Zirconium-Dioxide As Preferred Material for Dental Implants a Narrative Review: Part I
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

The Riches of Uranium Uranium Is Best Known, and Feared, for Its Involvement in Nuclear Energy
in your element The riches of uranium Uranium is best known, and feared, for its involvement in nuclear energy. Marisa J. Monreal and Paula L. Diaconescu take a look at how its unique combination of properties is now increasingly attracting the attention of chemists. t is nearly impossible to find an uplifting, and can be arrested by the skin, making found about uranium’s superior catalytic funny, or otherwise endearing quote on depleted uranium (composed mainly of 238U) activity may not be an isolated event. The Iuranium — the following dark wisecrack1 safe to work with as long as it is not inhaled organometallic chemistry of uranium was reflects people’s sinister feelings about this or ingested. born during the ‘Manhattan project’ — code element: “For years uranium cost only a few Studying the fundamental chemistry of name of the development of the first nuclear dollars a ton until scientists discovered you uranium is an exotic endeavour, but those who weapon during the Second World War. This could kill people with it”. But, in the spirit of embrace it will reap its benefits. Haber and field truly began to attract interest in 1956 rebranding, it is interesting to note that the Bosch found that uranium was a better catalyst when Reynolds and Wilkinson reported the main source of Earth’s internal heat comes than iron for making ammonia2. The preparation of the first cyclopentadienyl from the radioactive decay of uranium, isolation of an η1-OCO complex derivatives6. The discovery of thorium and potassium-40 that keeps the of uranium3 also showed uranocene electrified the field outer core liquid, induces mantle convection that, even though it is as much as that of ferrocene and, subsequently, drives plate tectonics. -

Project Note Weston Solutions, Inc
PROJECT NOTE WESTON SOLUTIONS, INC. To: Canadian Radium & Uranium Corp. Site File Date: June 5, 2014 W.O. No.: 20405.012.013.2222.00 From: Denise Breen, Weston Solutions, Inc. Subject: Determination of Significant Lead Concentrations in Sediment Samples References 1. New York State Department of Environmental Conservation. Technical Guidance for Screening Contaminated Sediments. March 1998. [45 pages] 2. U.S. Environmental Protection Agency (EPA) Office of Emergency Response. Establishing an Observed Release – Quick Reference Fact Sheet. Federal Register, Volume 55, No. 241. September 1995. [7 pages] 3. International Union of Pure and Applied Chemistry, Inorganic Chemistry Division Commission on Atomic Weights and Isotopic Abundances. Atomic Weights of Elements: Review 2000. 2003. [120 pages] WESTON personnel collected six sediment samples (including one environmental duplicate sample) from five locations along the surface water pathway of the Canadian Radium & Uranium Corp. (CRU) site in May 2014. The sediment samples were analyzed for Target Analyte List (TAL) Metals and Stable Lead Isotopes. 1. TAL Lead Interpretation: In order to quantify the significance for Lead, Thallium and Mercury the following was performed: 1. WESTON personnel tabulated all available TAL Metal data from the May 2014 Sediment Sampling event. 2. For each analyte of concern (Lead, Thallium, and Mercury), the highest background concentration was selected and then multiplied by three. This is the criteria to find the significance of site attributable release as per Hazard Ranking System guidelines. 3. One analytical lead result (2222-SD04) of 520 mg/kg (J) was qualified with an unknown bias. In accordance with US EPA document “Using Data to Document an Observed Release and Observed Contamination”, 2222-SD03 lead concentration was adjusted by dividing by the factor value for lead of 1.44 to equal 361 mg/kg. -

RBRC-32 BNL-6835.4 PARITY ODD BUBBLES in HOT QCD D. KHARZEEV in This ~A~Er We Give a Pedawwicalintroduction~0 Recent Work Of
RBRC-32 BNL-6835.4 PARITY ODD BUBBLES IN HOT QCD D. KHARZEEV RIKEN BNL Research Center, Br$ookhauenNational Laboratory, . Upton, New York 11973-5000, USA R.D. PISARSKI Department of Physics, Brookhaven National Laboratoy, Upton, New York 11973-5000, USA M.H.G. TYTGAT Seruice de Physique Th&orique, (7P 225, Uniuersitc4Libre de Bruzelles, B[ud. du !t%iomphe, 1050 Bruxelles, Belgium We consider the topological susceptibility for an SU(N) gauge theory in the limit of a large number of colors, N + m. At nonzero temperature, the behavior of the topological susceptibility depends upon the order of the reconfining phrrse transition. The meet interesting possibility is if the reconfining transition, at T = Td, is of second order. Then we argue that Witten’s relation implies that the topological suscepti~lfity vanishes in a calculable fdion at Td. Ae noted by Witten, this implies that for sufficiently light quark messes, metaetable etates which act like regions of nonzero O — parity odd bubbles — can arise at temperatures just below Td. Experimentally, parity odd bubbles have dramatic signature% the rI’ meson, and especially the q meson, become light, and are copiously produced. Further, in parity odd bubbles, processes which are normally forbidden, such as q + rr”ro, are allowed. The most direct way to detect parity violation is by measuring a parity odd global seymmetry for charged pions, which we define. 1 Introduction In this .-~a~er we give a Pedawwicalintroduction~0 recent work of ours? We I consider an SU(IV) gau”ge t~e~ry in the limit of a large number of colors, N + co, This is, of course, a familiar limit? We use the large N expansion I to investigate the behavior of the theory at nonzero temperature, especially for the topological susceptibility. -
Hexagon Fall
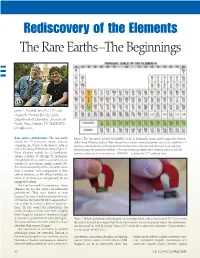
Redis co very of the Elements The Rare Earth s–The Beginnings I I I James L. Marshall, Beta Eta 1971 , and Virginia R. Marshall, Beta Eta 2003 , Department of Chemistry, University of North Texas, Denton, TX 76203-5070, [email protected] 1 Rare earths —introduction. The rare earths Figure 1. The “rare earths” are defined by IUPAC as the 15 lanthanides (green) and the upper two elements include the 17 chemically similar elements of the Group III family (yellow). These elements have similar chemical properties and all can exhibit the +3 occupying the f-block of the Periodic Table as oxidation state by the loss of the highest three electrons (two s electrons and either a d or an f electron, well as the Group III chemical family (Figure 1). depending upon the particular element). A few rare earths can exhibit other oxidation states as well; for These elements include the 15 lanthanides example, cerium can lose four electrons —4f15d 16s 2—to attain the Ce +4 oxidation state. (atomic numbers 57 through 71, lanthanum through lutetium), as well as scandium (atomic number 21) and yttrium (atomic number 39). The chemical similarity of the rare earths arises from a common ionic configuration of their valence electrons, as the filling f-orbitals are buried in an inner core and generally do not engage in bonding. The term “rare earths” is a misnome r—these elements are not rare (except for radioactive promethium). They were named as such because they were found in unusual minerals, and because they were difficult to separate from one another by ordinary chemical manipula - tions. -

Synthesis of Actinide Materials for the Study of Basic Actinide Science and Rapid Separation of Fission Products
UNLV Theses, Dissertations, Professional Papers, and Capstones 12-1-2017 Synthesis of Actinide Materials for the Study of Basic Actinide Science and Rapid Separation of Fission Products Jacquelyn M. Dorhout University of Nevada, Las Vegas Follow this and additional works at: https://digitalscholarship.unlv.edu/thesesdissertations Part of the Chemistry Commons Repository Citation Dorhout, Jacquelyn M., "Synthesis of Actinide Materials for the Study of Basic Actinide Science and Rapid Separation of Fission Products" (2017). UNLV Theses, Dissertations, Professional Papers, and Capstones. 3125. http://dx.doi.org/10.34917/11889685 This Dissertation is protected by copyright and/or related rights. It has been brought to you by Digital Scholarship@UNLV with permission from the rights-holder(s). You are free to use this Dissertation in any way that is permitted by the copyright and related rights legislation that applies to your use. For other uses you need to obtain permission from the rights-holder(s) directly, unless additional rights are indicated by a Creative Commons license in the record and/or on the work itself. This Dissertation has been accepted for inclusion in UNLV Theses, Dissertations, Professional Papers, and Capstones by an authorized administrator of Digital Scholarship@UNLV. For more information, please contact [email protected]. SYNTHESIS OF ACTINIDE MATERIALS FOR THE STUDY OF BASIC ACTINIDE SCIENCE AND RAPID SEPARATION OF FISSION PRODUCTS By Jacquelyn M. Dorhout Bachelor of Science – Chemistry University of Massachusetts Amherst 2012 A dissertation submitted in partial fulfillment of the requirements for the Doctor of Philosophy – Radiochemistry Department of Chemistry and Biochemistry College of Sciences The Graduate College University of Nevada, Las Vegas December 2017 Copyright by Jacquelyn M. -

Klaprothite Na6(UO2)(SO4)4(H2O)4
Klaprothite Na6(UO2)(SO4)4(H2O)4 Crystal Data: Monoclinic. Point Group: 2/m. As equant to blocky prismatic crystals, to ~ 1 mm, with skeletal or rounded edges and in parallel intergrowths. Crystals are elongated along [010] and display {100}, {001}, {110}, {011}, and {012}. Physical Properties: Cleavage: Perfect on {100} and {001}. Tenacity: Brittle, slightly sectile. Fracture: Irregular. Hardness = ~ 2.5 D(meas.) = 2.90(2) D(calc.) = 2.923 Bright bluish green fluorescence under SW & LW UV. Easily soluble in water; slightly deliquescent. Optical Properties: Transparent. Color: Yellowish green to greenish yellow. Streak: Pale yellow-green. Luster: Vitreous. Optical Class: Biaxial (–). α = 1.497 β = 1.517 γ = 1.519 2V(meas.) = 34(1)° 2V(calc.) = 34.7° Pleochroism: X = colorless, Y = light yellowish green, Z = light yellowish green. Absorption: X < Y ≈ Z. Orientation: Y = b, X ^ c = 10° in obtuse β. Dispersion: r > v, distinct. Cell Data: Space Group: P21/c. a = 9.8271(4) b = 9.7452(3) c = 20.8725(15) β = 98.743(7)° Z = 4 X-ray Powder Pattern: Blue Lizard mine, Red Canyon, San Juan County, Utah, USA. 3.434 (100), 7.09 (97), 5.158 (77), 9.72 (68), 3.082 (65), 3.012 (61), 4.330 (58) Chemistry: (1) (2) Na2O 21.06 21.51 UO3 33.14 33.10 SO3 35.93 37.05 H2O [8.15] 8.34 Total 98.28 100.00 (1) Blue Lizard mine, Red Canyon, San Juan County, Utah, USA; average of 11 electron microprobe analyses supplemented by Raman spectroscopy, H2O calculated from stoichiometry; corresponds to Na6.01(U1.03O2)(S0.99O4)4(H2O)4. -

Quantum Chemical Studies of Actinides and Lanthanides: from Small Molecules to Nanoclusters
Quantum Chemical Studies of Actinides and Lanthanides: From Small Molecules to Nanoclusters A DISSERTATION SUBMITTED TO THE FACULTY OF THE GRADUATE SCHOOL OF THE UNIVERSITY OF MINNESOTA BY Bess Vlaisavljevich IN PARTIAL FULFILLMENT OF THE REQUIREMENTS FOR THE DEGREE OF Doctor of Philosophy Professor Laura Gagliardi June, 2013 c Bess Vlaisavljevich 2013 ALL RIGHTS RESERVED Acknowledgements There are many people that I would like to thank for all of their support through my graduate school years. First of all, I'd like to thank my advisor Prof. Laura Gagliardi for her encouragement, advice, and providing me with countless opportunities to develop as a scientist. Additionally, I'd like to thank Prof. David Blank and Prof. Chris Cramer for taking the time to be great mentors in teaching. I would also like to thank Prof. Chris Cramer for all of the helpful discussions in research as well. I'd also like to thank the Chemistry faculty at the University of Minnesota { Twin Cities for all they have taught me. I'd also like to thank Profs. Joe Alia, Nancy Carpenter, Jenn Goodnough, Ted Pappenfus, and Jim Togeas at the University of Minnesota { Morris for starting me off on the right foot in my chemistry career. I would like thank all of the collaborators from outside the University of Minnesota for the very useful discussions especially Prof. Thomas Albrecht-Schmidt, Prof. Lester Andrews, Prof. Carles Bo, Prof. Peter Burns, Prof. Scott Daly, Prof. Paula Diaconescu, Prof. Greg Girolami, Dr. Ivan Infante, Dr. Jason Keith, Prof. Stephen Liddle, Prof. May Nyman, Dr. Jie Qiu, Dr. -

Organotitanium Chemistry (Merchant, 2017)
Baran Group Meeting Rohan Merchant Organotitanium Chemistry 08/04/2017 Ziegler Natta Catalysts First row transition metal Electron Configuration: [Ar]3d24s2 Common Oxidation States: +2, +3, +4 Highly oxophilic Highly resistant to corrosion Originally Ti-based catalysts used to prepare stereoregular polymers from propylene Highest strength-to-weight ratio of any metal One of the most important use of organotitanium complexes In unalloyed condition, titanium is as strong as Karl Ziegler and Giulio Natta awarded the Nobel Prize in chemistry in 1963 some steels Today, this class of catalysts has been expanded to include: 1. Solid supported Ti-based catalysts, often used in conjunction with organoaluminum cocatalysts (Kroll Process) 2. Metallocene catalysts, often of Ti, Zr, or Hf, and typically in conjuntion with MAO 250,000 tons per year of titanium made from TiCl4 3. Post-metallocene catalysts, various transition metals used with multidentate N and O based ligands, often use MAO Fun Facts about Titanium Worldwide production of polymers using these catalysts in 2010 >100 million tons British pastor William Gregor discovered titanium in 1791 This topic has not been covered in the interest of time. Named by German chemistry Martin Heinrich Klaproth after Titans of Greek mythology in 1795 See: "Polymer Chemistry" GM by D. Holte (2011) 9th most abundant element in the Earth's crust (0.63% of Earth's crust) 7th most abundant metal Common titanium complexes used in synthesis Pure sample isolated in 1910 by Matthew A. Hunter (Hunter Process) i -
Chemists for the Common Good (1)
Bull. Hist. Chem., VOLUME 42, Number 1 (2017) 1 CHEMISTS FOR THE COMMON GOOD (1) Ursula Klein, Max Planck Institute for the History of Science, Berlin, Germany; [email protected] Introduction that followed, his shop prospered both economically and scientifically. Klaproth produced and sold all kinds Martin Heinrich Klaporth (1743-1817) was the most of remedies as well as luxury goods and chemicals. The famous German chemist in the last third of the eighteenth eighteenth-century pharmaceutical laboratories belonged century. He was well known in Europe as an excellent to the precursors of the nineteenth-century chemical in- analytical chemist, discoverer and inventor. In 1789 he dustry. But Klaproth’s reputation as a chemist also grew discovered uranium (in the form of oxide) and what was apace. His private lectures on chemistry became the called “earth of zirconium,” that is, zirconium dioxide. latest fashion among Berlin’s intellectual elite. In 1782, In the years to follow he discovered or rediscovered six he received a teaching position at the Medical-Surgical additional substances: strontia (1793), earth of titanium College of Berlin (Collegium medico-chirurgicum), (titanium dioxide, 1795-97), tellurium (1798), chromium followed (in 1784) by a salaried teaching position at the (1798), beryllia (1801), and ceria (1804) (2). Throughout Mining Academy of Berlin and another teaching posi- his chemical career Klaproth analyzed, qualitatively and tion (in 1787) at the Artillery School of General G. F. v. quantitatively, more than 200 substances, most of mineral Tempelhoff (renamed Royal Artillery Academy in 1791), origin. In each single case “analysis” meant a true re- which earned him the title of professor (4). -

Demarcation Debates Lavoisier in Germany
Christoph Meinel Demarcation Debates Lavoisier in Germany During the 1860’s, German universities experienced the advent of a new genera- tion of »palace laboratories,« workshops designed for the mass production of chemical knowledge on a scale never before seen. These laboratories testified to the transformation of the universities into centres of experimental research, and impressively underlined Germany’s claim to leadership in the world of science., Berlin’s Chemical Laboratory, in particular, marked the culmination of represen- tation and functionality. Designed for August Wilhelm Hofmann upon his return from London, the huge building, close to the very centre of Prussian power, was one of the first of its kind to incorporate a rich sculptural programme dedicated to the history of science: a series of busts and portraits linking the lustre of tradition to chemistry’s claims to modernity.1 The distinguished personalities to be includ- ed in this gallery were chosen by a committee formed by the members of the physi- co-mathematical class of the Royal Prussian Academy of Sciences. On March 1st, 1866, the committee decided to decorate the entrance hall with life-sized busts of those unanimously held to be the most prominent living chemists of their time, namely Michael Faraday, Justus von Liebig and Friedrich Wöhler. More contro- versial was the choice of deceased chemists, whose portraits were to be placed in the 14 angles of the window arches alongside the front of the building. Eventually, and »not ... without a lengthy and animated discussion,«2 a list was drawn up, led by Antoine Laurent Lavoisier and followed by three of his rivals for the discovery of oxygen: Karl Wilhelm Scheele, Henry Cavendish, and Joseph Priestley. -

Romantic Chemistry Has Been Made Possible by the Generous Support of Our Sponsor, the Companhia Brasileira De Metalurgia E Mineração (CBMM)
chemistryRomantic Acknowledgements Romantic Chemistry has been made possible by the generous support of our sponsor, the Companhia Brasileira de Metalurgia e Mineração (CBMM). The Royal Society would also like to thank the following organisations and individuals for their help and advice in compiling the exhibition: Beta Technology Ltd., including Ben Micó and Jayne Evans. The Department of Earth Sciences at the Natural History Museum, London. Derby Museum and Art Gallery, Derby. introduction The exhibition Romantic Chemistry uses the Royal You could say that the Romantic Chemists had it easy. Society’s archives to tell the stories of the early Most of the elements were waiting to be discovered. scientists Humphry Davy, Smithson Tennant, William But now, synthesising new super-heavy elements Hyde Wollaston and many others, the elements they is the realm of specialised physics centres. So what uncovered, and the modern world they built. Many is the chemistry that will really excite the public treasures are exhibited, including Joseph Priestley’s today? I believe that one area is green chemistry, the spectacles, with frames of a surprisingly trendy design, cleaner, safer production of chemicals and materials. the prototype of Davy’s miner’s lamp and, more Sustainability is becoming increasingly important in prosaically, my old Osmiroid fountain pen, displayed people’s minds. They want to live in a greener way but because of the osmium/iridium alloy in its nib. are reluctant to change their lifestyles. Furthermore, 1.3 billion of our planet’s poorest inhabitants need to Are there messages for us today in this fascinating consume more to lift them from profound poverty. -

THE MAJOR RARE-EARTH-ELEMENT DEPOSITS of AUSTRALIA: GEOLOGICAL SETTING, EXPLORATION, and RESOURCES Figure 1.1
CHAPTER ONE WHAT ARE RARE- EARTH ELEMENTS? 1.1. INTRODUCTION latter two elements are classified as REE because of their similar physical and chemical properties to the The rare-earth elements (REE) are a group of seventeen lanthanides, and they are commonly associated with speciality metals that form the largest chemically these elements in many ore deposits. Chemically, coherent group in the Periodic Table of the Elements1 yttrium resembles the lanthanide metals more closely (Haxel et al., 2005). The lanthanide series of inner- than its neighbor in the periodic table, scandium, and transition metals with atomic numbers ranging from if its physical properties were plotted against atomic 57 to 71 is located on the second bottom row of the number then it would have an apparent number periodic table (Fig. 1.1). The lanthanide series of of 64.5 to 67.5, placing it between the lanthanides elements are often displayed in an expanded field at gadolinium and erbium. Some investigators who want the base of the table directly above the actinide series to emphasise the lanthanide connection of the REE of elements. In order of increasing atomic number the group, use the prefix ‘lanthanide’ (e.g., lanthanide REE: REE are: lanthanum (La), cerium (Ce), praseodymium see Chapter 2). In some classifications, the second element of the actinide series, thorium (Th: Mernagh (Pr), neodymium (Nd), promethium (Pm), samarium 1 (Sm), europium (Eu), gadolinium (Gd), terbium (Tb), and Miezitis, 2008), is also included in the REE dysprosium (Dy), holmium (Ho), erbium (Er), thulium group, while promethium (Pm), which is a radioactive (Tm), ytterbium (Yb), and lutetium (Lu).