Fluorodopa F-18 [18F]FDOPA
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
PET Imaging of Occult Tumours by Temporal Integration of Tumour-Acidosis Signals from Ph-Sensitive 64Cu-Labelled Polymers
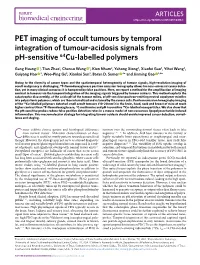
ARTICLES https://doi.org/10.1038/s41551-019-0416-1 PET imaging of occult tumours by temporal integration of tumour-acidosis signals from pH-sensitive 64Cu-labelled polymers Gang Huang 1, Tian Zhao1, Chensu Wang 1, Kien Nham2, Yahong Xiong2, Xiaofei Gao3, Yihui Wang3, Guiyang Hao 2, Woo-Ping Ge3, Xiankai Sun2, Baran D. Sumer 4* and Jinming Gao 1,4* Owing to the diversity of cancer types and the spatiotemporal heterogeneity of tumour signals, high-resolution imaging of occult malignancy is challenging. 18F-fluorodeoxyglucose positron emission tomography allows for near-universal cancer detec- tion, yet in many clinical scenarios it is hampered by false positives. Here, we report a method for the amplification of imaging contrast in tumours via the temporal integration of the imaging signals triggered by tumour acidosis. This method exploits the catastrophic disassembly, at the acidic pH of the tumour milieu, of pH-sensitive positron-emitting neutral copolymer micelles into polycationic polymers, which are then internalized and retained by the cancer cells. Positron emission tomography imaging of the 64Cu-labelled polymers detected small occult tumours (10–20 mm3) in the brain, head, neck and breast of mice at much higher contrast than 18F-fluorodeoxyglucose, 11C-methionine and pH-insensitive 64Cu-labelled nanoparticles. We also show that the pH-sensitive probes reduce false positive detection rates in a mouse model of non-cancerous lipopolysaccharide-induced inflammation. This macromolecular strategy for integrating tumour acidosis should enable improved cancer detection, surveil- lance and staging. ancer exhibits diverse genetic and histological differences tumours over the surrounding normal tissues often leads to false from normal tissues1. -

Epilepsy & Seizure
Epilepsy & Seizure Journal of Japan Epilepsy Society Vol.4 No.1 (2011) pp.15-25 Original Article Usefulness of 123I-iomazenil SPECT for childhood focal epilepsies 1) 1) 1) 1) Kentaro Okamoto, MD , Hirokazu Oguni, MD , Yoshiko Hirano, MD , Makiko Osawa, MD 1Department of Pediatrics, Tokyo Women's Medical University, 8-1 Kawada-cho, Shinjuku-ku, Tokyo 162-8666, Japan Key words: focal epilepsy, children, 123I-iomazenil SPECT, epileptic foci Published online July 29, 2011 Abstract Purpose: We investigated the usefulness of obtained from visualization of IMZ-SPECT 123I-iomazenil (IMZ-) SPECT to detect epilep- images and those speculated based on a com- tic foci in children with symptomatic focal bination of clinical manifestations, EEG find- epilepsy (SFE). ings, and brain MRI. We then verified the Subjects: 21 children with SFE who under- concordance of the results between the two went IMZ-SPECT to identify the epileptic fo- methods. cus were studied. Results: There was concordance in both later- Methods: We retrospectively compared the alization and localization in 9/12 patients with localization and lateralization of epileptic foci temporal lobe epilepsy (75%), in 2/5 patients Correspondence to: Hirokazu Oguni, MD, Department of Pediatrics, Tokyo Women's Medical University, 8-1 Kawada-cho, Shinjuku-ku, Tokyo 162, Japan Tel. 81-3-3353-8111, Fax. 81-3-5269-7338, [email protected] 15 Kentaro Okamoto, et al. IMZ-SPECT for childhood epilepsy with frontal lobe epilepsy (40%), and in 2/4 interictal/ictal cerebral blood flow single pho- patients with parieto-occipital lobe epilepsy ton emission computed tomography (SPECT) (50%). -

A Technique for Standardized Central Analysis of 6-18F-Fluoro-L-DOPA PET Data from a Multicenter Study
A Technique for Standardized Central Analysis of 6-18F-Fluoro-L-DOPA PET Data from a Multicenter Study Alan L. Whone, MRCP1; Dale L. Bailey, PhD2; Philippe Remy, PhD3; Nicola Pavese, MD1; and David J. Brooks, DSc1 1Division of Neuroscience and MRC Clinical Sciences Centre, Faculty of Medicine, Imperial College, Hammersmith Hospital, London, United Kingdom; 2Department of Nuclear Medicine, Royal North Shore Hospital, Sydney, Australia; and 3CEA-Centre National de la Recherche Scientifique Unite´ de Recherche Associe´e 2210, Service Hospitalier Frederic Joliot, Orsay, France tralized analysis offers the potential for improved detection of We have recently completed a large 6-18F-fluoro-L-DOPA (18F- outcomes due to the standardization of the analytic approach DOPA) PET study comparing rates of loss of dopamine terminal and allows the analysis of large numbers of PET studies. function in Parkinson’s disease (PD) patients taking either the Key Words: PET; 18F-DOPA; Parkinson’s disease; progression; dopamine agonist ropinirole or L-DOPA. This trial involved a central analysis “distributed acquisition/centralized analysis” method, in which J Nucl Med 2004; 45:1135–1145 18F-DOPA images were acquired at 6 different PET centers around the world and then analyzed at a single site. To our knowledge, this is the first time such a centralized approach has been employed with 18F-DOPA PET and this descriptive basic science article outlines the methods used. Methods: One hun- With rapid advances in molecular medicine, the pro- dred eighty-six PD patients were randomized (1:1) to ropinirole duction of neuroprotective or neurorestorative agents that or L-DOPA therapy, and 18F-DOPA PET was performed at base- affect the progression of degenerative conditions such as line and again at 2 y. -
![[123I]FP-CIT SPECT in Atypical Degenerative Parkinsonism](https://docslib.b-cdn.net/cover/2351/123i-fp-cit-spect-in-atypical-degenerative-parkinsonism-242351.webp)
[123I]FP-CIT SPECT in Atypical Degenerative Parkinsonism
CONTRAST AGENT EVALUATION [123I]FP-CIT SPECT in atypical degenerative parkinsonism One of the most widely used techniques to support the clinical diagnosis of Parkinson’s disease is the SPECT scan with [123I]FP-CIT. This tracer binds reversibly and visualizes the striatal presynaptic dopamine transporters. Several uncertainties remain on the value of [123I]FP-CIT and SPECT in atypical degenerative parkinsonian syndromes. In this concise review, we discuss the contribution of SPECT and [123I]FP-CIT in supporting the clinical diagnosis of Parkinson’s disease and their role in the differential diagnosis of Parkinson’s disease and atypical degenerative parkinsonism. The chemistry, pharmacodynamics and pharmacokinetics of [123I]FP-CIT are also discussed. 1,2,3 KEywordS: atypical degenerative parkinsonism n FP-CIT n ioflupane n SPECT Ioannis U Isaias* , Giorgio Marotta4, Gianni Pezzoli2, Parkinson’s disease (PD) is the second most dystonic tremor [15] and psychogenic parkin- Osama Sabri5 [1] [16,17] 5,6 common neurodegenerative disorder , yet sonism . In this concise review, we will & Swen Hesse 123 early accurate diagnosis remains challenging. discuss the role of SPECT and [ I]FP-CIT in 1Università degli Studi di Milano, The estimated prevalence of PD is 0.5–1% in supporting the clinical diagnosis of PD and its Dipartimento di Fisiologia Umana, those aged 65–69 years and 1–3% in those aged differential diagnosis with ADP. Milano, Italy 2Centro per la Malattia di Parkinson e i ≥80 years [1]. Although the clinical diagnosis of Disturbi del Movimento, -

Imaging in Parkinson's Disease
Clinical Medicine 2016 Vol 16, No 4: 371–5 CME MOVEMENT DISORDERS I m a g i n g i n P a r k i n s o n ’ s d i s e a s e Authors: G e n n a r o P a g a n o , A F l a v i a N i c c o l i n i B a n d M a r i o s P o l i t i s C The clinical presentation of Parkinson’s disease (PD) Abnormal intra-neuronal (Lewy bodies) and intra-neuritic is heterogeneous and overlaps with other conditions, (Lewy neurites) deposits of fibrillary aggregates are currently including the parkinsonian variant of multiple system considered the key neuropathological alterations in PD. atrophy (MSA-P), progressive supranuclear palsy (PSP) and The majority of these aggregates, mainly composed of alpha essential tremor. Imaging of the brain in patients with (α)−synuclein, are located at presynaptic level and impair ABSTRACT parkinsonism has the ability to increase the accuracy of axonal trafficking, resulting in a series of noxious events that differential diagnosis. Magnetic resonance imaging (MRI), cause neuronal damage to the substantia nigra pars compacta single photon emission computed tomography (SPECT) and with a subsequent dopaminergic denervation of the striatum. positron emission tomography (PET) allow brain imaging The cardinal motor features of PD (bradykinesia and rigidity, of structural, functional and molecular changes in vivo in with or without resting tremor) manifest after a substantial patients with PD. Structural MRI is useful to differentiate denervation of substantia nigra, which is associated with about PD from secondary and atypical forms of parkinsonism. -

DICOM Conformance Template
g GE Heathcare Technical Publications Direction 5507068-1EN (DOC1584283) Revision 1 DaTQUANT Application™ DICOM CONFORMANCE STATEMENT Copyright 2015 by General Electric Co. Do not duplicate g GE Heathcare LIST OF REVISIONS REV DATE DESCRIPTION PAGES APPR. 1 May 2015 Initial Release All M. Mesh DATQUANT APPLICATION GE Healthcare DICOM CONFORMANCE STATEMENT DIR 5507068-1EN (DOC1584283) REV 1 THIS PAGE LEFT INTENTIONALLY BLANK DATQUANT APPLICATION GE Healthcare DICOM CONFORMANCE STATEMENT DIR 5507068-1EN (DOC1584283) REV 1 CONFORMANCE STATEMENT OVERVIEW DaTQUANT application is an application that uses NM and CT images and creates NM, SC and MFSC images. Table 0.1 provides an overview of the network services supported by the DaTQUANT application. Table 0.1 – APPLICATION SOP Classes User of Object Creator of Instances Object Instances Transfer Secondary Capture Image Storage No Yes Multi-frame True Color Secondary Capture Image Storage No Yes Nuclear Medicine Image Storage Yes Yes Computerized Tomography Image Storage Yes No 4 DATQUANT APPLICATION GE Healthcare DICOM CONFORMANCE STATEMENT DIR 5507068-1EN (DOC1584283) REV 1 1. INTRODUCTION ............................................................................................................... 8 1.1 Overview ..................................................................................................................................................................... 8 1.2 Overall DICOM Conformance Statement Document Structure .......................................................................... -

Brain Imaging
Publications · Brochures Brain Imaging A Technologist’s Guide Produced with the kind Support of Editors Fragoso Costa, Pedro (Oldenburg) Santos, Andrea (Lisbon) Vidovič, Borut (Munich) Contributors Arbizu Lostao, Javier Pagani, Marco Barthel, Henryk Payoux, Pierre Boehm, Torsten Pepe, Giovanna Calapaquí-Terán, Adriana Peștean, Claudiu Delgado-Bolton, Roberto Sabri, Osama Garibotto, Valentina Sočan, Aljaž Grmek, Marko Sousa, Eva Hackett, Elizabeth Testanera, Giorgio Hoffmann, Karl Titus Tiepolt, Solveig Law, Ian van de Giessen, Elsmarieke Lucena, Filipa Vaz, Tânia Morbelli, Silvia Werner, Peter Contents Foreword 4 Introduction 5 Andrea Santos, Pedro Fragoso Costa Chapter 1 Anatomy, Physiology and Pathology 6 Elsmarieke van de Giessen, Silvia Morbelli and Pierre Payoux Chapter 2 Tracers for Brain Imaging 12 Aljaz Socan Chapter 3 SPECT and SPECT/CT in Oncological Brain Imaging (*) 26 Elizabeth C. Hackett Chapter 4 Imaging in Oncological Brain Diseases: PET/CT 33 EANM Giorgio Testanera and Giovanna Pepe Chapter 5 Imaging in Neurological and Vascular Brain Diseases (SPECT and SPECT/CT) 54 Filipa Lucena, Eva Sousa and Tânia F. Vaz Chapter 6 Imaging in Neurological and Vascular Brain Diseases (PET/CT) 72 Ian Law, Valentina Garibotto and Marco Pagani Chapter 7 PET/CT in Radiotherapy Planning of Brain Tumours 92 Roberto Delgado-Bolton, Adriana K. Calapaquí-Terán and Javier Arbizu Chapter 8 PET/MRI for Brain Imaging 100 Peter Werner, Torsten Boehm, Solveig Tiepolt, Henryk Barthel, Karl T. Hoffmann and Osama Sabri Chapter 9 Brain Death 110 Marko Grmek Chapter 10 Health Care in Patients with Neurological Disorders 116 Claudiu Peștean Imprint 126 n accordance with the Austrian Eco-Label for printed matters. -

Lettirs to Th Editor Radiation Injury from Interstitial Injection Of
DEPARTMENTS Lettirs to th Editor Radiation Injury from Interstitial Injection of measuring approximately 2 cm x 1 cm. Monitoring of the site Iodine-131-Iodocholesterol demonstrated retention of 131!(Fig. 2). On the basis of serial counts, the half-time was 5.5 days at the i.v. injection site. TO THE EDITOR: A 44-yr-oldman wasinvestigatedfor recur The absorbeddose deliveredto the overlyingskin cannot be rent Cushing's disease. An adrenal gland scan was initiated with precisely calculated because it has a very strong inverse depend injection of 34-MBq of ‘31I-iodocholesterol over a 5-mm interval. ence on the interstitial volume occupied by the injectate, and this Prior to injection, blood was withdrawn into the hub of the volume is not accurately known. The absorbed dose can be syringe to ensure correct i.v. placement. At the conclusion of the estimated by treating the interstitial volume occupied by the injection, the patient volunteered that the injection had been the injectate as a disk of the same area as the erythematous patch; least painful i.v. entry he had experienced. Seven days later, the thickness of this volume can be roughly estimated. The imaging failed to detect any radioactivity in the field of view volumeofdistributionwasassumedto remainconstantovertime centered on the adrenal glands. Monitoring of the injection site since the injectate is not water-soluble. The absorbed dose in this demonstrated essentially complete retention of the radiophar volume can be calculated by the method of Johns and Cun maceutical at the site. ningham (1). Because the model assumes no activity outside the The patient returned 13 days later (i.e., 20 days after the volume,the absorbeddose in the regionadjacentto this volume injection) to inquire about the tender pruritic and erythematous within the range of the beta particles (i.e., the skin) can be patch at the injection site at which time the photograph in Figure estimated to be halfthe dose inside the volume. -

Nuclear Medicine Imaging in Neuroblastoma: Current Status and New Developments
Journal of Personalized Medicine Review Nuclear Medicine Imaging in Neuroblastoma: Current Status and New Developments Atia Samim 1,2, Godelieve A.M. Tytgat 1, Gitta Bleeker 3, Sylvia T.M. Wenker 1,2, Kristell L.S. Chatalic 1,2, Alex J. Poot 1,2, Nelleke Tolboom 1,2, Max M. van Noesel 1 , Marnix G.E.H. Lam 2 and Bart de Keizer 1,2,* 1 Princess Maxima Center for Pediatric Oncology, Heidelberglaan 25, 3584 CS Utrecht, The Netherlands; [email protected] (A.S.); [email protected] (G.A.M.T.); [email protected] (S.T.M.W.); [email protected] (K.L.S.C.); [email protected] (A.J.P.); [email protected] (N.T.); [email protected] (M.M.v.N.) 2 Department of Radiology and Nuclear Medicine, University Medical Center Utrecht/Wilhelmina Children’s Hospital, Heidelberglaan 100, 3584 CX Utrecht, The Netherlands; [email protected] 3 Department of Radiology and Nuclear Medicine, Northwest Clinics, Wilhelminalaan 12, 1815 JD Alkmaar, The Netherlands; [email protected] * Correspondence: [email protected]; Tel.: +31-887-571-794 Abstract: Neuroblastoma is the most common extracranial solid malignancy in children. At diagnosis, approximately 50% of patients present with metastatic disease. These patients are at high risk for refractory or recurrent disease, which conveys a very poor prognosis. During the past decades, Citation: Samim, A.; Tytgat, G.A.M.; nuclear medicine has been essential for the staging and response assessment of neuroblastoma. 123 123 Bleeker, G.; Wenker, S.T.M.; Currently, the standard nuclear imaging technique is meta-[ I]iodobenzylguanidine ([ I]mIBG) Chatalic, K.L.S.; Poot, A.J.; whole-body scintigraphy, usually combined with single-photon emission computed tomography Tolboom, N.; van Noesel, M.M.; with computed tomography (SPECT-CT). -

Nuclear Pharmacy Quick Sample
12614-01_CH01-rev3.qxd 10/25/11 10:56 AM Page 1 CHAPTER 1 Radioisotopes Distribution for Not 1 12614-01_CH01-rev3.qxd 10/25/1110:56AMPage2 2 N TABLE 1-1 Radiopharmaceuticals Used in Nuclear Medicine UCLEAR Chemical Form and Typical Dosage P Distribution a b HARMACY Radionuclide Dosage Form Use (Adult ) Route Carbon C 11 Carbon monoxide Cardiac: Blood volume measurement 60–100 mCi Inhalation Carbon C 11 Flumazenil injection Brain: Benzodiazepine receptor imaging 20–30 mCi IV Q UICK Carbon C 11 Methionine injection Neoplastic disease evaluation in brain 10–20 mCi IV R Carbon C 11 forRaclopride injection Brain: Dopamine D2 receptor imaging 10–15 mCi IV EFERENCE Carbon C 11 Sodium acetate injection Cardiac: Marker of oxidative metabolism 12–40 mCi IV Carbon C 14 Urea Diagnosis of Helicobacter pylori infection 1 µCi PO Chromium Cr 51 Sodium chromate injection Labeling red blood cells (RBCs) for mea- 10–80 µCi IV suring RBC volume, survival, and splenic sequestration Cobalt Co 57 Cyanocobalamin capsules Diagnosis of pernicious anemia and 0.5 µCi PO Not defects of intestinal absorption Fluorine F 18 Fludeoxyglucose injection Glucose utilization in brain, cardiac, and 10–15 mCi IV neoplastic disease Fluorine F 18 Fluorodopa injection Dopamine neuronal decarboxylase activity 4–6 mCi IV in brain Fluorine F 18 Sodium fluoride injection Bone imaging 10 mCi IV Gallium Ga 67 Gallium citrate injection Hodgkin’s disease, lymphoma 8–10 mCi IV Acute inflammatory lesions 5 mCi IV Indium In 111 Capromab pendetide Metastatic imaging in patients with biopsy- -

(18F-FDG) Uptake for PET/CT in Normal Organs
www.nature.com/scientificreports OPEN Efects of blood glucose level on 18F fuorodeoxyglucose (18F- FDG) uptake for PET/CT in normal Received: 24 October 2017 Accepted: 18 January 2018 organs: an analysis on 5623 Published: xx xx xxxx patients Clarice Sprinz1,2, Matheus Zanon 3,4, Stephan Altmayer3,4, Guilherme Watte 3, Klaus Irion 5, Edson Marchiori 6 & Bruno Hochhegger 2,3,4 Our purpose was to evaluate the efect of glycemia on 18F-FDG uptake in normal organs of interest. The infuences of other confounding factors, such as body mass index (BMI), diabetes, age, and sex, on the relationships between glycemia and organ-specifc standardized uptake values (SUVs) were also investigated. We retrospectively identifed 5623 consecutive patients who had undergone clinical PET/ CT for oncological indications. Patients were stratifed into groups based on glucose levels, measured immediately before 18F-FDG injection. Diferences in mean SUVmax values among glycemic ranges were clinically signifcant only when >10% variation was observed. The brain was the only organ that presented a signifcant inverse relationship between SUVmax and glycemia (p < 0.001), even after controlling for diabetic status. No such diference was observed for the liver or lung. After adjustment for sex, age, and BMI, the association of glycemia with SUVmax was signifcant for the brain and liver, but not for the lung. In conclusion, the brain was the only organ analyzed showing a clinically signifcant relationship to glycemia after adjustment for potentially confounding variables. The lung was least afected by the variables in our model, and may serve as an alternative background tissue to the liver. -

Initial Clinical Comparison of 18F-Florbetapir and 18F-FDG PET in Patients with Alzheimer Disease and Controls
Journal of Nuclear Medicine, published on May 10, 2012 as doi:10.2967/jnumed.111.099606 Initial Clinical Comparison of 18F-Florbetapir and 18F-FDG PET in Patients with Alzheimer Disease and Controls Andrew B. Newberg1, Steven E. Arnold2, Nancy Wintering1, Barry W. Rovner1, and Abass Alavi2 1Thomas Jefferson University and Hospital, Philadelphia, Pennsylvania; and 2University of Pennsylvania, Philadelphia, Pennsylvania The purpose of this study was to determine how clinical inter- Alzheimer disease (AD) is a brain disorder of older pretations of the 18F-amyloid tracer florbetapir compares diagnos- adults, with symptoms of progressive decline in memory 18 tically with F-FDG PET when evaluating patients with Alzheimer and other cognitive functions. A definitive diagnosis of AD disease (AD) and controls. Methods: Nineteen patients with a clin- ical diagnosis of AD and 21 elderly controls were evaluated with can be established only by demonstrating the presence of both 18F-florbetapir and 18F-FDG PET scans. Scans were inter- abundant senile plaques and neurofibrillary tangles in post- preted together by 2 expert readers masked to any case informa- mortem brain sections (1,2). During life, most patients are tion and were assessed for tracer binding patterns consistent with diagnosed by clinical criteria that imperfectly track with AD. The criteria for interpreting the 18F-florbetapir scan as positive postmortem pathologic findings. The criteria for the diagno- for AD was the presence of binding in the cortical regions relative to sis of AD were defined by the Working Group of the Na- the cerebellum. 18F-FDG PET scans were interpreted as positive if they displayed the classic pattern of hypometabolism in the tem- tional Institute of Neurologic and Communicative Disorders poroparietal regions.