Final Addenda FY 2005
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Anterior Reconstruction Techniques for Cervical Spine Deformity
Neurospine 2020;17(3):534-542. Neurospine https://doi.org/10.14245/ns.2040380.190 pISSN 2586-6583 eISSN 2586-6591 Review Article Anterior Reconstruction Techniques Corresponding Author for Cervical Spine Deformity Samuel K. Cho 1,2 1 1 1 https://orcid.org/0000-0001-7511-2486 Murray Echt , Christopher Mikhail , Steven J. Girdler , Samuel K. Cho 1Department of Orthopedics, Icahn School of Medicine at Mount Sinai, New York, NY, USA Department of Orthopaedics, Icahn 2 Department of Neurological Surgery, Montefiore Medical Center/Albert Einstein College of Medicine, Bronx, School of Medicine at Mount Sinai, 425 NY, USA West 59th Street, 5th Floor, New York, NY, USA E-mail: [email protected] Cervical spine deformity is an uncommon yet severely debilitating condition marked by its heterogeneity. Anterior reconstruction techniques represent a familiar approach with a range Received: June 24, 2020 of invasiveness and correction potential—including global or focal realignment in the sagit- Revised: August 5, 2020 tal and coronal planes. Meticulous preoperative planning is required to improve or prevent Accepted: August 17, 2020 neurologic deterioration and obtain satisfactory global spinal harmony. The ability to per- form anterior only reconstruction requires mobility of the opposite column to achieve cor- rection, unless a combined approach is planned. Anterior cervical discectomy and fusion has limited focal correction, but when applied over multiple levels there is a cumulative ef- fect with a correction of approximately 6° per level. Partial or complete corpectomy has the ability to correct sagittal deformity as well as decompress the spinal canal when there is an- terior compression behind the vertebral body. -

Spinal Interventional Pain Management and Lumbar Spine Surgery
Spinal Interventional Pain Management and Lumbar Spine Surgery Policy Number: Original Effective Date: MM.06.024 01/01/2014 Line(s) of Business: Current Effective Date: HMO; PPO; QUEST Integration 12/15/2017 Section: Surgery; Medicine Place(s) of Service: Office; Outpatient; Inpatient I. Description The following spinal interventional pain management and lumbar spine surgery procedures require precertification through Magellan Hawaii, formally known as National Imaging Associates, Inc. (NIA): A. Spinal Epidural Injections B. Paravertebral Facet Joint Denervation (radiofrequency neurolysis) C. Paravertebral Facet Joint Injections or Blocks D. Sacroiliac joint injections E. Lumbar Spinal Fusion Surgery II. Administrative Guidelines A. The ordering physician can obtain precertification or consult with Magellan Hawaii by accessing their website at http://www.radmd.com/ or by calling 1 (866) 306-9729, from 6 a.m. to 6 p.m., weekdays, Hawaii Time. Refer to the e-library for instructions on navigating the radmd.com website (RadMD Get Started) and requesting precertification/checking the status of a request (RadMD QuickStart). B. For access to the latest clinical guidelines used for precertification, go to www.radmd.com and click on the link entitled View Clinical Guidelines. C. For interventional pain management procedures (epidural injections, facet joint denervation neurolysis, facet joint injections and sacroiliac joint injections), if more than one procedure is planned, a separate precertification number must be obtained for each procedure planned. D. For spinal surgeries (lumbar fusions, lumbar decompressions, and lumbar microdiscectomy), one precertification number should be obtained for the most invasive surgery to be performed. E. Precertification requirements for injection procedures apply only to office and outpatient services (POS 11, 22, or 24). -

Automated Percutaneous and Endoscopic Discectomy
Corporate Medical Policy Automated Percutaneous and Endoscopic Discectomy File Name: percutaneous_discectomy Origination: 9/1991 Last CAP Review: 5/2021 Next CAP Review: 5/2022 Last Review: 5/2021 Description of Procedure or Service Surgical management of herniated intervertebral discs most commonly involves discectomy or microdiscectomy, performed manually through an open incision. Automated percutaneous discectomy involves placement of a probe within the intervertebral disc under image guidance with aspiration of disc material using a suction cutting device. Removal of disc herniations under endoscopic visualization is also being investigated. Endoscopic discectomy involves the percutaneous placement of a working channel under image guidance, followed by visualization of the working space and instruments through an endoscope, and aspiration of disc material. Back pain or radiculopathy related to herniated discs is an extremely common condition and a frequent cause of chronic disability. Although many cases of acute low back pain and radiculopathy will resolve with conservative care, a surgical decompression is often considered when the pain is unimproved after several months and is clearly neuropathic in origin, resulting from irritation of the nerve roots. Open surgical treatment typically consists of discectomy, in which the extruding disc material is excised. When performed with an operating microscope the procedure is known as microdiscectomy. Minimally invasive options have also been researched, in which some portion of the disc is removed or ablated, although these techniques are not precisely targeted at the offending extruding disc material. Ablative techniques include laser discectomy and radiofrequency (RF) decompression. In addition, intradiscal electrothermal annuloplasty is another minimally invasive approach to low back pain. -

Musculoskeletal Program CPT Codes and Descriptions
Musculoskeletal Program CPT Codes and Descriptions Spine Surgery Procedure Codes CPT CODES DESCRIPTION Allograft, morselized, or placement of osteopromotive material, for spine surgery only (List separately in addition 20930 to code for primary procedure) 20931 Allograft, structural, for spine surgery only (List separately in addition to code for primary procedure) Autograft for spine surgery only (includes harvesting the graft); local (eg, ribs, spinous process, or laminar 20936 fragments) obtained from same incision (List separately in addition to code for primary procedure) Autograft for spine surgery only (includes harvesting the graft); morselized (through separate skin or fascial 20937 incision) (List separately in addition to code for primary procedure) Autograft for spine surgery only (includes harvesting the graft); structural, bicortical or tricortical (through separate 20938 skin or fascial incision) (List separately in addition to code for primary procedure) 20974 Electrical stimulation to aid bone healing; noninvasive (nonoperative) Osteotomy of spine, posterior or posterolateral approach, 3 columns, 1 vertebral segment (eg, pedicle/vertebral 22206 body subtraction); thoracic Osteotomy of spine, posterior or posterolateral approach, 3 columns, 1 vertebral segment (eg, pedicle/vertebral 22207 body subtraction); lumbar Osteotomy of spine, posterior or posterolateral approach, 3 columns, 1 vertebral segment (eg, pedicle/vertebral 22208 body subtraction); each additional vertebral segment (List separately in addition to code for -

Successful Aortocoronary Bypass in Osteogenesis Imperfecta
View metadata, citation and similar papers at core.ac.uk brought to you by CORE 960 provided bylACC Elsevier Vol. - Publisher 9. No.4 Connector April 1987:960-3 CASE REPORTS Successful Aortocoronary Bypass in Osteogenesis Imperfecta JOHN MURRAH PASSMORE, MD, WILLIAM EASTON WALKER, MD, PHD , FRANCISCO FUENTES, MD, FACC Houston, Texas Cardiovascular abnormalities are infrequently docu anastomoses. Although successfulaortocoronary bypass mented in osteogenesis imperfecta, one of a group of surgery had not been previouslyreported in osteogenesis hereditary, generalized connective tissue disorders. A imperfecta, this patient received such surgery with ther patient with osteogenesis imperfecta is described with apeutic benefit. Therefore, coronary artery vascularl mitral valve prolapse, significantcoronary artery disease zation should be considered as a safe and effective treat and a coronary artery aneurysm. The latter two cardiac ment modality for patients with osteogenesis imperfecta defects are apparently rare in this disease. The option and coexistingcoronary atherosclerosis. of surgery was carefully considered with regard to tech (J Am Coll CardioI1987,'9:960-3) nical feasibility and potential deterioration of the graft Osteogenesis imperfecta is one of the group of hereditary , disorders, including pseudoxanthoma elasticum (4) and Eh generalized disorders of connective tissue including Mar lers-Danlos syndrome (5). fan's syndrome, pseudoxanthoma elasticum, Ehlers-Danlos We present a patient with osteogenesis imperfecta who syndrome and Hurler's syndrome. Significant cardiovas had significant multivessel disease that was treated with cular abnormalities are a recognized feature of the latter four coronary artery bypass grafting. The results indicate that conditions (I ). Although the primary clinical manifestations such surgery is worthy of consideration and feasible in pa of osteogenesis imperfecta include skeletal, ocular, cuta tients with this connective tissue disorder. -

Biomechanical Evaluation of Relationship of Screw Pullout
ORIGINAL ARTICLE Biomechanical Evaluation of Relationship of Screw Pullout Strength, Insertional Torque, and Bone Mineral Density in the Cervical Spine Charles Alan Reitman, MD, Lyndon Nguyen, and Guy R. Fogel help prevent implant loosening and add rigidity to the plate- Background: Understanding of implant failure mechanisms is im- screw construct. Some screws actually lock to the plate, while portant in the successful utilization of anterior cervical plates. Many in most cases, there is some kind of blocking plate or screw variables influence screw purchase, including the quality of the bone. head expansion to secure the screw to the plate. In these cases, The purpose of this study was to assess the relationship of screw pull- out and screw insertional torque across a wide range of bone mineral the screws are initially placed securely per the surgeon’s own densities (BMDs). perception, in most instances without specific torque control. Screw pullout and stripping (exceeding maximal inser- Methods: A total of 54 cervical vertebrae in 12 cervical spines were tional torque) are possible modes of failure. Some factors af- evaluated for BMD using dual-energy x-ray absorptiometry scan- fecting the pullout strength of a cancellous bone screw are spe- ning. Actual and perceived peak torques of 3.5-mm anterior cervical cific to the screw design and include the major diameter of the screws were determined at each level followed by screw pullout screw, the length of engagement of the thread, and screw strength testing. thread depth and pitch.4 Furthermore, tapping was found to Results: A high correlation was observed between screw pullout reduce pullout force by an average of 8% compared with non- strength and BMD. -

Computer-Aided Patient-Specific Coronary Artery Graft Design
Cardiovascular Engineering and Technology, Vol. 2, No. 1, March 2011 (Ó 2010) pp. 35–47 DOI: 10.1007/s13239-010-0029-z Computer-Aided Patient-Specific Coronary Artery Graft Design Improvements Using CFD Coupled Shape Optimizer 1 2 3 4 ONUR DUR, SINAN TOLGA COSKUN, KASIM OGUZ COSKUN, DAVID FRAKES, 5 1,5 LEVENT BURAK KARA, and KEREM PEKKAN 1Department of Biomedical Engineering, Carnegie Mellon University, Pittsburgh, PA, USA; 2Department of Vascular Surgery, Horst Schmidt Kliniken, Wiesbaden, Germany; 3Department of Thoracic Cardiovascular Surgery, University of Go¨ttingen, Go¨ttingen, Germany; 4School of Biological and Health Systems Engineering, Arizona State University, Tempe, AZ, USA; and 5Department of Mechanical Engineering, Carnegie Mellon University, Pittsburgh, PA, USA (Received 29 June 2010; accepted 1 November 2010; published online 18 November 2010) Associate Editor Peter McHugh oversaw the review of this article. Abstract—This study aims to (i) demonstrate the efficacy of a coronary bypass surgery procedures based on acute hemo- new surgical planning framework for complex cardiovascular dynamic readjustments of aorta-CA flow. This methodology reconstructions, (ii) develop a computational fluid dynamics may provide a rational to aid surgical decision making in (CFD) coupled multi-dimensional shape optimization meth- time-critical, patient-specific CA bypass operations before in od to aid patient-specific coronary artery by-pass graft vivo execution. (CABG) design and, (iii) compare the hemodynamic effi- ciency of the sequential CABG, i.e., raising a daughter Keywords—Surgical planning, Coronary artery, Bypass parallel branch from the parent CABG in patient-specific 3D graft, CFD, Hemodynamics, Shape optimization, Sequential settings. Hemodynamic efficiency of patient-specific complete revascularization scenarios for right coronary artery (RCA), graft, WSS, WSSG, Surgical design. -
IVUS Imaging Catheters Reference Guide
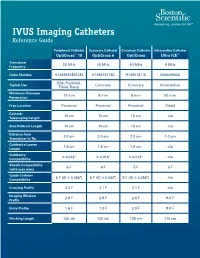
IVUS Imaging Catheters Reference Guide Peripheral Catheter Coronary Catheter Coronary Catheter Intracardiac Catheter OptiCross™ 18 OptiCross 6 OptiCross Ultra ICE™ Transducer 30 MHz 40 MHz 40 MHz 9 MHz Frequency Order Number H7493932800180 H7495181160 H749518110 M00499000 SFA, Popliteal, Typical Use Coronary Coronary Intracardiac Tibial, Renal Maximum Diameter 12 mm 6 mm 6 mm 50 mm Penetration Prep Location Proximal Proximal Proximal Distal Catheter 15 cm 15 cm 15 cm n/a Telescoping Length Sled Pullback Length 10 cm 10 cm 10 cm n/a Distance from 2.0 cm 2.0 cm 2.0 cm 1.0 cm Transducer to Tip Guidewire Lumen 1.6 cm 1.6 cm 1.6 cm n/a Length Guidewire ≤ 0.018" ≤ 0.014" ≤ 0.014" n/a Compatibility Sheath Compatibility 6 F 6 F 5 F 9 F (with max wire) Guide Catheter 6 F (ID ≥ 0.068") 6 F (ID ≥ 0.064") 5 F (ID ≥ 0.058") n/a Compatibility Crossing Profile 3.5 F 3.1 F 3.1 F n/a Imaging Window 2.9 F 2.9 F 2.6 F 9.0 F Profile Entry Profile 1.6 F 1.3 F 2.0 F 9.0 F Working Length 135 cm 135 cm 135 cm 110 cm OPTICROSS™ 18 CATHETER AND MDU5 PLUS BAG OPTICROSS 6 40 MHZ CORONARY IMAGING CATHETER CAUTION Federal law (USA) restricts this device to sale by or on the order of a physician. Rx only. Prior to use, please see the CAUTION: Federal law (USA) restricts this device to sale by or on the order of a physician. -

The Costs and Benefits of Moving to the ICD-10 Code Sets
CHILDREN AND ADOLESCENTS This PDF document was made available from www.rand.org as a public CIVIL JUSTICE service of the RAND Corporation. EDUCATION ENERGY AND ENVIRONMENT Jump down to document HEALTH AND HEALTH CARE 6 INTERNATIONAL AFFAIRS POPULATION AND AGING The RAND Corporation is a nonprofit research PUBLIC SAFETY SCIENCE AND TECHNOLOGY organization providing objective analysis and effective SUBSTANCE ABUSE solutions that address the challenges facing the public TERRORISM AND HOMELAND SECURITY and private sectors around the world. TRANSPORTATION AND INFRASTRUCTURE U.S. NATIONAL SECURITY Support RAND Purchase this document Browse Books & Publications Make a charitable contribution For More Information Visit RAND at www.rand.org Explore RAND Science and Technology View document details Limited Electronic Distribution Rights This document and trademark(s) contained herein are protected by law as indicated in a notice appearing later in this work. This electronic representation of RAND intellectual property is provided for non-commercial use only. Permission is required from RAND to reproduce, or reuse in another form, any of our research documents for commercial use. This product is part of the RAND Corporation technical report series. Reports may include research findings on a specific topic that is limited in scope; present discus- sions of the methodology employed in research; provide literature reviews, survey instruments, modeling exercises, guidelines for practitioners and research profes- sionals, and supporting documentation; -

Patients with Positive Preoperative Stress Tests Undergoing Vascular Surgery
Patients With Positive Preoperative Stress Tests Undergoing Vascular Surgery Kyung W. Tim Park, MD, Kathirvel Subramaniam, MD, Feroze Mahmood, MD, Fred Shapiro, MD, Selina Long, MD, and David Napoli, MD Objective: To examine the perioperative cardiac morbidity Cardiology and 7 had a left ventricular ejection fraction and mortality in patients undergoing major vascular surgery <40%. Twenty-three patients had been on a -blocker and with -blockade after a positive stress test or cardiac cath- continued on it, while the remainder started on it de novo eterization. perioperatively. None of the patients suffered from myocar- Design: Retrospective review of a quality assurance data- dial infarction, congestive heart failure, or cardiac death base. perioperatively. Setting: A university teaching hospital. Conclusions: This case series reports on the authors’ ex- Participants: A consecutive series of 31 patients undergo- perience with patients undergoing high-risk vascular sur- ing peripheral vascular or aortic surgery after a positive gery after a positive stress test or catheterization, but with- stress test or catheterization between November 2001 and out an intervening coronary intervention. All patients received perioperative -blockade and had a very low ad- September 2003. verse cardiac event rate. With reduction of adverse events Intervention: None. by -blockade, the likelihood of a positive event may be Measurements and Main Results: All 31 patients had a reduced and the utility of the test in risk stratification may preoperative positive stress test and/or cardiac catheteriza- be questioned. tion, with 12 having multiple areas at risk for myocardial © 2005 Elsevier Inc. All rights reserved. ischemia. None had an intervening coronary revasculariza- tion. -

Diagnosis and Treatment of Lumbar Disc Herniation with Radiculopathy
Y Lumbar Disc Herniation with Radiculopathy | NASS Clinical Guidelines 1 G Evidence-Based Clinical Guidelines for Multidisciplinary ETHODOLO Spine Care M NE I DEL I U /G ON Diagnosis and Treatment of I NTRODUCT Lumbar Disc I Herniation with Radiculopathy NASS Evidence-Based Clinical Guidelines Committee D. Scott Kreiner, MD Paul Dougherty, II, DC Committee Chair, Natural History Chair Robert Fernand, MD Gary Ghiselli, MD Steven Hwang, MD Amgad S. Hanna, MD Diagnosis/Imaging Chair Tim Lamer, MD Anthony J. Lisi, DC John Easa, MD Daniel J. Mazanec, MD Medical/Interventional Treatment Chair Richard J. Meagher, MD Robert C. Nucci, MD Daniel K .Resnick, MD Rakesh D. Patel, MD Surgical Treatment Chair Jonathan N. Sembrano, MD Anil K. Sharma, MD Jamie Baisden, MD Jeffrey T. Summers, MD Shay Bess, MD Christopher K. Taleghani, MD Charles H. Cho, MD, MBA William L. Tontz, Jr., MD Michael J. DePalma, MD John F. Toton, MD This clinical guideline should not be construed as including all proper methods of care or excluding or other acceptable methods of care reason- ably directed to obtaining the same results. The ultimate judgment regarding any specific procedure or treatment is to be made by the physi- cian and patient in light of all circumstances presented by the patient and the needs and resources particular to the locality or institution. I NTRODUCT 2 Lumbar Disc Herniation with Radiculopathy | NASS Clinical Guidelines I ON Financial Statement This clinical guideline was developed and funded in its entirety by the North American Spine Society (NASS). All participating /G authors have disclosed potential conflicts of interest consistent with NASS’ disclosure policy. -

Intravascular Ultrasound and Magnetic Resonance Imaging Of
Intravascular Ultrasound and Magnetic Resonance Imaging of Atherosclerosis and Assessment of Endothelial Function Lachlan Frost Discipline of Medicine, School of Medicine The University of Adelaide & Cardiovascular Research Centre Royal Adelaide Hospital April 2015 Submitted in the total fulfilment of the requirements for the degree of Doctor of Philosophy i THESIS DECLARATION I certify that this work contains no material which has been accepted for the award of any other degree or diploma in any university or other tertiary institution and, to the best of my knowledge and belief, contains no material previously published or written by another person, except where due reference has been made in the text. In addition, I certify that no part of this work will, in the future, be used in a submission for any other degree or diploma in any university or other tertiary institution without the prior approval of the University of Adelaide and where applicable, any partner institution responsible for the joint-award of this degree. I give consent to this copy of my thesis when deposited in the University Library, being made available for loan and photocopying, subject to the provisions of the Copyright Act 1968. I also give permission for the digital version of my thesis to be made available on the web, via the University’s digital research repository, the Library Search and also through web search engines, unless permission has been granted by the University to restrict access for a period of time. Signed, Lachlan Frost University of Adelaide ii THESIS RELATED ABSTRACTS Frost L, Richardson J, Carbone A, Puri R, Nelson A, Sidhartha S, Worthley M, Worthley S.