Beauty Salon, Barber Shop and Spa
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Opening a Salon Checklist
OPENING FROM A SALON CHECKLIST STEP 1: PLAN & ESTABLISH BUSINESS Select a name & business legal structure Develop your business plan, financial projections & budget Develop business branding, logo & identity Obtain your cosmetology license (if applicable) Obtain a federal employer ID number Obtain a state tax ID Open a company bank account Choose a website domain name & register it Research local zoning to locate areas with proper zoning for salons Choose a location for your salon & sign a lease/purchase space STEP 2a: OPERATIONAL SETUP Research inspection requirements, local codes & regulations for your area Research, interview & hire plumbers, electricians & handymen Create salon layout & design plan Map out electrical & plumbing Apply for business licenses & building permits STEP 2b: OPERATIONAL SETUP Arrange any needed financing Obtain business insurance coverage Contact utility providers (power, security, water, waste, etc.) Choose a phone & internet provider Choose suppliers for wet goods & consumables Choose a credit card processing company Purchase point of sale equipment Purchase computers & appointment-booking software Purchase & set up accounting & record-keeping software Purchase business cards Purchase outdoor & indoor signage STEP 3: PURCHASING YOUR EQUIPMENT Note: Start purchasing these items 8 - 12 weeks before your grand opening day. You'll want to give yourself plenty of time to get shampoo bowls plumbed in, electrical finalized, etc. STYLING CHAIRS DRYERS/STEAMERS/HAIR PROCESSORS Salon Styling Chair Dryer Unit: Hooded -

Wigmaker and Barber by Sharon Fabian
Name Date Wigmaker and Barber By Sharon Fabian Cosmetology is a popular vocational subject in high school. In cosmetology class, students learn to wash and cut hair. They learn to give perms and to color hair too. They learn how to do a fancy hairstyle for a special occasion like a prom. They might learn to cut and style wigs as well as real hair. Cosmetology students often go on to work as hairdressers, styling hair for customers. In colonial times, there were also people who worked as hairdressers. Some people are surprised to learn that, because we often think of the colonists as hard working people who didn't have time for frivolous things like a fancy hairdo. However, there were many people in colonial America who were very fashion conscious and who kept up with the latest styles in both clothing and hairstyles. This was especially true in the larger cities like Williamsburg, Virginia. A city like Williamsburg had shops that catered to the fashion conscious. Wigmakers and barbers there both provided hairdressing services. A barber might provide shaves and haircuts in addition to his other duties, such as performing surgery and pulling teeth! A wigmaker, of course, made wigs, and in the 1700s, wigs were the latest fashion! The fashion of wearing wigs began with the royalty in France; it spread to England and then to America. In colonial times, the gentlemen, not the ladies, wore wigs. Colonial gentlemen also wore queues. A queue was like a ponytail wig that was tied on at the back of the head. -

Barbershop Quartet Sc They Wear Even Politicians and Bureaucrats Are Serious About Their Hair: Nearly a Dozen It Well Federal Entities Have On-Site Barbers
Great HAIR OM SC EW N THEY WEAR EvenBarbershop politicians and bureaucrats are serious aboutQuartet their hair: Nearly a dozen IT WELL RIPPLAAR/SIPA/ federal entities have on-site barbers. Here’s a look at four. T Sure, Abraham Lincoln and Teddy Roosevelt By Kate Parham TOFFER sported distinguished facial hair, but modern S RI K Washington men seem more comfortable with a Y B close shave—though there are exceptions. OLDER We asked Mike Gilman, cofounder of the House of Central H OM; Grooming Lounge, and Aaron Perlut, chairman of ➻ Representatives ➻ Intelligence SC EW the American Mustache Institute, to tell us who Agency N around town has winning facial hair. Barber: Joe Quattrone, formerly LLAN/ U a farmer in Italy, heads the House’s M Barber: Daivon Davis is not only c By Christine Ianzito M privatized barbershop. His is one of K the first African-American to own C the best jobs, he says, “because you the CIA’s barbershop but the first to ATRI P come in contact every day with the cut hair in the shop, which opened people who control the world.” LDING/ Ted Leonsis Jayson Werth in 1955. Now 24, he got the gig at age U 18, then bought the shop in 2010. ENTREPRENEUR NATIONALS OUTFIELDER Inside look: He has trimmed ev- Y CLINT SPA eryone from Prime Minister Giulio Inside look: Davis’s chair has seen B ER Andreotti of Italy—who insisted on the likes of General Michael Hayden Z having his picture taken with Quat- and former CIA director Leon I; BLIT ZZ trone—to Dick Cheney, Al Gore, and I Panetta. -
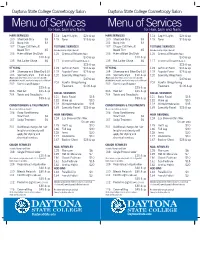
Menu of Services
Daytona State College Cosmetology Salon Daytona State College Cosmetology Salon Menu of Services Menu of Services for Hair, Skin and Nails for Hair, Skin and Nails HAIR SERVICES 114 Cap Hi-Lights $25 & up HAIR SERVICES 114 Cap Hi-Lights $25 & up 100 Shampoo Only $3 115 Toner $15 & up 100 Shampoo Only $3 115 Toner $15 & up 101 Bang Trim $3 _______________________________ 101 Bang Trim $3 _______________________________ 102 Clipper Cut/Haircut/ TEXTURE SERVICES 102 Clipper Cut/Haircut/ TEXTURE SERVICES Beard Trim $5 (Includes Shampoo/Style & Haircut) Beard Trim $5 (Includes Shampoo/Style & Haircut) 103 Haircut/Blow-Dry/Style 116 Chemical Relaxer (Virgin) 103 Haircut/Blow-Dry/Style 116 Chemical Relaxer (Virgin) $10 & up $30 & up $10 & up $30 & up 135 Hot Lather Shave $6 117 Chemical Relaxer (Retouch) 135 Hot Lather Shave $6 117 Chemical Relaxer (Retouch) _______________________________ $25 & up _______________________________ $25 & up STYLING 118 Soft Curl Perm $35 & up STYLING 118 Soft Curl Perm $35 & up 104 Shampoo and Blow-Dry $10 119 Regular Perm $25 & up 104 Shampoo and Blow-Dry $10 119 Regular Perm $25 & up 105 Specialty Style $10 & up 120 Specialty Wrap Perm 105 Specialty Style $10 & up 120 Specialty Wrap Perm (May include; wrap, twists, press & curl, wet sets with (May include; wrap, twists, press & curl, wet sets with $40 & up $40 & up detailed finish, up-do’s, spiral curls, freeze curls or flat-iron) detailed finish, up-do’s, spiral curls, freeze curls or flat-iron) 203 Keratin Straightening 203 Keratin Straightening 202 Dominican -

Barber Shops Full Page
July/Aug 2012 Edition The Fayetteville Press Page 5b Community Barber Shops Flat Top Haircut Barbershop 360 Waves Brushing Techniques It is easy to achieve a flattop haircut, barbershop style As a guy who wants a perfect waved up hairstyle right from home. People are generally more familiar with you may want to consider 360 waves brushing tech- the flattops cousin hairstyle, the crew cut. The flattop is niques. To get those waves to spinning there is a certain similar to the crew cut in many ways, the difference is that way you need to handle your brush when stroking your with a flattop hairstyle the hair on the tops of the head is thirsty roots. A grooming plan that involves a strategic made to stand up, and is then cut in a flat style. This is what regiment of brushing is imperative to get your hair fol- gives this hairstyle is square shape. licles spinning. Some guys figure it out on there own but You would commonly find this hairstyle on boys. Girls others prefer a training guide. do sometimes wear this hairstyle or different variations or Are there tricks and trade secrets to getting these it, but this is uncommon. The flattop is a popular military style haircut because it is similar to the military crew cut. deep waves? Well yes and no. To get the effective and People commonly created this hairstyle with electric desired results you seek follow the instructions below clippers, which cut the sides and back of the hair. Using the provided by Wave Builder which includes their mainte- clippers, a stylist will cut the hair very close to the scalp; it nance preferences. -

WHO Surgical Site Infection Prevention Guidelines Web Appendix 7 Summary of a Systematic Review on the Effectiveness and Optimal Method of Hair Removal
WHO Surgical Site infection Prevention Guidelines Web Appendix 7 Summary of a systematic review on the effectiveness and optimal method of hair removal 1. Introduction Removal of hair from the intended site of surgical incision has traditionally been part of the routine preoperative preparation of patients undergoing surgery. Hair removal may be necessary to facilitate adequate exposure to the site and preoperative skin marking. Furthermore, suturing and the application of wound dressings can be complicated by the presence of hair. Apart from these practical issues, hair has been associated with a lack of cleanliness and the potential to cause surgical site infection (SSI). However, there is also the belief that hair removal inversely increases the risk of SSI by causing microscopic trauma of the skin. To minimize the potential of skin trauma, the use of clippers instead of razors has been proposed for preoperative hair removal. Clippers cut the hair close to the skin without actually touching it, whereas razors involve a sharp blade drawn directly over the skin. A third method for hair removal is the application of depilatory creams containing chemicals. The drawbacks are the necessity to leave the cream in place for approximately 15-20 minutes for the hair to be dissolved and the potential for allergic reactions. A Cochrane review, published in 2009 and updated in 2011, concluded that there was no statistically significant effect on SSI rates of hair removal 1. However, a significant harm was seen when hair removal with razors was compared with clipping. 2. PICO questions 1. Does hair removal affect the incidence of SSI? 2. -

Beauty Salon and Barber Shop Product Claim Examples
Beauty Salon and Barber Shop Product Claim Examples u General Liability u Property A patron at a nail salon was receiving a manicure. As she The nail salon’s pipe broke from the pedicure chair, causing stood up, she fainted from the fumes causing fractures to damage to the insured’s property. The cost to replace the her face. Medical costs were $150,000 after reconstructive damaged items was $5,000. facial surgery. A stylist did not unplug his hair dryer when he left the salon. A hair stylist was providing hair cutting services to her The dryer short-circuited and caused $20,000 in damages to customer. As it was very busy that day, the stylist was the salon. not able to sweep up the hair before accepting the next customer. The next customer slipped and broke his wrist when he tried to catch himself. Because he was a computer programmer, he was not able to perform his duties. Medical and lost wage costs totaled $50,000. u Professional Liability A patron came in to receive a pedicure. Unknown to the nail technician, the patron had a skin disease. The pedicure procedure aggravated the skin, which caused an infection resulting in $25,000 in medical costs for the patron. The hair stylist used her normal hair dying solution on a new customer. The customer had a severe allergic reaction to the chemicals and was hospitalized for two days. The medical and loss wage costs were $20,000. Policyholders have access to many services through our Business Resource Center that will assist in growing and protecting their business. -

THE COMPLETE SALON EQUIPMENT GUIDE PAGE 3 General Salon Equipment
The Complete WWW.JOINBLVD.COM Salon Equipment Everything You Need to Guide Outfit Your Salon Contents Introduction 03 Ring light for salon photos 12 General Salon Equipment 04 Cleaning products 12 Checklist and price ranges 13 Reception area equipment 04 Retail display shelving 05 Nail salons 14 Commercial laundering equipment 05 Manicure stations 14 Outdoor signage 06 Pedicure chairs 14 Checklist and price ranges 06 Nail drying station 14 Hair salons 07 Nail polish racks 15 Manicure/pedicure supplies 15 Aprons and cutting capes 07 Checklist and price ranges 15 Towels 07 Hand mirrors 08 Protecting stylists during COVID-19 16 Spray bottles 08 Georgia Board of Cosmetology 17 Hair clips 08 practices 09 Combs and brushes Personal protective equipment for salons 18 Salon scissors 09 Hairdryers 09 Hand protection 18 Hair straighteners 10 Eye protection 18 Curling irons 10 Respiratory Protection 18 Hair clippers 10 Checklist and price ranges 18 Salon chairs 11 Conclusion 19 Salon carts & trolleys 11 Shampoo station (backwash) 11 About Boulevard 19 Hairstyling stations 12 Introduction Salon owners know there’s more to starting a how do you run a professional hair salon without business than professional cosmetology licensure. shampoo bowls and salon chairs? Whether you’re starting a salon from the studs up or scaling your You must buy or rent a location, locate comfortable existing operations, these are the crucial details that furniture, and order enough salon equipment you need to get right. to support clients and stylists. Without these considerations, your salon is little more than a few In our salon equipment guide, we’ve summarized empty rooms. -

Catalog Volume 39
AMERICAN INSTITUTE OF BEAUTY, INC. LARGO CAMPUS 3665 East Bay Drive Suite 164 Largo Florida 33771 727-532-2125 ST. PETERSBURG CAMPUS 2800 34th St. North St. Petersburg, Florida 33713 727-826-0969 SCHOOL CATALOG ACCREDITED BY ! Volume 39 July 2017 TABLE OF CONTENTS Page 3 Ownership and History Page 3 Mission Statement Page 3 Administrative Staff Page 3 – 4 Faculty Page 4 Hours of Operation Page 4 Professional Ethics and Duties Page 4 – 5 Facilities Page 5 Campus Security Page 5 Student Commitment and Consumer Rights Page 5 – 6 Student Responsibilities and Rights Page 6 What You Should Know Page 6 – 7 Job Demand in Cosmetology Page 7 Placement Assistance Page 7 Admissions Requirements Page 7 – 8 Transfer of Credits Page 8 Ability to Benefit Page 8 Advising Page 8 Attendance Page 8 – 9 Veterans’ Educational Benefits Page 9 Dress Code Page 9 Tardiness Page 9 – 10 Make Up Work Page 10 Graduation Requirements Page 10 Program or Schedule Change Page 10 Re-entry Students Page 10– 11 Leave of Absence Page 11 School Policy on the Handicapped Page 11 School Policy on Student Services Page 11 – 12 Privacy and Access to Student Records Page 12 – 13 Standards of Conduct Page 13 – 14 Disciplinary Policies Page 14 Student Services Page 14 – 15 Instructional Methods Page 15 Units of Instruction and Hours Page 15 Programs Offered Page 15 – 17 Cosmetology Program Page 17 – 18 Restricted Barber Program Page 18 – 19 Barbering/Hair Design Program Page 19 – 21 Nail Technology Program Page 21 – 23 Skin Care Program Page 23 – 25 Clinical Skin Care Program Page 25 – 27 Full Specialist Program Page 28 Course numbering system Page 28 Unit of credit Page 28 Tuition and Fees Page 28 Additional Tuition Page 28 – 29 Financial Assistance Page 29 School Calendar Page 29 – 30 Licensure Requirements Page 30 Grievance Policy Page 30 – 33 Satisfactory Academic Progress Policy Page 33 – 35 Refund and Cancellation Policy !2 Page 35 – 36 Organization and Affiliations OWNERSHIP AND HISTORY American Institute of Beauty, Inc. -

Crowded House Skin Clinic, Hair & Beauty Salon
CROWDED HOUSE SKIN CLINIC, HAIR & BEAUTY SALON 626 Manchester Road Bury BL9 9SU 0161 280 5905 BOOK ONLINE AT www.crowdedhousebury.co.uk CROWDED HOUSE SKIN CLINIC, HAIR & BEAUTY SALON Hair Hair Cutting & Styling Hair Consultation 10mins £0 Ladies Wash, Cut & Blow 1h £35 Ladies Restyle, Cut & Blow Dry 1h £39 Wash & Blow Dry/Straighten/Wanded/Pin Curl/ 1h £22 Curly Blow/Put Up/Party Curls Unwashed Straightened/Wanded/Pin Curl/Curly Blow/ 40mins £19 Put Up/Party Curls Perm With Cut & Blow Dry (OAP’s) 1h 30mins £45 Braids & Plaites (not washed) 20mins £10 Fringe Trim 5mins £5 Gents Dry Cut 45mins £10 Gents Wash, Head Massage, Cut & Style 30mins £15 Gents Wash, Head Massage, Cut & Restyle 30mins £22 Child Hair Cut (Under 10yrs) 30mins £10 Child Under 10 Wash Cut & Finish 30mins £15 Innoluxe re bonding conditioner that reinforces 20mins £25 your hairs strength Luxury Head Massage 5mins £5 Tape Extensions (with your own Extensions, includes fitting & cut) 1h 15mins £80 Tape Extensions (Extensions supplied, includes fitting & cut) 1h 15mins £300 2 CROWDED HOUSE SKIN CLINIC, HAIR & BEAUTY SALON Fashion Colours (Semi Permanent, note: patch test required 24 hours prior to treatment) 1 Fashion Colour & Blow Wave for Long Hair 1h 30mins £35 (Add £10 for each addtional colour) 1 Fashion Colour & Blow Wave for Medium Hair 1h 25mins £30 (Add £7 for each addtional colour) 1 Fashion Colour & Blow Wave for Short Hair 1h £25 (Add £5 for each addtional colour) Highlights (note: patch test required 24 hours prior to treatment) (If Cut & Blow Required Pls Book Additional Required Service. -

Barber Makes Shaving Easy the Perforated Hone
mple Invention of Western Barber Makes Shaving Easy V m New Perforated Razor Hone, Which Prevents Wire Edge, Already Has Thousands of Satisfied Users you all what a good shave was until I tried bevel on a chisel, but much thinner. tinual expense, and? will last some sub- your life. my brother's Perforated Hone. I This can only be done by wouldn't be without one now, and en- stance harder than steel, such as the EVEN" BARBERS I SB THE PERFOR- used close $3 for three." fine but very hard cutting stone ATED HONE. 11. Wallace Noyes, Portland Maine, In the Perforated Hone. If there is any one class of men that old-sty- wrote: "Received the Perforated Hone, The cutting edge of u razor is so very could get along with the le hone, proper con- and It works O. K. Send me four more thin and delicate that even the finest, and keep their razors In at once; want them for Christmas Va hardest steel gets hent and twisted dition with It, surely It woulc be the .presents. Enclosed are $4.00.' experi- out of shape by the thousands of barbers. But they know from And so we could go on. but they all stubby, wiry bristles on the average ence the. supreme importance of a good ir very-bes- say same thing In a little about the man's face. Then a few s'rokea on hone, and they always use the different way. the strop will staighten or "true" this they can buy. even If it costs them bent edge But after several such strop-plng- s 125.00. -

Guide to Opening a Barbershop, Hair Salon And/Or Cosmetology Shop
Chesprocott Health District Guide to Opening a Barbershop, Hair Salon and/or Cosmetology Shop Chesprocott Health District requires that all plans for proposed hairdressing and/or cosmetology salon or shop must be submitted to this office for review. This helps ensure that the proposed equipment, layout and floor/wall finishes meet the local ordinance requirements before the start of construction. Following the plan review and the completion of construction, our Registered Sanitarian will conduct a preopening inspection of your facility. A Cosmetology Permit will be presented upon completion of all requirements and is required to operate a salon in our district. We hope that you find the enclosed material helpful in your planning. Please do not hesitate to contact this office should you have any questions regarding the planning of your facility. 1 PROPOSED COSMETOLOGY SHOP/SALON REQUIREMENTS The following information must be submitted to Chesprocott Health District for all proposed barbershop, hairdressing and/or cosmetology salon/shops: □ 1. A plan review application which is included in this packet and the required fee (see current fee schedule). □ 2. A complete floor plan including equipment layout and work flow. □ 3. Cut sheets of all types and models of equipment to be used. □ 4. List of material that floors, walls and ceilings will consist of □ 5. If the facility is served by an onsite well, you must be registered with the Connecticut Department of Public Health Water Supply Section (DPH) and a lab analysis verifying the water portability must be submitted to the Health District. Check with staff if you need assistance.