Baseline Report of Wash4urbanpoor Project
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-
Bangladesh, Year 2019: Update on Incidents According to the Armed Conflict Location & Event Data Project (ACLED)
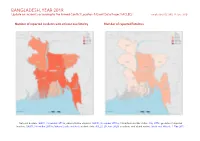
BANGLADESH, YEAR 2019: Update on incidents according to the Armed Conflict Location & Event Data Project (ACLED) compiled by ACCORD, 29 June 2020 Number of reported incidents with at least one fatality Number of reported fatalities National borders: GADM, November 2015b; administrative divisions: GADM, November 2015a; China/India border status: CIA, 2006; geodata of disputed borders: GADM, November 2015b; Natural Earth, undated; incident data: ACLED, 20 June 2020; coastlines and inland waters: Smith and Wessel, 1 May 2015 BANGLADESH, YEAR 2019: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 29 JUNE 2020 Contents Conflict incidents by category Number of Number of reported fatalities 1 Number of Number of Category incidents with at incidents fatalities Number of reported incidents with at least one fatality 1 least one fatality Protests 930 1 1 Conflict incidents by category 2 Riots 405 107 122 Development of conflict incidents from 2010 to 2019 2 Violence against civilians 257 184 195 Battles 99 43 63 Methodology 3 Strategic developments 15 0 0 Conflict incidents per province 4 Explosions / Remote 7 2 2 violence Localization of conflict incidents 4 Total 1713 337 383 Disclaimer 6 This table is based on data from ACLED (datasets used: ACLED, 20 June 2020). Development of conflict incidents from 2010 to 2019 This graph is based on data from ACLED (datasets used: ACLED, 20 June 2020). 2 BANGLADESH, YEAR 2019: UPDATE ON INCIDENTS ACCORDING TO THE ARMED CONFLICT LOCATION & EVENT DATA PROJECT (ACLED) COMPILED BY ACCORD, 29 JUNE 2020 Methodology GADM. Incidents that could not be located are ignored. -

CPD-CMI Working Paper Series Finance for Local Government in Bangladesh an Elusive Agenda 6
CPD-CMI Working Paper Series 6 Finance for Local Government in Bangladesh An Elusive Agenda Debapriya Bhattacharya Mobasser Monem Umme Shefa Rezbana CENTRE FOR POLICY DIALOGUE (CPD) B A N G L A D E S H a c i v i l s o c i e t y t h i n k t a n k Absorbing Innovative Financial Flows: Looking at Asia FINANCE FOR LOCAL GOVERNMENT IN BANGLADESH An Elusive Agenda CPD-CMI Working Paper 6 Debapriya Bhattacharya Mobasser Monem Umme Shefa Rezbana Dr Debapriya Bhattacharya is a Distinguished Fellow at the Centre for Policy Dialogue (CPD); Dr Mobasser Monem is Professor, Department of Public Administration, University of Dhaka and Ms Umme Shefa Rezbana is Research Associate, CPD. i CPD Working Paper 000 Publishers Centre for Policy Dialogue (CPD) House 40C, Road 32, Dhanmondi R/A Dhaka 1209, Bangladesh Telephone: (+88 02) 8124770, 9126402, 9141703, 9141734 Fax: (+88 02) 8130951; E-mail: [email protected] Website: cpd.org.bd Chr. Michelsen Institute (CMI) Jekteviksbakken 31, 5006 Bergen, Norway P.O. Box 6033 Bedriftssenteret, N-5892 Bergen, Norway Telephone: (+47 47) 93 80 00; Fax: (+47 47) 93 80 01 E-mail: [email protected]; Website: www.cmi.no First Published November 2013 © Centre for Policy Dialogue (CPD) Disclaimer: The views expressed in this paper are those of the authors alone and do not necessarily reflect the views of CPD or CMI. Tk. 90 USD 6 ISSN 2225-8175 (Online) ISSN 2225-8035 (Print) Cover Design Avra Bhattacharjee CCM42013_3WP6_DGP ii Absorbing Innovative Financial Flows: Looking at Asia The present Working Paper Series emerged from a joint collaborative programme being implemented by the Centre for Policy Dialogue (CPD), Dhaka, Bangladesh and the Chr. -

Sakhipur, Bangladesh
Small town sanitation learning series Sakhipur, Bangladesh July 2020 View of the co-composting plant and its drying beds in the foreground WaterAid/ Al-Emran WaterAid/ Key messages 1. The small town of Sakhipur is on track to achieve town-wide safely managed sanitation, the result of technical excellence (including its co-composting plant), political drive, a clear vision, and support by WaterAid Bangladesh. 2. Local partnerships are vital to close the sanitation service chain such as the Agricultural Extension Department. 3. The sanitation vision includes both considering sanitation as a service and using the principles of circular economy. 4. Fostering municipal leadership and ownership is a slow but critical process, which can be the focus of national level advocacy for future replication. 1 / Small town sanitation learning series Sakhipur, Bangladesh July 2020 1. Introduction WaterAid Bangladesh (WAB) and the Bangladesh Association for Social Advancement (BASA) have supported Sakhipur Municipality both technically and financially to establish a co-composting plant in 2015. The plant treats both faecal sludge and organic solid waste to produce compost. The technical achievement has been well recognised and documented. This brief is mainly focusing at non-technical aspects, especially how this plant (and work around it) is paving the way for full safely-managed sanitation in the town, what has led to this success, and how it could be replicated. 2. Context Bangladesh has impressively reached almost zero open defecation and is now facing the “second generation” challenge of faecal sludge management (FSM) – with 32% “safely managed sanitation” in rural areas, and no urban estimate. -
Human Rights Monitoring Report
Human Rights Monitoring Report 1 – 31 May 2018 1 June 2018 1 Odhikar has, since 1994, been monitoring the human rights situation in Bangladesh in order to promote and protect civil, political, economic, social and cultural rights of Bangladeshi citizens and to report on violations and defend the victims. Odhikar does not believe that the human rights movement merely endeavours to protect the „individual‟ from violations perpetrated by the state; rather, it believes that the movement to establish the rights and dignity of every individual is part of the struggle to constitute Bangladesh as a democratic state. Odhikar has always been consistent in creating mass awareness of human rights issues using several means, including reporting violations perpetrated by the State and advocacy and campaign to ensure internationally recognised civil and political rights of citizens. The Organisation unconditionally stands by the victims of oppression and maintains no prejudice with regard to political leanings or ideological orientation, race, religion or sex. In line with this campaign, Odhikar prepares and releases human rights status reports every month. The Organisation has prepared and disseminated this human rights monitoring report of May 2018, despite facing persecution and continuous harassment and threats to its existence since 2013. Although many incidents of human rights violations occur every month, only a few significant incidents have been highlighted in this report. Information used in the report was gathered by grassroots human rights -

Stakeholders Meeting
Study on IBFB International Business Forum of Bangladesh (IBFB) CONTENTS Page No. 01. Contents . .. … . ……… 2 02. Executive Summary .................................................................... 3 03. Introduction …………………………………………… 5 04. Objectives of the Study . ………………………………………………….. 5 05. Methodology ………………………………………………………………………… 6 06. City Corporations in Bangladesh ………………………………………………….. 6 07. The Provision of the Local Government in the Constitution ………………………. 6 08. Elements of good governance ……………………………………..…….. 7 09. Contribution of Cities to GDP ……………………………………………………. 8 10. Urbanization Trend in Bangladesh ………………………………………………… 8 11. Constraints in the Present City Governance . 9 12. Private Sector Participation and City Governance ………………………….…. 11 13. Investment Climate for Private Participation ……………………………….…. 13 14. Recommendations ………………………………………………. 14 15. REFERENCES ………………………………………… 15 16. ANNEXES: Annex -01: Historical Perspective of City Governance ………………………. …... 17 Annex -02: Evolution & Upgradation of City Government in Bangladesh …….… … 18 Annex -03: City Corporation in Bangladesh ………………………………….. 19 Annex -04: Functions of Urban Government bodies ………………………………….. 21 wmwU Ki‡cv‡ikb msµvšÍ g~j AvBb I ms‡kvwaZ AvBbmg~n Annex -05: …………………………… 22 Annex -06: The Unified City Corporation Act (Act N0. 60 of 2009) …………………. 23 Annex -07: A short view of Details of Functions of Corporations ……………….......... 25 (As per schedule 3 and clause 41 of Act No. 60, 2009) Annex -08: List of representation from different Govt. departments for ………………. 27 attending City Corporation‟s meeting (as per Act No. 60 of 2009) Annex- 09: Global Good Practice on City Governance ……………………………... 29 2 Executive Summary The in-house research paper on „Improving City Governance and Private Sector Development’ is intended to explore the ground reality of city governance –how it functions, its constraints and how people, particularly city dwellers, can harness better civic amenities from the existing system. -

Climate Vulnerability Assessment: Impacts on Health Outcomes in Secondary Cities Of
TECHNICAL REPORT CLIMATE VULNERABILITY ASSESSMENT: IMPACTS ON HEALTH OUTCOMES IN SECONDARY CITIES OF BANGLADESH January 2020 This document was produced for review by the United States Agency for International Development. It was prepared by Chemonics International for the Adaptation Thought Leadership and Assessments (ATLAS) Task Order No. AID-OAA-TO- 14-00044, under the Restoring the Environment through Prosperity, Livelihoods, and Conserving Ecosystems (REPLACE) IDIQ. Chemonics contact: Chris Perine, Chief of Party ([email protected])- Chemonics International Inc. 1717 H Street NW Washington, DC 20006 ATLAS reports and other products are available on the ClimateLinks website: https://www.climatelinks.org/projects/atlas Cover Photo: View of Khulna City, Goran Hoglund (Kartlasarn), 2016. CLIMATE VULNERABILITY ASSESSMENT: IMPACTS ON HEALTH OUTCOMES IN SECONDARY CITIES OF BANGLADESH January 2020 Prepared for: United States Agency for International Development Adaptation Thought Leadership and Assessments (ATLAS) Prepared by: Chemonics International Inc. Fernanda Zermoglio, Aneire Khan, Sophia Dahodwala and Chris Perine This report is made possible by the support of the American people through the United States Agency for International Development (USAID). The contents of this report are the sole responsibility of the author or authors and do not necessarily reflect the views of USAID or the United States Government. CONTENTS LIST OF FIGURES AND TABLES ······································································ I ACRONYMS -
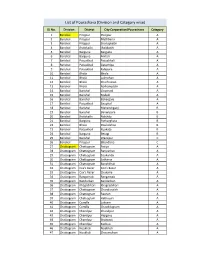
List of Pourashava (Division and Category Wise)
List of Pourashava (Division and Category wise) SL No. Division District City Corporation/Pourashava Category 1 Barishal Pirojpur Pirojpur A 2 Barishal Pirojpur Mathbaria A 3 Barishal Pirojpur Shorupkathi A 4 Barishal Jhalokathi Jhalakathi A 5 Barishal Barguna Barguna A 6 Barishal Barguna Amtali A 7 Barishal Patuakhali Patuakhali A 8 Barishal Patuakhali Galachipa A 9 Barishal Patuakhali Kalapara A 10 Barishal Bhola Bhola A 11 Barishal Bhola Lalmohan A 12 Barishal Bhola Charfession A 13 Barishal Bhola Borhanuddin A 14 Barishal Barishal Gournadi A 15 Barishal Barishal Muladi A 16 Barishal Barishal Bakerganj A 17 Barishal Patuakhali Bauphal A 18 Barishal Barishal Mehendiganj B 19 Barishal Barishal Banaripara B 20 Barishal Jhalokathi Nalchity B 21 Barishal Barguna Patharghata B 22 Barishal Bhola Doulatkhan B 23 Barishal Patuakhali Kuakata B 24 Barishal Barguna Betagi B 25 Barishal Barishal Wazirpur C 26 Barishal Pirojpur Bhandaria C 27 Chattogram Chattogram Patiya A 28 Chattogram Chattogram Bariyarhat A 29 Chattogram Chattogram Sitakunda A 30 Chattogram Chattogram Satkania A 31 Chattogram Chattogram Banshkhali A 32 Chattogram Cox's Bazar Cox’s Bazar A 33 Chattogram Cox's Bazar Chakaria A 34 Chattogram Rangamati Rangamati A 35 Chattogram Bandarban Bandarban A 36 Chattogram Khagrchhari Khagrachhari A 37 Chattogram Chattogram Chandanaish A 38 Chattogram Chattogram Raozan A 39 Chattogram Chattogram Hathazari A 40 Chattogram Cumilla Laksam A 41 Chattogram Cumilla Chauddagram A 42 Chattogram Chandpur Chandpur A 43 Chattogram Chandpur Hajiganj A -

Evaluation of Netherlands-Funded Ngos in Bangladesh
Evaluation of Netherlands-funded NGOs in Bangladesh Ministry of Foreign Affairs, Policy and Operations Evaluation Department (IOB) ISBN 90-5328-163-0 Photographs: Ron Giling/LINEAIR Maps and figures: Geografiek, Amsterdam Pre-press services: Transcripta, Beerzerveld Printed by: Ridderprint BV, Ridderkerk Preface The evaluation of Netherlands supported NGOs in Bangladesh forms part of a study undertaken by the Policy and Operations Evaluation Department (IOB) on the Netherlands bi-lateral aid programme for Bangladesh in the period 1972–96. The support to NGOs through the regular aid programme and through the Co-financing Programme has been important to the Netherlands’ pursuance of poverty alleviation objectives in Bangladesh. A total of Dfl. .247 million has been disbursed through these channels, some three quarters of which after 1990. The position of NGOs in Bangladeshi society is quite unique. Bangladesh is home to the largest national NGOs in the world, as well as to a multitude of middle- and small-sized NGOs that operate on a national, regional or local level. The Bangladeshi NGOs literally reach out to millions of people in both rural and urban areas. This study comprises extensive case studies of a cross section of NGOs in Bangladesh. Both the Bangladeshi NGOs that were subject of study and their partners in the Netherlands, Bilance (formerly Cebemo), ICCO and Novib, have been closely involved in the various stages of the study. The study has concentrated on the credit and training activities that constitute the mainstay of NGO programmes. It is concluded that these activities effectively target the poorer sections of the population, particularly women. -

Division Zila Upazila Name of Upazila/Thana 10 10 04 10 04
Geo Code list (upto upazila) of Bangladesh As On March, 2013 Division Zila Upazila Name of Upazila/Thana 10 BARISAL DIVISION 10 04 BARGUNA 10 04 09 AMTALI 10 04 19 BAMNA 10 04 28 BARGUNA SADAR 10 04 47 BETAGI 10 04 85 PATHARGHATA 10 04 92 TALTALI 10 06 BARISAL 10 06 02 AGAILJHARA 10 06 03 BABUGANJ 10 06 07 BAKERGANJ 10 06 10 BANARI PARA 10 06 32 GAURNADI 10 06 36 HIZLA 10 06 51 BARISAL SADAR (KOTWALI) 10 06 62 MHENDIGANJ 10 06 69 MULADI 10 06 94 WAZIRPUR 10 09 BHOLA 10 09 18 BHOLA SADAR 10 09 21 BURHANUDDIN 10 09 25 CHAR FASSON 10 09 29 DAULAT KHAN 10 09 54 LALMOHAN 10 09 65 MANPURA 10 09 91 TAZUMUDDIN 10 42 JHALOKATI 10 42 40 JHALOKATI SADAR 10 42 43 KANTHALIA 10 42 73 NALCHITY 10 42 84 RAJAPUR 10 78 PATUAKHALI 10 78 38 BAUPHAL 10 78 52 DASHMINA 10 78 55 DUMKI 10 78 57 GALACHIPA 10 78 66 KALAPARA 10 78 76 MIRZAGANJ 10 78 95 PATUAKHALI SADAR 10 78 97 RANGABALI Geo Code list (upto upazila) of Bangladesh As On March, 2013 Division Zila Upazila Name of Upazila/Thana 10 79 PIROJPUR 10 79 14 BHANDARIA 10 79 47 KAWKHALI 10 79 58 MATHBARIA 10 79 76 NAZIRPUR 10 79 80 PIROJPUR SADAR 10 79 87 NESARABAD (SWARUPKATI) 10 79 90 ZIANAGAR 20 CHITTAGONG DIVISION 20 03 BANDARBAN 20 03 04 ALIKADAM 20 03 14 BANDARBAN SADAR 20 03 51 LAMA 20 03 73 NAIKHONGCHHARI 20 03 89 ROWANGCHHARI 20 03 91 RUMA 20 03 95 THANCHI 20 12 BRAHMANBARIA 20 12 02 AKHAURA 20 12 04 BANCHHARAMPUR 20 12 07 BIJOYNAGAR 20 12 13 BRAHMANBARIA SADAR 20 12 33 ASHUGANJ 20 12 63 KASBA 20 12 85 NABINAGAR 20 12 90 NASIRNAGAR 20 12 94 SARAIL 20 13 CHANDPUR 20 13 22 CHANDPUR SADAR 20 13 45 FARIDGANJ -
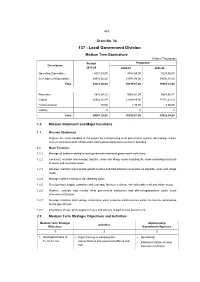
137 - Local Government Division
453 Grant No. 34 137 - Local Government Division Medium Term Expenditure (Taka in Thousands) Budget Projection Description 2019-20 2020-21 2021-22 Operating Expenditure 4321,54,00 4753,69,00 5229,06,00 Development Expenditure 29919,66,00 31541,98,00 34696,18,00 Total 34241,20,00 36295,67,00 39925,24,00 Recurrent 7815,04,16 9003,87,04 8807,80,41 Capital 26425,35,84 27289,84,96 31115,37,59 Financial Asset 80,00 1,95,00 2,06,00 Liability 0 0 0 Total 34241,20,00 36295,67,00 39925,24,00 1.0 Mission Statement and Major Functions 1.1 Mission Statement Improve the living standard of the people by strengthening local government system, developing climate resilient rural and urban infrastructure and implementing socio-economic activities. 1.2 Major Functions 1.2.1 Manage all matters relating to local government and local government institutions; 1.2.2 Construct, maintain and manage Upazilla, union and village roads including the roads and bridges/culverts of towns and municipal areas; 1.2.3 Develop, maintain and manage growth centres and hats-bazaars connected via Upazilla, union and village roads; 1.2.4 Manage matters relating to safe drinking water; 1.2.5 Develop water supply, sanitation and sewerage facilities in climate risk vulnerable rural and urban areas; 1.2.6 Finance, evaluate and monitor local government institutions and offices/organizations under Local Government Division; 1.2.7 Develop, maintain and manage small-scale water resource infrastructures within the timeline determined by the government. 1.2.8 Enactment of Law, promulgation of rules and policies related to local government. -

Land Resource Appraisal of Bangladesh for Agricultural
BGD/81/035 Technical Report 3 Volume II LAND RESOURCES APPRAISAL OF BANGLADESH FOR AGRICULTURAL DEVELOPMENT REPORT 3 LAND RESOURCES DATA BASE VOLUME II SOIL, LANDFORM AND HYDROLOGICAL DATA BASE A /UNITED NATIONS DEVELOPMENT PROGRAMME FAo FOOD AND AGRICULTURE ORGANIZATION vJ OF THE UNITED NATIONS BGD/81/035 Technical Report 3 Volume II LAND RESOURCES APPRAISAL OF BANGLADESH FOR AGRICULTURALDEVELOPMENT REPORT 3 LAND RESOURCES DATA BASE VOLUME II SOIL, LANDFORM AND HYDROLOGICAL DATA BASE Report prepared for the Government of the People's Republic of Bangladesh by the Food and Agriculture Organization of the United Nations acting as executing agency for the United Nations Development Programme based on the work of H. Brammer Agricultural Development Adviser J. Antoine Data Base Management Expert and A.H. Kassam and H.T. van Velthuizen Land Resources and Agricultural Consultants UNITED NATIONS DEVELOPMENT PROGRAMME FOOD AND AGRICULTURE ORGANIZATION OF THE UNITED NATIONS Rome, 1988 The designations employed and the presentation of material in this publication do not imply the expression of any opinion whatsoever on the part of the Food and AgricultureOrganization of the United Nations concerning the legal status of any country, territory, city or area or of its authorities, or concerning the delimitation of its frontiers or boundaries. All rights reserved. No part of this publication may be reproduced, stored ina retrieval system, or transmitted in any form or by any means, electronic, mechanical, photocopyingor otherwise, without the prior perrnission of (he copyright owner. Applications for such permission,with a statement of the purpose and extent of the reproduction, should be addressedto the Director, Publications Division, Food and Agriculture Organization of the United Nations, Viadelle Terme di Caracarla, 00100 Home, Italy. -

List of Madrsha
List of Madrasha Division BARISAL District BARGUNA Thana AMTALI Sl Eiin Name Village/Road Mobile 1 100065 WEST CHILA AMINIA FAZIL MADRASAH WEST CHILA 01716835134 2 100067 MOHAMMADPUR MAHMUDIA DAKHIL MADRASAH MOHAMMADPUR 01710322701 3 100069 AMTALI BONDER HOSAINIA FAZIL MADRASHA AMTALI 01714599363 4 100070 GAZIPUR SENIOR FAZIL (B.A) MADRASHA GAZIPUR 01724940868 5 100071 KUTUBPUR FAZIL MADRASHA KRISHNA NAGAR 01715940924 6 100072 UTTAR KALAMPUR HATEMMIA DAKHIL MADRASA KAMALPUR 01719661315 7 100073 ISLAMPUR HASHANIA DAKHIL MADRASHA ISLAMPUR 01745566345 8 100074 MOHISHKATA NESARIA DAKHIL MADRASA MOHISHKATA 01721375780 9 100075 MADHYA TARIKATA DAKHIL MADRASA MADHYA TARIKATA 01726195017 10 100076 DAKKHIN TAKTA BUNIA RAHMIA DAKHIL MADRASA DAKKHIN TAKTA BUNIA 01718792932 11 100077 GULISHAKHALI DAKHIL MDRASHA GULISHAKHALI 01706231342 12 100078 BALIATALI CHARAKGACHHIA DAKHIL MADRASHA BALIATALI 01711079989 13 100080 UTTAR KATHALIA DAKHIL MADRASAH KATHALIA 01745425702 14 100082 PURBA KEWABUNIA AKBARIA DAKHIL MADRASAH PURBA KEWABUNIA 01736912435 15 100084 TEPURA AHMADIA DAKHIL MADRASA TEPURA 01721431769 16 100085 AMRAGACHIA SHALEHIA DAKHIL AMDRASAH AMRAGACHIA 01724060685 17 100086 RAHMATPUR DAKHIL MADRASAH RAHAMTPUR 01791635674 18 100088 PURBA PATAKATA MEHER ALI SENIOR MADRASHA PATAKATA 01718830888 19 100090 GHOP KHALI AL-AMIN DAKHIL MADRASAH GHOPKHALI 01734040555 20 100091 UTTAR TEPURA ALAHAI DAKHIL MADRASA UTTAR TEPURA 01710020035 21 100094 GHATKHALI AMINUDDIN GIRLS ALIM MADRASHA GHATKHALI 01712982459 22 100095 HARIDRABARIA D.S. DAKHIL MADRASHA HARIDRABARIA