The Use of Titanium in Dentistry
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Repoussé Work for Amateurs
rf Bi oN? ^ ^ iTION av op OCT i 3 f943 2 MAY 8 1933 DEC 3 1938 MAY 6 id i 28 dec j o m? Digitized by the Internet Archive in 2011 with funding from Boston Public Library http://www.archive.org/details/repoussworkforamOOhasl GROUP OF LEAVES. Repousse Work for Amateurs. : REPOUSSE WORK FOR AMATEURS: BEING THE ART OF ORNAMENTING THIN METAL WITH RAISED FIGURES. tfjLd*- 6 By L. L. HASLOPE. ILLUSTRATED. LONDON L. UPCOTT GILL, 170, STRAND, W.C, 1887. PRINTED BY A. BRADLEY, 170, STRAND, LONDON. 3W PREFACE. " JjJjtfN these days, when of making books there is no end," ^*^ and every description of work, whether professional or amateur, has a literature of its own, it is strange that scarcely anything should have been written on the fascinating arts of Chasing and Repousse Work. It is true that a few articles have appeared in various periodicals on the subject, but with scarcely an exception they treated only of Working on Wood, and the directions given were generally crude and imperfect. This is the more surprising when we consider how fashionable Repousse Work has become of late years, both here and in America; indeed, in the latter country, "Do you pound brass ? " is said to be a very common question. I have written the following pages in the hope that they might, in some measure, supply a want, and prove of service to my brother amateurs. It has been hinted to me that some of my chapters are rather "advanced;" in other words, that I have gone farther than amateurs are likely to follow me. -

Metals and Metal Products Tariff Schedules of the United States
251 SCHEDULE 6. - METALS AND METAL PRODUCTS TARIFF SCHEDULES OF THE UNITED STATES SCHEDULE 6. - METALS AND METAL PRODUCTS 252 Part 1 - Metal-Bearing Ores and Other Metal-Bearing Schedule 6 headnotes: Materials 1, This schedule does not cover — Part 2 Metals, Their Alloys, and Their Basic Shapes and Forms (II chemical elements (except thorium and uranium) and isotopes which are usefully radioactive (see A. Precious Metals part I3B of schedule 4); B. Iron or Steel (II) the alkali metals. I.e., cesium, lithium, potas C. Copper sium, rubidium, and sodium (see part 2A of sched D. Aluminum ule 4); or E. Nickel (lii) certain articles and parts thereof, of metal, F. Tin provided for in schedule 7 and elsewhere. G. Lead 2. For the purposes of the tariff schedules, unless the H. Zinc context requires otherwise — J. Beryllium, Columbium, Germanium, Hafnium, (a) the term "precious metal" embraces gold, silver, Indium, Magnesium, Molybdenum, Rhenium, platinum and other metals of the platinum group (iridium, Tantalum, Titanium, Tungsten, Uranium, osmium, palladium, rhodium, and ruthenium), and precious- and Zirconium metaI a Iloys; K, Other Base Metals (b) the term "base metal" embraces aluminum, antimony, arsenic, barium, beryllium, bismuth, boron, cadmium, calcium, chromium, cobalt, columbium, copper, gallium, germanium, Part 3 Metal Products hafnium, indium, iron, lead, magnesium, manganese, mercury, A. Metallic Containers molybdenum, nickel, rhenium, the rare-earth metals (Including B. Wire Cordage; Wire Screen, Netting and scandium and yttrium), selenium, silicon, strontium, tantalum, Fencing; Bale Ties tellurium, thallium, thorium, tin, titanium, tungsten, urani C. Metal Leaf and FoU; Metallics um, vanadium, zinc, and zirconium, and base-metal alloys; D, Nails, Screws, Bolts, and Other Fasteners; (c) the term "meta I" embraces precious metals, base Locks, Builders' Hardware; Furniture, metals, and their alloys; and Luggage, and Saddlery Hardware (d) in determining which of two or more equally specific provisions for articles "of iron or steel", "of copper", E. -

A Review on Nickel Titanium and It's Biomedical Applications
International Research Journal of Engineering and Technology (IRJET) e-ISSN: 2395-0056 Volume: 07 Issue: 09 | Sep 2020 www.irjet.net p-ISSN: 2395-0072 A Review on Nickel Titanium and it’s Biomedical Applications Agnesh Rao K1, Ayush Kothari2, Dhanush L Prakash3, Jeevan S Hallikeri4, Nesar V Shetty5 1,2,3,4,5Bachelor’s in Mechanical Engineering, Dept. of Mechanical Engineering, BNM Institute of Technology, Karnataka, India ------------------------------------------------------------------------***----------------------------------------------------------------------- Abstract - NiTinol is a super alloy that has influenced Fields like Aeronautics and Biomedicine. Modern Medicine tremendous change in science and technology, since its has accepted and acknowledged the usage of Shape Memory inception in 1959. It has provided novel solutions to our pre- Alloys. Industrial and commercial applications of SMA haven’t existing challenges and has affected many fields in our been exploited still but rather given trivial importance. This paper pertains only to Nitinol, Its properties and its scientific community bringing funding for research and applications in the field of Biomedical Engineering. positively impacting many industries to help in their development. One such impact is in the bio medical industry. The bio medical industry is the most fast paced section of our 1.2 An Overview about the Material Science of scientific community and sees a lot of development in a short Nickel-Titanium Alloy span of time. This review provides an understanding of the history, manufacturing methods, shape memory effect and the use of NiTinol in biomedicine & orthodontics; how NiTinol has William J. Buehler along with Frederick Wang, discovered the helped improve pre-existing solutions to medical problems that SME of Nitinol and its properties during research at the Naval affect a large demographic and how NiTinol has helped in Ordnance Laboratory in 1959. -

The Aerospace Applications of Nickel-Titanium As a Superelastic Material
Session A8 Paper #3 Disclaimer—This paper partially fulfills a writing requirement for first year (freshman) engineering students at the University of Pittsburgh Swanson School of Engineering. This paper is a student, not a professional, paper. This paper is based on publicly available information and may not provide complete analyses of all relevant data. If this paper is used for any purpose other than these authors’ partial fulfillment of a writing requirement for first year (freshman) engineering students at the University of Pittsburgh Swanson School of Engineering, the user does so at his or her own risk. THE AEROSPACE APPLICATIONS OF NICKEL-TITANIUM AS A SUPERELASTIC MATERIAL Arsha Mamoozadeh, [email protected], Mena 1:00, Nick Fratto, [email protected], Mena 1:00 Abstract—Nickel-titanium, commonly referred to as Nitinol, is The alloy is called Nitinol, named from its two key ingredients a shape-memory alloy with superelastic properties that make (nickel and titanium), and from its place of discovery at the it useful in certain environments and applications. These Naval Ordnance Laboratory in White Oak, Maryland [1]. properties include shape-memory, flexibility, and durability. Nitinol has superelastic properties that manifest in increased Titanium, a primary material, is a material that reacts with flexibility and durability, as well as the shape-memory carbon and oxygen when molten and is not easy to work with. properties, which allow the material to change shape during a Consequently, there are two commercially viable methods for heat treatment processes. All these properties can be adjusted producing Nitinol that account for titanium’s reactivity: by adding other materials and making a more complicated vacuum induction melting and vacuum arc re-melting. -

Antibacterial Property and Biocompatibility of Silver, Copper, and Zinc in Titanium Dioxide Layers Incorporated by One-Step Micro-Arc Oxidation: a Review
antibiotics Review Antibacterial Property and Biocompatibility of Silver, Copper, and Zinc in Titanium Dioxide Layers Incorporated by One-Step Micro-Arc Oxidation: A Review Masaya Shimabukuro Department of Biomaterials, Faculty of Dental Science, Kyushu University, 3-1-1 Maidashi, Higashi-ku, Fukuoka 812-8582, Japan; [email protected]; Tel.: +81-92-642-6346 Received: 3 October 2020; Accepted: 19 October 2020; Published: 20 October 2020 Abstract: Titanium (Ti) and its alloys are commonly used in medical devices. However, biomaterial-associated infections such as peri-implantitis and prosthetic joint infections are devastating and threatening complications for patients, dentists, and orthopedists and are easily developed on titanium surfaces. Therefore, this review focuses on the formation of biofilms on implant surfaces, which is the main cause of infections, and one-step micro-arc oxidation (MAO) as a coating technology that can be expected to prevent infections due to the implant. Many researchers have provided sufficient data to prove the efficacy of MAO for preventing the initial stages of biofilm formation on implant surfaces. Silver (Ag), copper (Cu), and zinc (Zn) are well used and are incorporated into the Ti surface by MAO. In this review, the antibacterial properties, cytotoxicity, and durability of these elements on the Ti surface incorporated by one-step MAO will be summarized. This review is aimed at enhancing the importance of the quantitative control of Ag, Cu, and Zn for their use in implant surfaces and the significance of the biodegradation behavior of these elements for the development of antibacterial properties. Keywords: titanium; biofilm; infection; micro-arc oxidation; silver; copper; zinc; antibacterial properties; coating; implant 1. -

Multi-Objective Optimization of Micro-Electrical Discharge Machining of T Nickel-Titanium-Based Shape Memory Alloy Using MOGA-II ⁎ Mustufa H
Measurement 125 (2018) 336–349 Contents lists available at ScienceDirect Measurement journal homepage: www.elsevier.com/locate/measurement Multi-objective optimization of micro-electrical discharge machining of T nickel-titanium-based shape memory alloy using MOGA-II ⁎ Mustufa H. Abidia, Abdulrahman M. Al-Ahmaria,b, Usama Umera, , Mohammed Sarvar Rasheedc a Princess Fatima Alnijris Research Chair for Advanced Manufacturing Technology (FARCAMT Chair), Advanced Manufacturing Institute, King Saud University, Riyadh, Saudi Arabia b Industrial Engineering Department, College of Engineering, King Saud University, Riyadh, Saudi Arabia c Baynounah Institute of Science and Technology, Abu Dhabi Vocational Education Training Institute, Madinat Zayed, Abu Dhabi, United Arab Emirates ARTICLE INFO ABSTRACT Keywords: Shape memory alloys (SMAs) have received significant attention especially in biomedical and aerospace in- Micro-EDM (µEDM) dustries owing to their unique properties. However, they are difficult-to-machine materials. Electrical discharge Micro-machining machining (EDM) can be used to machine difficult to cut materials with good accuracy. However, several Shape memory alloy challenges and issues related with the process at micro-level continue to exist. One of the aforementioned issues MOGA-II is that the micro-EDM (µEDM) process is extremely slow when compared to other non-conventional processes, such as laser machining, although it offers several other benefits. The study considers the analysis and opti- mization of µEDM by using a multi-objective genetic algorithm (MOGA-II). Drilling of micro-holes is performed by using a tabletop electrical discharge machine. Nickel-Titanium (Ni-Ti) based SMA (a difficult to cut advance material) is used as a specimen. The objective involves determining optimal machining parameters to obtain better material removal rate with good surface finish. -
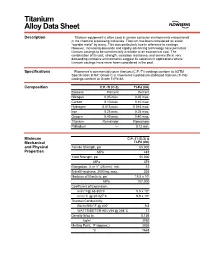
Titanium Alloy Data Sheet
M Titanium Alloy Data Sheet Description Titanium equipment is often used in severe corrosive environments encountered in the chemical processing industries. Titanium has been considered an exotic “wonder metal” by many. This was particularly true in reference to castings. However, increasing demands and rapidly advancing technology have permitted titanium castings to be commercially available at an economical cost. The combination of its cost, strength, corrosion resistance, and service life in very demanding corrosive environments suggest its selection in applications where titanium castings have never been considered in the past. Specifications Flowserve’s commercially pure titanium (C.P.-Ti) castings conform to ASTM Specification B367, Grade C-3. Flowserve’s palladium stabilized titanium (Ti-Pd) castings conform to Grade Ti-Pd 8A. Composition C.P.-Ti (C-3) Ti-Pd (8A) Element Percent Percent Nitrogen 0.05 max. 0.05 max. Carbon 0.10 max. 0.10 max. Hydrogen 0.015 max. 0.015 max. Iron 0.25 max. 0.25 max. Oxygen 0.40 max. 0.40 max. Titanium Remainder Remainder Palladium –– 0.12 min. Minimum C.P.-Ti (C-3) & Mechanical Ti-Pd (8A) and Physical Tensile Strength, psi 65,000 Properties MPa 448 Yield Strength, psi 55,000 MPa 379 Elongation, % in 1" (25 mm), min. 12 Brinell Hardness, 3000 kg, max. 235 Modulus of Elasticity, psi 15.5 x 106 MPa 107,000 Coefficient of Expansion, in/in/°F@ 68-800°F 5.5 x 10-6 m/m/°C @ 20-427°C 9.9 x 10-6 Thermal Conductivity, Btu/hr/ft/ft2/°F @ 400° 9.8 WATTS/METER-KELVIN @ 204°C 17 Density lb/cu in 0.136 kg/m3 3760 Melting Point, °F (approx.) 3035 °C 1668 Titanium Alloy Data Sheet (continued) Corrosion The outstanding mechanical and physical properties of titanium, combined with its Resistance unexpected corrosion resistance in many environments, makes it an excellent choice for particularly aggressive environments like wet chlorine, chlorine dioxide, sodium and calcium hypochlorite, chlorinated brines, chloride salt solutions, nitric acid, chromic acid, and hydrobromic acid. -

Invictus Catalog Lowres.Pdf
At Invictus Body Jewelry we believe that professional piercers and body modifi cation artists desire high quality, implant grade jewelry at a reasonable price. To accomplish this, we designed and developed Invictus Body Jewelry to supply implant grade titanium jewelry to professional piercers all over the world. Invictus Body Jewelry is manufactured out of Ti 6Al-4V ELI ASTM F-136 implant grade titanium. All of our jewelry is internally threaded and adheres to industry standard thread patterns. At Invictus Body Jewelry we strive to provide the professional piercer with safe, customizable, and affordable implant grade jewelry. 2 www.invictusbodyjewelry.com Invictus Body Jewelry is manufactured only using implant grade materials - Ti 6Al-4V ELI ASTM-F136. All Invictus Body Jewelry products are internally threaded for professional piercers and their clients. Invictus Body Jewelry uses industry standard thread patterns. We use M1.2 threading on our 14ga and M0.9 threading on our 16ga & 18ga. We believe in providing quality piercing products at reasonable prices to our customers. We fulfi ll orders within 24 to 48 hours from being entered into the system. Invictus Body Jewelry is only available to wholesale customers. Only piercing shops and retailers may purchase our products, not the general public. 203.803.1129 3 HORSESHOES & CURVES TIHI (Internally Threaded Titanium Horseshoes) TICI (Internally Threaded Titanium Curves) CodeSizeDiameter Ends Code Size Diameter Ends TIHI601 16g 1/4” 3mm TIHI411 14g 5/16” 4mm TIHI611 16g 5/16” 3mm TIHI421 -

Stainless Steel Activator for Gold
CASWELL 7696 Route 31, Lyons NY 14489 Voice - (315) 946-1213 Fax - (315) 946-4456 Www.caswellplating.com [email protected] STAINLESS STEEL ACTIVATOR FOR GOLD 1. Fill a one quart or 1000 ml beaker nearly full with Activator-SS. 2. Check solution temperature to assure it is between 80-100 degrees Fahrenheit. 3. Check connections from power supply to anode and work to be sure the negative (-) and positive (+) wires are connected properly. • The work should be charged negative (-), and the anode positive (+). • Use a Stainless Steel Anode 4. Turn rectifier on. 5. Activate at 6-8 volts for 45-60 seconds depending on size of part. Part should be completely clean prior to further plating. 6. Larger parts require slightly higher voltage, while smaller parts require lower voltage. If part shows any burning such as dark or gray deposits around the edges, you are burning the part and must lower the voltage. If part is not cleaning after two minutes, voltage is too low, therefore, increase voltage slightly. 7. After Activating, rinse part thoroughly in water and continue the plating process with Fastgold brush plating or Caswell Tank Plating Gold at 140 degrees Fahrenheit. Plate 15- 30 seconds longer than normal. 8. If you are not going to continue the plating process immediately, then dry the part thoroughly. When you continue the plating process, re-activate the part in Activator~SS to assure better adhesion. 9. Change solution when Activator-55 becomes inactive, reaches a pH higher than 2, or noticeably dirty. Discard &: Replace: Activator-SSTM is a rugged solution and is designed to help assure long life. -

Gold - Silver Ratio Investors’ Perspective
Gold - Silver Ratio Investors’ Perspective Gold and Silver Prices Jan 2000 - Aug 2011 50 y = 3.2481e0.0016x Here’s a fresh, 45 R² = 0.92 in depth look at the 40 important gold-silver ratio indicator with tell-all charts 35 y = 0.0209x - 2.0747 and ideas to help you inter- 30 R² = 0.8949 pret the ratio and trade the pair. Keep in mind that the 25 y = 13.138ln(x) - 71.585 By: Przemyslaw Radomski - Chief Investment - Chief Radomski Investment By: Przemyslaw Autor Stall - Contibuting Mike and Strategist Profits Sunshine Investments Silver & Effective Gold for Tools majority of investors lose, R² = 0.7914 and that successfully playing Silver ($/oz) 20 the game in the markets is about doing 15 things that the majority does not. In order to outsmart the majority, we need to look 10 at the gold silver ratio in a unique way. 5 The gold-silver ratio is one of the first indi- 0 200 400 600 800 1000 1200 1400 1600 1800 cators traders look at to comprehend the state of the precious metals market. In- Gold ($/oz) deed, it has been out of favor among mod- Chart 1: Gold and Silver Prices ern investors who believe that a simple sinusoidal (smooth repetitive oscillation) instead of standard gold/silver and time started in 2000) is best represented by a movement does not often work. axis does not give you a clear idea about linear trend line, so the trend line is rising the ratio extremities, but it shows a clear and the slope is constant. -

Investment Casting Or the Lost Wax Process
Investment Casting or The Lost Wax Process Apecs Investment Castings was founded in 1963 and is now situated in the Melbourne suburb of Burwood where we have been since we outgrew our Canterbury factory in August 1987. The company name (APECS), stands for Anthony Philip Eccles Casting Service. Investment is a type of plaster that we use in our process of reproducing multiple copies of an original master pattern which is usually supplied to us by our customers. This is a classic 18ct yellow gold emerald and diamond ring taken from the Apecs catalogue. The next series of photos will show the steps involved in producing multiple copies of this ring. An original master pattern is designed and fabricated by our customers and supplied to us to reproduce in the quantities and metals of their choice. It is important to ensure that the master is made as accurately as possible and to pay particular attention to the finish of the master pattern. The better the quality of the master pattern the better the casting result. The finished master pattern ready for the caster. A picture of the master pattern is drawn and a mould number is allocated for identification. When the customer wants to reorder he quotes the mould number for the pattern he wants. A sprue is soldered onto the pattern. This sprue enables the pattern to be easily located in the mould and will provide the path for the wax to be injected into the rubber mould. To make a mould the master pattern is placed between sheets of uncured vulcanising rubber. -

The Precious Metal Account Timeless Investments – Securely Managed
The Precious Metal Account Timeless Investments – Securely Managed Everything You Need to Know about Your Benefits the Precious Metal Account • You benefit from a clear investment in account form This solution provides a simple form of investment for book- • It is possible to convert your credit into physical precious entry balances in precious metal accounts and is managed metal at any time in the currency of the relevant precious metal (gold, silver, platinum, or palladium) in ounces.1 The precious metal Potential Risks account is attractive for investors with frequent trading activity • Precious metals are subject to currency and price fluctua- (purchase/sale of precious metals). tions and are therefore only suitable for investors who are able and willing to take on a certain amount of risk The key points at a glance: • In contrast to custody in a safekeeping account, credit in • Ability to transfer balances in precious metal accounts, both the precious metal account would be classed as bankruptcy within Credit Suisse and to other banks estate in the event of bankruptcy • Balances in precious metal accounts are managed in book form, in contrast to investments in safekeeping accounts Conditions • Credit can be converted into physical precious metal at any time, subject to a charge Currency Gold (XAU), silver (XAG), platinum (XPT), palladium (XPD) Your Needs Charges2 0.80% (all metals) p.a. • You want to diversify your portfolio Min. CHF 100 p.a. • You want an overview of your balances in precious metal Conversion into or Charges vary depending on the weight and accounts at all times delivery as physical the service required.