanda, bihar pin 801301 3 KUMARI APARNA ASHOK KUMAR vill- bhojit pur, post- 16-Apr-83 BC 700 511 73 Champaran-E (7) Champaran-W Madhubani (2) Darbhanga (13) Muzaffarpur (23) PRIYA ekangar sarai, dist- (3) nalanda. 4RINA KUMARISRI KUMAR MAHTO d/o sri kumar mahto, 08-Dec-83 SC 500 365 73 Champaran-E (6) Champaran-W Sitamarahi (8) Madhubani (4) Patna (69) village- sakhuanwan, (4) post- gounoli, p.s. walmiki nagar, district- pachim champaran, bihar pin 845107 5RINA KUMARIMANOJ KUMAR vill- muzaffarpur, post- 28-Oct-88 BC 700 508 72.57 Champaran-E (8) Champaran-W Madhubani (5) Darbhanga (16) Samastipur (29) kathoule, disst- nalanda. (5) 6 SUCHITRA VIKASH PRASAD w/o- vikash prasad, 08-Feb-83 BC 700 507 72.43 Champaran-W Champaran-E (9) Madhubani (8) Darbhanga (18) Samastipur (32) KUMARI vill+post- ajnaura, (6) nalanda 7KUMARI SRI AMRESH musahari nagin -
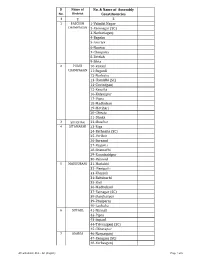
AC with District Dist
Sl Name of No. & Name of Assembly No. District Constituencies 1 2 3 1 PASCHIM 1-Valmiki Nagar CHAMPARAN 2-Ramnagar (SC) 3-Narkatiaganj 4-Bagaha 5-Lauriya 6-Nautan 7-Chanpatia 8-Bettiah 9-Sikta 2 PURVI 10-Raxaul CHAMPARAN 11-Sugauli 12-Narkatia 13-Harsidhi (SC) 14-Govindganj 15-Kesaria 16-Kalyanpur 17-Pipra 18-Madhuban 19-Motihari 20-Chiraia 21-Dhaka 3 SHEOHAR 22-Sheohar 4 SITAMARHI 23-Riga 24-Bathnaha (SC) 25-Parihar 26-Sursand 27-Bajpatti 28-Sitamarhi 29-Runnisaidpur 30-Belsand 5 MADHUBANI 31-Harlakhi 32- Benipatti 33-Khajauli 34-Babubarhi 35-Bisfi 36-Madhubani 37-Rajnagar (SC) 38-Jhanjharpur 39-Phulparas 40-Laukaha 6 SUPAUL 41-Nirmali 42-Pipra 43-Supaul 44-Triveniganj (SC) 45-Chhatapur 7 ARARIA 46-Narpatganj 47-Raniganj (SC) 48-Forbesganj AC with district Dist. - AC (English) Page 1 of 6 Sl Name of No. & Name of Assembly No. District Constituencies 1 2 3 49-Araria 50-Jokihat 51-Sikti 8 KISHANGANJ 52-Bahadurganj 53-Thakurganj 54-Kishanganj 55-Kochadhaman 9 PURNIA 56-Amour 57-Baisi 58-Kasba 59-Banmankhi (SC) 60-Rupauli 61-Dhamdaha 62-Purnia 10 KATIHAR 63-Katihar 64-Kadwa 65-Balrampur 66-Pranpur 67-Manihari (ST) 68-Barari 69-Korha (SC) 11 MADHEPURA 70-Alamnagar 71-Bihariganj 72-Singheshwar (SC) 73-Madhepura 12 SAHARSA 74-Sonbarsha (SC) 75-Saharsa 76-Simri Bakhtiarpur 77-Mahishi 13 DARBHANGA 78-Kusheshwar Asthan (SC) 79-Gaura Bauram 80-Benipur 81-Alinagar 82-Darbhanga Rural 83-Darbhanga 84-Hayaghat 85-Bahadurpur 86-Keoti 87-Jale 14 MUZAFFARPUR 88-Gaighat 89-Aurai 90-Minapur 91-Bochaha (SC) 92-Sakra (SC) 93-Kurhani 94-Muzaffarpur 95-Kanti 96-Baruraj AC with district Dist. -
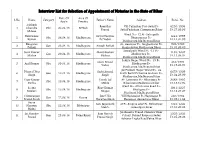
Interview List for Selection of Appointment of Notaries in the State of Bihar
Interview List for Selection of Appointment of Notaries in the State of Bihar Date Of Area Of S.No. Name Category Father's Name Address Enrol. No. App'n Practice Subhash Ramvilas Vill-Pakarihar Post-Sathi Ps- 8230/1996 1 Chandra Obc 06.04.18 Bettiah Prasad Sathi,Pashchim Champaran,Bihar Dt.27.09.96 Mohan Ward No- 12 At- Sahugadh Balkrishna Satya Narayan 1664/1999 2 Obc 06.04.18 Madhepura Bhagwanpur Ps- Kumar Pd Yadav Dt.14.04.99 Madhepura,Madhepura,Bihar Bhagwan At- Gauripur Po- Singheshwar Ps- 902/1989 3 Gen 08.04.18 Madhepura Awadh Pathak Pathak Singheshwar,Madhepura,Bihar Dt.01.09.89 Jaypalpatti Ward No -15 Po- Sunil Kumar Manibhushan 1182/2007 4 Gen 09.04.18 Madhepura Madhepura Ps - Mishra Mishra Dt.11.04.07 Madhepura,Madhepura,Bihar Lohiya Nagar Ward No- 19 Po- Guru Prasad 410/1991 5 Anil Kumar Obc 09.04.18 Madhepura Madhepura Ps- Yadav Dt.19.02.91 Madhepura,Madhepura,Bihar Jai Prakash Nagar Ward No- 06 Dharni Dhar Sachidanand 6679/1999 6 Gen 10.04.18 Madhepura South East Of Chamra Godoun Po- Singh Singh Dt.24.08.99 Madhepura,Madhepura,Bihar Vijay Kumar Tanuk Lal At- Laxmipur Po- Bihariganj Ps- 3883/1995 7 Obc 10.04.18 Madhepura Mehta Mehta Bihariganj,Madhepura,Bihar Dt.18.10.95 Ward No- 09 Cinema Road Po- Seema Bijay Kumar 1931/2007 8 Obc 15.04.18 Madhepura Murliganj Ps- Kumari Bhagat Dt.18.07.07 Murliganj,Madhepura,Bihar Chittaranjan Late Udit Vill Nayanagar Po Nayanagar Ps 620/1984 9 Gen 22.06.18 Rosera Prasad Singh Narayan Singh Hasanpur ,Samastipur,Bihar Dt.23.11.84 Surya Late Jagannath At Po-Singhia Ghat Ps- Bibhutipur 1232/2003 -

Glimpses of Sugarcane Varietal Screening and Improvement at Pusa, Bihar
ACTA SCIENTIFIC AGRICULTURE (ISSN: 2581-365X) Volume 4 Issue 3 March 2020 Review Article Glimpses of Sugarcane Varietal Screening and Improvement at Pusa, Bihar Balwant Kumar* Received: January 18, 2020 SRI, DRPCAU, Pusa, Bihar, India Published: February 08, 2020 Balwant Kumar, SRI, DRPCAU, Pusa, Bihar, India. *Corresponding Author: © All rights are reserved by Balwant DOI: 10.31080/ASAG.2020.04.0793 Kumar. Abstract Sugarcane is primarily grown in nine states of India namely; Uttar Pradesh, Maharashtra, Andhra Pradesh, Bihar, Gujarat, Haryana, Karnataka, Punjab, and Tamil Nadu. During early 19th century sugarcane cultivation started as cash crop and number of sugar facto- ries open keeping in view a glimpses of sugarcane varietal screening and Improvement has been reviewed and found that Bihar was rich in term of sugar factories and its 20-40% share in national sugar production was already reported. It was the introduction of Co seedling that replace local varieties under cultivation those were Co 210, Co213, Co 214, Co 313, Co 331, Co 513,Co 356, Co 395,Co 453,Co508 and CoK 32, Co 383, Co 622,Co 419,Co 617,Co1148 and Co 1158 while in present varietal scenario cultivated varieties are Co 0238, Co 0118, Co 98014, CoP 9301, CoLk 94184, CoP 112, CoSe 01434, CoP 09437, BO 154 and CoP 16437. It was also found that POJ 2878, Co285, Co281, CP 28/11, Co213 & Co205 were mainly responsible for improvement in high yield and high sugar. The varietal development and evaluation of sugarcane varieties started in Bihar by after that Central Sugarcane Research Institute was established 1932 since then total 281 clones were developed at SRI, while several Sugarcane varieties of other place were also evalu- ated. -
West Champaran Introduction
DISTRICT PROFILE WEST CHAMPARAN INTRODUCTION West Champaran is an administrative district in the state of Bihar. West Champaran district was carved out of old champaran district in the year 1972. It is part of Tirhut division. West Champaran is surrounded by hilly region of Nepal in the North, Gopalganj & part of East Champaran district in the south, in the east it is surrounded by East Champaran and in the west Padrauna & Deoria districts of Uttar Pradesh. The mother-tongue of this region is Bhojpuri. The district has its border with Nepal, it has an international importance. The international border is open at five blocks of the district, namely, Bagha- II, Ramnagar, Gaunaha, Mainatand & Sikta, extending from north- west corner to south–east covering a distance of 35 kms . HISTORICAL BACKGROUND The history of the district during the late medieval period and the British period is linked with the history of Bettiah Raj. The British Raj palace occupies a large area in the centre of the town. In 1910 at the request of Maharani, the palace was built after the plan of Graham's palace in Calcutta. The Court Of Wards is at present holding the property of Bettiah Raj. The rise of nationalism in Bettiah in early 20th century is intimately connected with indigo plantation. Raj Kumar Shukla, an ordinary raiyat and indigo cultivator of Champaran met Gandhiji and explained the plight of the cultivators and the atrocities of the planters on the raiyats. Gandhijii came to Champaran in 1917 and listened to the problems of the cultivators and the started the movement known as Champaran Satyagraha movement to end the oppression of the British indigo planters. -

Kesariya Stupa: Recently Excavated Architectural Marvel
Proceeding of the International Conference on Archaeology, History and Heritage, Vol. 1, 2019, pp. 27-31 Copyright © 2019 TIIKM ISSN 2651-0243online DOI: https://doi.org/10.17501/26510243.2019.1103 KESARIYA STUPA: RECENTLY EXCAVATED ARCHITECTURAL MARVEL Ishani Sinha Deccan College Post Graduate and Research Institute, Pune, Maharashtra, India Abstract: The early Buddhist texts record that Buddha announced his approaching nirvana to the monks at vaishali. According to historical traditions, monks followed him as he departed from Vaishali after delivering the last sermon. Buddha persuaded them to return back and presented his alms-bowl to them as memorial. To commemorate that event a stupa was built there which is now identified with kesariya stupa (in Bihar) and which falls en route from Vaishali to Kushinagar (in eastern Uttar Pradesh) where Buddha attained nirvana. This stupa finds reference in the travelogues of Fa Xian and Xuan Zang, the two celebrated Chinese monks of fifth and seventh century CE respectively. Briefly mentioned by Alexander Cunningham in 1861-62, the stupa mound at Kesariya was subjected to meticulous excavation from 1997-98 onwards by Archaeological Survey of India which is still continuing. The unearthed brick stupa is datable to Gupta period (5th-6th century CE) although an earlier phase datable to Sunga-Satavahana period (1st-2nd century CE) was also traced below it. The stupa is a six terraced structure with a cylindrical drum atop and a group of cells, with intervening polygonal designs, on each terrace enshrining stucco image of Buddha. With an extant height of about 31.5 metres and a diameter of about 123 metres, it is undoubtedly one of the tallest and most voluminous stupas in India. -

Harsidhi Assembly Bihar Factbook
Editor & Director Dr. R.K. Thukral Research Editor Dr. Shafeeq Rahman Compiled, Researched and Published by Datanet India Pvt. Ltd. D-100, 1st Floor, Okhla Industrial Area, Phase-I, New Delhi- 110020. Ph.: 91-11- 43580781, 26810964-65-66 Email : [email protected] Website : www.electionsinindia.com Online Book Store : www.datanetindia-ebooks.com Report No. : AFB/BR-013-0619 ISBN : 978-93-5313-089-3 First Edition : January, 2018 Third Updated Edition : June, 2019 Price : Rs. 11500/- US$ 310 © Datanet India Pvt. Ltd. All rights reserved. No part of this book may be reproduced, stored in a retrieval system or transmitted in any form or by any means, mechanical photocopying, photographing, scanning, recording or otherwise without the prior written permission of the publisher. Please refer to Disclaimer at page no. 186 for the use of this publication. Printed in India No. Particulars Page No. Introduction 1 Assembly Constituency - (Vidhan Sabha) at a Glance | Features of Assembly 1-2 as per Delimitation Commission of India (2008) Location and Political Maps Location Map | Boundaries of Assembly Constituency - (Vidhan Sabha) in 2 3- District | Boundaries of Assembly Constituency under Parliamentary 10 Constituency - (Lok Sabha) | Village-wise Winner Parties- 2019, 2015, 2014, 2010 and 2009 Administrative Setup 3 District | Sub-district | Towns | Villages | Inhabited Villages | Uninhabited 11-17 Villages | Village Panchayat | Intermediate Panchayat Demographics 4 Population | Households | Rural/Urban Population | Towns and Villages -

District -EAST CHAMPARAN -~
[~ District -EAST CHAMPARAN No. of Post -27 (GEN-14, EBC-5, SC-4, BC-3, BC-Women-1) General Category s. Roll Name of the Father'sl Correspondence Date of Mobile No. No. Candidate Husband's Name Address Birth No. 1 81 Madhuri Kumari Wlo-Shri Rajesh Thakurwari, 2/10/1972 9470233044 Kumar In front of Rani Sati Mandir, Motihari, E- Champaran- 845401 2 55 Manoj Prasad Baidyanath Prasad VilI+PO- Mathiya Brat 12/11/1983 9430286503 Yadav Yadav PS- Chhauradano Dist. East Champaran Pin-845302 3 59 Alka Kumari Deepak Kumar Parsouni Devajeet 10/211975 9430876245 PO- Mehsi 9430876247 Thana- Mehsi Dist. East Champaran Pin-845426 4 26 Shyam Kishor Gauri Shankar C/o Sri Sheo Shankar Pandey 1/3/1977 9334314454. Mishra Mishra Officer's Colony Power House Chowk Opp- Little Heart Public School (Bara chakia) PO-Bara Chakia Dist. East Champaran Pin-845412 5 15 Madan Kumar Potan Mahto VilI- Hindu Chakiya 3/211986 9939240658 PO- Bara Chakiya Dist. East Champaran Pin-845412 6 89 Ram Naresh Banshi Prasad At-Shivnath Mehta Lodge, 2/3/1974 9661218972 Prasad Room No-4 (F) Gulbighat, Mahendru Patna-800006 7 88 Kundan Kumar Shambhu Prasad C/o-Dr Shambhu Prasad 9/3/1983 9931780815 Homeo chikitsalya Janpul Chauk, Bettiah, Road,Motihari- 845401 E. Motihari 8 5 Chandan Jayswal Sunil Kumar Behind Payal Cinema 20/02/1985 9934824243 Jayswal Chhatauni Chowk 9334970534 Motihari Dist. East Champaran Pin-845401 "- ~ \~c.-~ i 9 37 Akhileshwar Jagannath Prasad Vill+PO- Turkaulia Bazar 8/1/1977 9097616700 Kumar Gupta Gupta PS+Anchal-Turkoliya Bazar Dist. -

Break-Up of Contesting Candidates
1- Dhanaha 1. No. and Name of the Constituency : : 1 - Dhanaha 2. Form Unique Serial Number (FUSN) Prefix : : KMQ 3. Type of Constituency (Gen/SC/ST) : : GEN 4. Name and Designation of the Returning Officer : Sri M.Jaya Deputy Director, Consolidation, West Champaran 5. Date of Poll 13/11/05 6. Date of Repoll (if any) - 7. Date of Commencement of Counting 22-Nov-2005 8. Date of Declaration of Result 22-Nov-2005 9. Data About Polling Stations : Regular Polling Stations - 129 Average No. of Electors Per Polling Station - 876 Auxilliary Polling Stations 9 Average No. of Voters Per Polling Station - 429 Total Polling Stations 138 10. Data About Candidates : Men Women Total No. of Nomination Filed : 11 0 11 No. of Nomination Rejected : 0 0 0 No. of Nomination found correct after scrutiny : 11 0 11 No. of Withdrawals : 0 0 0 No. of Contesting Candidates : 11 0 11 No. of Candidates who forfeited their deposits : 8 0 8 Break-Up of Contesting Candidates National Parties : 1 0 1 State Parties : 4 0 4 Registered (Unrecognised) Parties : 2 0 2 Independents : 4 0 4 11. Details about Electors : General Service Total Male 68,015 5 68,020 Female 52,823 3 52,826 Total 120,838 8 120,846 12. Details about Voters : General Postal Total Male 33,424 0 33,424 Female 25,829 0 25,829 Total 59,253 0 59,253 Rejected Votes 0 Missing Votes 0 1- Dhanaha 13. Names of Contesting Candidates and their details : Sl. Candidate Name & Address SC/ Sex Party Symbol Final No. -

Soil Resource of East Champaran (Motihari) District, Bihar Abstract
Soil Resource of East Champaran (Motihari) District, Bihar Abstract 1. Surveyed Area : East Champaran district, Bihar 2. Location : Latitude 26°15´ 16 ´´to 27° 01´ 13´´ N Longitude 84°29´ 13´´ to 85° 17´ 55´´ E 3. Agroclimatic : Middle Gangetic Plain Region (Zone – IV as per planning commission) 4. Total Area of the : 396803 ha District 5. Kind of Survey : Soil Resource Mapping using Remote Sensing and GIS Techniques 6. Base Map : IRS-ID Geocoded Satellite Imagery (1:50,000 scale) Survey of India Topographical maps on 1:50,000 scale. 7. Scale of Mapping : 1:50,000 8. Period of Survey : January, 2015 9. Soil Series Association mapped and their respective area: Sl. No. Mapping Unit Soil Series Association Area(ha) Area% 01 ALb1a1 Kesaria, Rariaha 29773 7.50 02 ALb1a2 Bhawanipur, Partapur, Jhitkahia 70624 17.80 03 ALb1a3 Champapur, Jhajhara, Karmoulia 40742 10.27 04 ALb1a4 Bhakhari, Mathia Mohan 82363 20.75 05 ALb2a1 Mathbanbari, Jhakra 83043 20.93 06 ALb2a2 Sakrar, Parsaunikapur, Fatuha 29482 7.43 07 ALb2b1 Dhekha, Fatuha 2073 0.52 08 ALe2a1 Dumariya Ghat, Madhubani Ghat 10277 2.59 09 ALe2d1 Dumariya Ghat 7279 1.83 10 ALg3a1 Piprakothi, Jitwara 6968 1.76 11 ALn2a1 Tharghatma, Jitwara 9828 2.48 12 Miscellaneous Habitation 4035 1.02 River & Waterbody 20316 5.12 Grand Total 396803 100 i 10. Salient Features: Physiographic division of the soils of the East Champaran district of Bihar: Landscape Physiography Area (ha) Area(%) Alluvium Alluvial Plain 338100 85.20 Flood Plain 9828 2.48 Levee 17556 4.42 Stream/River Banks 6968 1.76 Miscellaneous Habitation 4035 1.02 River & Waterbody 20316 5.12 Total 396803 100 Soils of the district fall in two slope classes: Sl. -

Ministry of Road Transport & Highways Government of India Consultancy Services for Preparation of Feasibility Study and Deta
Ministry of Road Transport & Highways Government of India Consultancy Services for preparation of Feasibility Study and Detailed Project Report for Improvement to Two Lane with Paved shoulder of (i) Stretch from Gopalganj on NH-27-Areraj-Sugauli on NH-727 & (ii) Stretch from Areraj-Motihari in Bihar on EPC Mode REQUEST FOR PROPOSAL (RFP) (International Competitive Bidding) July, 2016 INDEX Sl. No. Contents Page No. 1 Notice for inviting the proposals for Consultancy services 1 2 Letter of Invitation 2-15 3. Annex - I : List of Project along with Package Nos. 16 4. Data Sheet 17-22 5. Appendix - I : Terms of Reference 23-66 6. Supplement -I: Additional Requirements for Hill Roads 67-69 7. Supplement - II: Additional Requirements for Bridges 70-74 8 Supplement – III: Additional requirement for safety audit 75-77 9. Enclosure - I : Manning Schedule 78 10 Enclosure - II : Qualification Requirements of Key Personnel 79-82 11. Enclosure - III : Schedule for Submission of Reports and Documents 83 12. Appendix - II : Formats for Proof of Eligibility 84-90 13. Appendix - III : Formats for Technical Proposals 91-103 14. Appendix - IV : Formats for Financial Proposals 104-110 15. Appendix - V : Draft Contract Agreement 111-148 1 Ministry of Road Transport & Highways Government of India MORT&H intends to take up the Consultancy Services for preparation of Feasibility Study and Detailed Project Report for Improvement to Two Lane with Paved shoulder of (i) Stretch from Gopalganj on NH- 27-Areraj-Sugauli on NH-727 & (ii) Stretch from Areraj-Motihari in Bihar on EPC / PPP Mode. The details of the roads are as follows: S. -

West Champaran District, Bihar State
भूजल सूचना पुस्तिका पस्चचमी च륍पारण स्जला, बिहार Ground Water Information Booklet West Champaran District, Bihar State ADMINISTRATIVE MAP WEST CHAMPARAN DISTRICT, BIHAR N 0 5 10 15 20 Km Scale Masan R GAONAHA SIDHAW RAMNAGAR PIPRASI MAINATAND BAGAHA NARKATIAGANJ LAURIYA MADHUBANI SIKTA BHITAHA CHANPATTIA GandakJOGAPATTI R MANJHAULIA District Boundary BETTIAH Block Boundary THAKRAHA BAIRIA Road Railway NAUTAN River Block Headquarter के न्द्रीय भमू मजल िो셍 ड Central Ground water Board Ministry of Water Resources जल संसाधन मंत्रालय (Govt. of India) (भारि सरकार) Mid-Eastern Region Patna मध्य-पर्वू ी क्षेत्र पटना मसिंिर 2013 September 2013 1 Prepared By - Dr. Rakesh Singh, Scientist – ‘B’ 2 WEST CHAMPARAN, BIHAR S. No CONTENTS PAGE NO. 1.0 Introduction 6 - 10 1.1 Administrative details 1.2 Basin/sub-basin, Drainage 1.3 Irrigation Practices 1.4 Studies/Activities by CGWB 2.0 Climate and Rainfall 11 3.0 Geomorphology and Soils 11 - 12 4.0 Ground Water Scenario 12 – 19 4.1 Hydrogeology 4.2 Ground Water Resources 4.3 Ground Water Quality 4.4 Status of Ground Water Development 5.0 Ground Water Management Strategy 19 – 20 5.1 Ground Water Development 5.2 Water Conservation and Artificial Recharge 6.0 Ground Water related issue and problems 20 7.0 Mass Awareness and Training Activity 20 8.0 Area Notified by CGWB/SGWA 20 9.0 Recommendations 20 FIGURES 1.0 Index map of West Champaran district 2.0 Month wise rainfall plot for the district 3.0 Hydrogeological map of West Champaran district 4.0 Aquifer disposition in West Champaran 5.0 Depth to Water Level map (May 2011) 6.0 Depth to Water Level map (November 2011) 7.0 Block wise Dynamic Ground Water (GW) Resource of West Champaran district TABLES 1.0 Boundary details of West Champaran district 2.0 List of Blocks in West Champaran district 3.0 Land use pattern in West Champaran district 4.0 HNS locations of West Champaran 5.0 Blockwise Dynamic Ground Water Resource of West Champaran District (2008-09) 6.0 Exploration data of West Champaran 7.0 Chemical parameters of ground water in West Champaran 3 WEST CHAMPARAN - AT A GLANCE 1.