Acute Watery Diarrhoea in Southern Sudan Date of Reporting
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
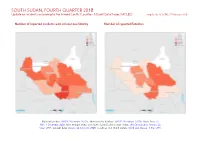
SOUTH SUDAN, FOURTH QUARTER 2018: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED) Compiled by ACCORD, 25 February 2020
SOUTH SUDAN, FOURTH QUARTER 2018: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 25 February 2020 Number of reported incidents with at least one fatality Number of reported fatalities National borders: GADM, November 2015a; administrative divisions: GADM, November 2015b; Abyei Area: SS- NBS, 1 December 2008; Ilemi triangle status and South Sudan/Sudan border status: UN Cartographic Section, Oc- tober 2011; incident data: ACLED, 22 February 2020; coastlines and inland waters: Smith and Wessel, 1 May 2015 SOUTH SUDAN, FOURTH QUARTER 2018: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 25 FEBRUARY 2020 Contents Conflict incidents by category Number of Number of reported fatalities 1 Number of Number of Category incidents with at incidents fatalities Number of reported incidents with at least one fatality 1 least one fatality Violence against civilians 120 48 142 Conflict incidents by category 2 Battles 84 49 156 Development of conflict incidents from December 2016 to December 2018 2 Strategic developments 18 0 0 Protests 6 0 0 Methodology 3 Explosions / Remote 2 1 2 Conflict incidents per province 4 violence Riots 2 0 0 Localization of conflict incidents 4 Total 232 98 300 Disclaimer 5 This table is based on data from ACLED (datasets used: ACLED, 22 February 2020). Development of conflict incidents from December 2016 to December 2018 This graph is based on data from ACLED (datasets used: ACLED, 22 February 2020). 2 SOUTH SUDAN, FOURTH QUARTER 2018: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 25 FEBRUARY 2020 Methodology sources if necessary. -

South Sudan (UNMISS) Media & Spokesperson Unit Communications & Public Information Office MEDIA MONITORING REPORT
United Nations Mission in South Sudan (UNMISS) Media & Spokesperson Unit Communications & Public Information Office MEDIA MONITORING REPORT FRIDAY, 08 NOVEMBER 2013 SOUTH SUDAN Kiir to appoint ex-rebels into government positions (Sudantribune.com) Media warned: register or face closure (Eye Radio) Security in Pibor: armed men cause panic (Sudantribune.com) South Sudan blames LRA for deadly attacks (VoA News) LRA attacks kill two in Western Equatoria State (Radio Miraya) One person killed as suspected LRA rebels attack Ezo County (Gurtong) Unity State court plans to ban women, irls from chewing bubble gum (Eye Radio) Haforere residents abandon homes over inter-clan conflict (Emmanuel Radio) Journalists‟ body gets new executive members (Gurtong) Catholic Radio Network reviews challenges (Catholic Radio Network) Rise in commodity prices caused by poor road network (Gurtong) South Africa to support South Sudan development (Sudantribune.com) Power cuts to continue for another 10 years (Bakhita Radio) Government needs electricity to address unemployment (Emmanuel Radio) OTHER HIGHLIGHTS Sudanese rebels tell world to „wake up‟ to war (Reuters) LINKS TO STORIES FROM THE MORNING MEDIA MONITOR Akobo County Commissioner denies youth mobilizing for raid (Sudantribune.com) Disarmament must be conducted in payams hiding weapons – official (Sudantribune.com) Wau police arrest most wanted criminal (Voice of Hope) Locals in Unity State blame oil companies for not doing enough to protect environment (Sudantribune.com) Rumbek FM presenters under threat file police case (Catholic Radio Network) Taha – Relations with South Sudasn progressing rapidly for the better (Sudan News Agency) NOTE: Reproduction here does not mean that the UNMISS Communications & Public Information Office can vouch for the accuracy or veracity of the contents, nor does this report reflect the views of the United Nations Mission in South Sudan. -

Action Research Report
FOOD SECURITY THROUGH AGRIBUSINESS IN SOUTH SUDAN (SSADP II) Action Research Report Johan te Velde, 6 February 2020 Table of contents FOOD SECURITY THROUGH AGRIBUSINESS IN SOUTH SUDAN (SSADP II) .............................................1 Table of contents ................................................................................................................................2 Acronyms............................................................................................................................................3 Preface ...............................................................................................................................................5 Executive summary .............................................................................................................................6 1. Introduction and background..................................................................................................... 10 1.1 The SSADP II (South Sudan Agribusiness Development Programme II) ................................. 10 1.2 Purpose and objectives of the Action Research ................................................................... 14 1.3 Action Research team ......................................................................................................... 15 2. Methodology ............................................................................................................................. 17 2.1 The AR methodology .......................................................................................................... -

Imatong Socio-Economic Baseline
SOCIO-ECONOMIC BASELINE SURVEY OF IMATONG MOUNTAINS WATER TOWER, AND KINYETI RIVER WATERSHED, SOUTH SUDAN, 2014 For AFRICAN WILDLIFE FOUNDATION Nairobi/Kenya BASELINE SURVEY REPORT 2014 ACKNOWLEDGEMENT We are most grateful to: South Sudan Chamber of Commerce and Agriculture (SSCCA); Government of Eastern Equatoria State (EES), State Ministries of Local Government, Law Enforcement and Wildlife Conservation; Finance and Economic Planning; Agriculture and Forestry; Health and Youth and Sports. We are most grateful to the Payam and Boma leaders especially those from the counties of Torit, Magwi and Ikotos. We are most grateful to the chiefs in the bomas the studies were conducted. Gratitude also goes to the household respondents who represented the counties and generously provided the information upon which this report is based. We would also like to acknowledge the substantive contribution of the research field team. Lastly, we are most honored to the African Wildlife Foundation (AWF) for giving us the opportunity to do this assignment. ii ABBREVIATIONS AND ACRONYMS AWF African Wildlife Foundation CBNRM Community Based Resource Management DDR Disarmament, Demobilization and Reintegration. EA Enumeration Area EES Eastern Equatoria State ECG Environment Cluster Group EIA Environment impact Assessment EKN Embassy of the Kingdom of the Netherlands in Juba FGD Focus Group Discussion GROSS Government of South Sudan ICFR Imatong Central Forest Reserve IEC Information Education and communication IDI In-depth Interview IKW Imatong Mountains Basin -
The Nasty War: Organised Violence During the Anya-Nya Insurgency in South Sudan, –*
Journal of African History, . (), pp. –. © Cambridge University Press doi:./S THE NASTY WAR: ORGANISED VIOLENCE DURING THE ANYA-NYA INSURGENCY IN SOUTH SUDAN, –* ØYSTEIN H. ROLANDSEN Peace Research Institute Oslo NICKI KINDERSLEY Cambridge University Abstract In 1963, unrest in Sudan’s three southern provinces (today’s South Sudan) escalated into a civil war between the government and the Anya-Nya rebellion. The subsequent eight years of violence has hitherto largely escaped scrutiny from academic researchers and has remained a subject of popular imagination and politicised narratives. This article demon- strates how this history can be explored with greater nuance, thereby establishing a local history of a postcolonial civil war. Focusing on the garrison town of Torit, our research reveals a localised and personalised rebellion, made up of a constellation of parochial armed groups. This new history also demonstrates how these parties built upon experiences from imperial conquest and colonial rule when entrenching violent wartime practices such as mass dis- placement and encampment, the raising of local militias and intelligence networks, and the deliberate starvation of civilians — all common methods in subsequent wars. Key Words South Sudan, governance, civil war, rebellion, counter-insurgency, organised violence. INTRODUCTION In September , government security forces in the South Sudanese town of Torit discov- ered that a man named Sakrana, who was suffering from leprosy (Hansen’s disease), was gathering intelligence for the Anya-Nya rebels, and that he was carrying with him a large quantity of salt and other supplies. He came from the leprosy colony of Ido, five * This has been a long-term project, and the authors have incurred debts from many generous individuals, none of whom bear any responsibility for any shortcomings of this article. -

Women's Experiences During Armed Conflict in Southern
WOMEN’S EXPERIENCES DURING ARMED CONFLICT IN SOUTHERN SUDAN, 1983-2005 THE CASE OF JUBA COUNTY CENTRAL EQUATORIAL STATE WOMEN’S EXPERIENCES DURING ARMED CONFLICT IN SOUTHERN SUDAN, 1983 - 2005: THE CASE OF JUBA COUNTY - CENTRAL EQUATORIAL STATE AN Isis-WICCE RESEARCH REPORT IN COLLABORATION WITH CENTRAL EQUATORIAL STATE, JUBA AND TOTTO CHAN TRAUMA CENTRE WITH FINANCIAL SUPPORT FROM DANIDA EED HIVOS NORWEGIAN COUNCIL FOR AFRICA/FOKUS SIGRID RAUSING TRUST UNIFEM SEPTEMBER, 2007 N E W S U D A N Central Equatorial Totto Chan We Link Women Internationally State Trauma Centre I Women’s Experiences during Armed Conflict in Southern Sudan, 1983 – 2005 TABLE OF CONTENTS Abbreviations........................................................................ iv List of Tables.......................................................................... v Authorship and Acknowledgement............................................ vi Executive Summary................................................................ ix CHAPTER ONE INTRODUCTION AND BACKGROUND TO THE STUDY 1.1 Introduction ............................................................... 1 1.2 Isis-WICCE Documentation........................................... 4 1.3 The Pre-Study Process ............................................... 4 1.4 Southern Sudan- Socio-Demographic Aspects .............. 4 1.5 Statement of the Problem .......................................... 5 1.6 Objectives .....................……………………………………… 7 1.7 Key Questions ........................................................... -

Ss 9301 Ee Torit County Map
SOUTH SUDAN Torit County map SUDAN Kapoeta North ETHIOPIA Ghaba CAR CENTRAL EQUATORIA Maitong DRC KENYA UGANDA Oheri Yegi Yegi Lafon Lokila Lotarang Ohilai Loronyo Fwara Husa Longija Makidi Losito 11 Juba Ogilate Omoro Langdimoleh Hidonge Ifura Lobithi Bari Lorieju Hutiala Osito Kidongi Gajawuru River Ongedon Lokila Lobuhi Losok Langario Mutaram Iswaha Pura Lofiri Kormus Bur Sauwo Muragatika Chalamni Kheba Longairo Buru Ilieu Lohira Torit New Keny Lohilo Momoi Hawai Oture Obule Dilen New Tirangore Hamuyang Kojopi Hatuloru Ibalami Payra Kidepo Italak Kaforere Tohubak Kateloro Olere Iddo Iloli Iyata Lohwa Lumo Torit Labalwa Tutumore Taudal Iluhum Enyiff EASTERN Lugurren Oguruny Hisiha Tabur Kinyeti Hai carton Irume Budi Isaloro Oguruny Fwara Loguto Tabuor EQUATORIA Egwi Ogire Ikulis Lomodik Iyedo Ngarama Farasika Lolianga Lobuli Mero Moti Oruho Kidol Lumudo Oruhoi Sunnat Lowudo Khartoum Imodongi Loudo Ohonyek Agoro Addui Ofong Ingama Lifa Hidiofo Oruho Omeyok Mobai Ogoto Kiliu Iromei Hinati Logonik Swurari Ipitari Iluma Loulang Gunyoro Kurmoz Ojek Logire Soyo Ogutu Ikara Soyo Hiwa Ikotos Osoro Makorro Edimang Tabwor Kimo Ohufa Iniela Gesiga Amiting Iheleng Hachalu Gong Mlgri Loping Ngabara Fwara Poli Wau Ingelire Fwara Bananiao Kwenda Labuge International boundary River Ogum Loguli Longwere River Ibobo State boundary Hoyuni County boundary Magwi Lotti Undetermined boundary Katiri Abyei region Upper Talanga Telanga Country capital State capital Administrative centre/County capital Kiteng Principal town Secondary town Issore Palwal Village Lomariti Primary road Secondary road Tertiary road Main river UGANDA 0 5 10 km The administrative boundaries and names shown and the designations used on this map do not imply official endorsement or acceptance by the United Nations. -

Community Driven Change Our Road Towards Peace
» REPORT NOVEMBER 2017 COMMUNITY DRIVEN CHANGE OUR ROAD TOWARDS PEACE EXPERIENCES FROM THE PROGRAM ‘INTERLINKING PEACEBUILDING, DECENTRALIZATION AND DEVELOPMENT’ OUR ROAD TOWARDS PEACE CONTENTS LIST OF ACRONYMS . 2 FOREWORD . 3 INTRODUCTION . 4 Context . 4 Approaches & Strategies . 5 HOW THIS PUBLICATION WAS MADE . 7 CASE STUDIES . 9 Peaceful Co-Existence among Farmers and Pastoralists . 9 Transforming a Culture Of Violence to a Culture Of Dialogue . 11 Disaster Risk Reduction Committees as Peace Agents . 13 Women Networks Fostering Human Security . 15 Women Sustaining Livelihoods . 17 A Safe Platform for Socio-Economic Empowerment . 19 “This is Big-Business” . 21 Water for Sustainable Peace . 23 Boosting Food Security . 25 Farming for Peaceful Co-Existence . .. 27 Skill Training for a Peaceful Future . 29 Youth become Peace Ambassadors . 31 FINDINGS & LESSONS LEARNED . 33 NOTES . .. 36 NOVEMBER 2017 © CORDAID 1 OUR ROAD TOWARDS PEACE LIST OF ACRONYMS LIST OF ACRONYMS CDoW Catholic Diocese of Wau CMDRR Community Managed Disaster Risk Reduction Cordaid Catholic Organization for Relief and Development Aid CPA Comprehensive Peace Agreement DRR Disaster Risk Reduction CSO Civil Society Organization EES Eastern Equatoria State GA Global Aim HARD Hope Agency for Relief and Development IDP Internally Displaced Persons IIRR International Institute of Rural Reconstruction PDRA Participatory Disaster Risk Assessment POC Protection of Civilians SARRA Solidarity Association for Rehabilitation and Recovery Affairs SGBV Sexual and Gender Based Violence -

Eastern Equatoria Torit, Eastern Equatoria
TORIT, EASTERN EQUATORIA TORIT, EASTERN EQUATORIA Village Assessment Survey County Profiles Village Assessment Survey Report (2013) | 1 VILLAGE ASSESSMENT SURVEY COUNTY PROFILES EASTERN EQUATORIA 2012 -2013 Torit Ikotos INTERNATIONAL ORGANIZATION FOR MIGRATION (IOM) The Village Assessment Survey (VAS) has been used by IOM since 2007 and is a comprehensive data source for South Sudan that provides granular data from 30 priority counties with the aim of informing reintegration assistance around basic services and infrastructure, livelihoods, land and shelter, WASH, education, health, and protection. The most recent VAS represents IOM’s largest effort to date and after consultations with the Government of South Sudan Relief and Rehabilitation Commission (RRC), UN agencies, and state-level partners, 30 priority counties were identified for the assessment. These comprise of 871 bomas, 197 payams, 468 health facilities, and 1,277 primary schools. There was a particular emphasis on assessing payams outside state capitals, where comparatively fewer comprehensive assessments have been carried out. IOM conducted the VAS in priority counties that represent an estimated 72% of the returnee population. Methodology The data presented are the results of four integrated questionnaires. At the boma level, a Boma Questionnaire gathered data in relation to basic services and socioeconomic conditions from boma committees, composed of the boma chief, as well as representatives of the youth, women, and returnees. In bomas where the Boma Questionnaire was being administered, separate Health and Education Technical Questionnaires were also distributed to healthcare workers and education administrators in order to capture specific data on the level of capacity and structure of public services provided to the boma. -

She Stands for Peace
SHEStands 20 YEARS, 20 JOURNEYS for Peace SHE Stands 20 YEARS, 20 JOURNEYS for Peace UNOAU United Nations Office to the African Union Norwegian Ministry of Foreign Affairs She Stands for Peace. 20 Years, 20 Journeys This book is jointly published by the United Nations Office to the African Union (UNOAU) and the African Union Commission (AUC), made possible by the generous support of the Government of the Kingdom of Norway. United Nations Office to the African Union (UNOAU), UNECA Compound, Menelik II Avenue, Zambezi Building 5th and 6th Floors, P.O. Box 1357, Addis Ababa, Ethiopia Website: https://unoau.unmissions.org Email: [email protected] African Union Commission P.O. Box 3243 Roosevelt Street (Old Airport Area), W21 K19, Addis Ababa, Ethiopia Website: https://au.int Email: [email protected] January 2020 This book commemorates 20 years of United Nations Security Council Resolution 1325 (2000). It captures 20 journeys of African women and organisations contributing to the implementation of the Women, Peace and Security agenda in Africa. Editorial consultant: Dr Yemisi Akinbobola Design, layout and cover printing: Phoenix Design Aid A/S (Denmark) The United Nations Security Council unanimously adopts Resolution 1325 (2000) calling for participation of women in the prevention, management, and resolution of conflict. The resolution calls on all actors involved to adopt a gender perspective when negotiating and implementing peace agreements, and further calls on all parties to armed conflict to fully respect international law applicable to the human rights of women and girls, as civilians and as refugees. A general view of the meeting as the vote is taken. -

Pdf | 393.38 Kb
Malek WARNING: Very little information is known Kolnyang E about the roads of South Sudan. If you have information to contribute, please LAKES JONGLEI contact [email protected]. H Gemmaiza I O Nanyangachor P Terakeka I Logono EASTERN EQUATORIA A Karotho Mangalla Kalimulinga Lafon Road Open for: Trailers (J>10u MTb) a Nanngolet CENTRAGllA oSnedaLsookn oEro QUATORIA Dry Season Only Mura Unknown Kapoeta Ngangala Lokolio post Trucks/Lorries (<10 MT) Liria Lohutok Kimotong Lologo All Season Loronyo Dry Season Only Iboni Nesitu Unknown Narus Longairo 4WD Only (< 3.5 MT) Okaru Chalamni Nadapal All Season Duro Tirangore DryS Sinedasiroun Only Unknown Lobira Unknown Torit All Season Kit Naqichot Gunyoro Dry Season Only Chukudum Natinga (new sit FagarUnknown Molongori K Lotome Karpeto Loguli New cush State Capital Magwi Nagishot Ikotos Kidepo Arado Palotaka E Primary Town Moli Gilo Lotukei Secondary Town N Mogiri Settlement/Village Upper talanga Y A Kerepi Opari Gaderu Shukoli Parajok KenyibaIntnl BUoluankdoary Lobone Tsertanya Mesika StaKte Baoujonda rKy eji Pageri Pugee Lofus JAorliemao MaPpompeojdu Bamurye Loa A Nimule D N A U G 0 10 20 30 40 50 Date Created: 8-FEB-2007 Proj/Datum: Geographic/WGS84 Kilometers R O A D S A N D S E T T L E M E N T S Map #: unjlc_sdn_706_A4L_EEQ GLIDE Num: The boundaries and names and the designations used on this map do not imply official E A S T E R N E Q U A T O R I A Scale 1:1,900,000 endorsement or acceptance by the United Nations. Some map data not verified. -

Village Assessment Survey Torit County
Village Assessment Survey COUNTY ATLAS 2013 Torit County Eastern Equatoria State Village Assessment Survey The Village Assessment Survey (VAS) has been used by IOM since 2007 and is a comprehensive data source for South Sudan that provides detailed information on access to basic services, infra- structure and other key indicators essential to informing the development of efficient reintegra- tion programmes. The most recent VAS represents IOM’s largest effort to date encompassing 30 priority counties comprising of 871 bomas, 197 payams, 468 health facilities, and 1,277 primary schools. There was a particular emphasis on assessing payams outside state capitals, where com- paratively fewer comprehensive assessments have been carried out. IOM conducted the assess- ment in priority counties where an estimated 72% of the returnee population (based on esti- mates as of 2012) has resettled. The county atlas provides spatial data at the boma level and should be used in conjunction with the VAS county profile. Two (2) Counties Assessed Planning Map and Dashboard..…………Page 1 WASH Section…………..………...Page 14 - 20 General Section…………...……...Page 2 - 5 Natural Source of Water……...……….…..Page 14 Main Ethnicities and Languages.………...Page 2 Water Point and Physical Accessibility….…Page 15 Infrastructure and Services……...............Page 3 Water Management & Conflict....….………Page 16 Land Ownership and Settlement Type ….Page 4 WASH Education...….……………….…….Page 17 Returnee Land Allocation Status..……...Page 5 Latrine Type and Use...………....………….Page 18 Livelihood