Gastric Outlet Obstruction in a Patient with Bouveret's
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Intestinal Obstruction
Intestinal obstruction Prof. Marek Jackowski Definition • Any condition interferes with normal propulsion and passage of intestinal contents. • Can involve the small bowel, colon or both small and colon as in generalized ileus. Definitions 5% of all acute surgical admissions Patients are often extremely ill requiring prompt assessment, resuscitation and intensive monitoring Obstruction a mechanical blockage arising from a structural abnormality that presents a physical barrier to the progression of gut contents. Ileus a paralytic or functional variety of obstruction Obstruction: Partial or complete Simple or strangulated Epidemiology 1 % of all hospitalization 3-5 % of emergency surgical admissions More frequent in female patients - gynecological and pelvic surgical operations are important etiologies for postop. adhesions Adhesion is the most common cause of intestinal obstruction 80% of bowel obstruction due to small bowel obstruction - the most common causes are: - Adhesion - Hernia - Neoplasm 20% due to colon obstruction - the most common cause: - CR-cancer 60-70%, - diverticular disease and volvulus - 30% Mortality rate range between 3% for simple bowel obstruction to 30% when there is strangulation or perforation Recurrent rate vary according to method of treatment ; - conservative 12% - surgical treatment 8-32% Classification • Cause of obstruction: mechanical or functional. • Duration of obstruction: acute or chronic. • Extent of obstruction: partial or complete • Type of obstruction: simple or complex (closed loop and strangulation). CLASSIFICATION DYNAMIC ADYNAMIC (MECHANICAL) (FUNCTIONAL) Peristalsis is Result from atony of working against a the intestine with loss mechanical of normal peristalsis, obstruction in the absence of a mechanical cause. or it may be present in a non-propulsive form (e.g. mesenteric vascular occlusion or pseudo-obstruction) Etiology Mechanical bowel obstruction: A. -

Inflammatory Bowel Disease Irritable Bowel Syndrome
Inflammatory Bowel Disease and Irritable Bowel Syndrome Similarities and Differences 2 www.ccfa.org IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 Important Differences Between IBD and IBS Many diseases and conditions can affect the gastrointestinal (GI) tract, which is part of the digestive system and includes the esophagus, stomach, small intestine and large intestine. These diseases and conditions include inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS). IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 www.ccfa.org 3 Inflammatory bowel diseases are a group of inflammatory conditions in which the body’s own immune system attacks parts of the digestive system. Inflammatory Bowel Disease Inflammatory bowel diseases are a group of inflamma- Causes tory conditions in which the body’s own immune system attacks parts of the digestive system. The two most com- The exact cause of IBD remains unknown. Researchers mon inflammatory bowel diseases are Crohn’s disease believe that a combination of four factors lead to IBD: a (CD) and ulcerative colitis (UC). IBD affects as many as 1.4 genetic component, an environmental trigger, an imbal- million Americans, most of whom are diagnosed before ance of intestinal bacteria and an inappropriate reaction age 35. There is no cure for IBD but there are treatments to from the immune system. Immune cells normally protect reduce and control the symptoms of the disease. the body from infection, but in people with IBD, the immune system mistakes harmless substances in the CD and UC cause chronic inflammation of the GI tract. CD intestine for foreign substances and launches an attack, can affect any part of the GI tract, but frequently affects the resulting in inflammation. -

Necrotizing Enterocolitis: Intraluminal Biochemistry in Human Neonates and a Rabbit Model
003 1-3998/85/ 1909-09 19$02.00/0 PEDIATRIC RESEARCH Vol. 19, No. 9, 1985 Copyright O 1985 International Ped~atncResearch Foundation, Inc. Prinrc~din U.S/1 Necrotizing Enterocolitis: Intraluminal Biochemistry in Human Neonates and a Rabbit Model DAVID A. CLARK. JEFFREY E. THOMPSON. LEONARD B. WEINER, JULIA A. McMILLAN, ALBERT J. SCHNEIDER, AND JOHN E. ROKAHR Dcy~crriincnio/'Pcdiarric.s. SU/L'Y, Ill,.siutc Meclrcul Cmtcr, Syrucir.cc, NPW York ABSTRACT. The intestinal contents of 17 neonates with amined the intestinal contents of preterm infants with severe necrotizing enterocolitis were analyzed for pH, carbohy- necrotizing enterocolitis. The low intraluminal pH and high drate, protein, and bacteria. The intraluminal pH was 4.0 protein content in the intestines of these neonates led us to (16117). Sufficient carbohydrate and bacteria capable of examine the variables of pH and protein in a rabbit intestinal fermenting the carbohydrate to organic acids were found. loop model. The intraluminal protein content was >S g/dl. The varia- bles of acid and protein were then examined in a rabbit intestinal loop model. The hemorrhagic response in indi- MATERIALS AND METHODS vidual loops was measured using Cr5' tagged red blood Nronute.~.We obtained the intestinal contents at or adjacent cells such that the microliters of blood per centimeter to the site of perforation or necrosis in 17 infants requiring intestine could be determined. Loops with organic acid and surgical removal of the intestine for advanced necrotizing enter- protein had significantly (p < 0.01) more intramural blood ocolitis. The intestinal contents were analyzed for blood, pH, than control loops. -

Acute Gastroenteritis
Article gastrointestinal disorders Acute Gastroenteritis Deise Granado-Villar, MD, Educational Gap MPH,* Beatriz Cunill-De Sautu, MD,† Andrea In managing acute diarrhea in children, clinicians need to be aware that management Granados, MDx based on “bowel rest” is outdated, and instead reinstitution of an appropriate diet has been associated with decreased stool volume and duration of diarrhea. In general, drug therapy is not indicated in managing diarrhea in children, although zinc supplementation Author Disclosure and probiotic use show promise. Drs Granado-Villar, Cunill-De Sautu, and Objectives After reading this article, readers should be able to: Granados have disclosed no financial 1. Recognize the electrolyte changes associated with isotonic dehydration. relationships relevant 2. Effectively manage a child who has isotonic dehydration. to this article. This 3. Understand the importance of early feedings on the nutritional status of a child who commentary does has gastroenteritis. contain a discussion of 4. Fully understand that antidiarrheal agents are not indicated nor recommended in the an unapproved/ treatment of acute gastroenteritis in children. investigative use of 5. Recognize the role of vomiting in the clinical presentation of acute gastroenteritis. a commercial product/ device. Introduction Acute gastroenteritis is an extremely common illness among infants and children world- wide. According to the Centers for Disease Control and Prevention (CDC), acute diarrhea among children in the United States accounts for more than 1.5 million outpatient visits, 200,000 hospitalizations, and approximately 300 deaths per year. In developing countries, diarrhea is a common cause of mortality among children younger than age 5 years, with an estimated 2 million deaths each year. -

A Case Report of Fibro-Stenotic Crohn's Disease in the Middle
DOI: https://doi.org/10.22516/25007440.185 Case report A Case Report of Fibro-Stenotic Crohn’s Disease in the Middle Ileum as the Initial Manifestation Adriana Margarita Rey,1 Gustavo Reyes,1 Fernando Sierra,1 Rafael García-Duperly,2 Rocío López,3 Leidy Paola Prada.4 1 Gastroenterologist in the Gastroenterology and Abstract Hepatology Service of the Hospital Universitario Fundación Santa Fe de Bogotá in Bogotá, Colombia Crohn’s disease (CD) is an inflammatory bowel disease that can affect the entire gastrointestinal tract. The small 2 Colon and Rectum Surgeon in the Department of intestine is affected in about 50% of patients among whom the terminal ileum is the area most commonly affected. Surgery of the Hospital Universitario Fundación Intestinal stenosis is a common complication in CD and approximately 30% to 50% of patients present Santa Fe de Bogotá in Bogotá, Colombia 3 Pathologist at of the Hospital Universitario Fundación stenosis or penetrating lesions at the time of diagnosis. Because conventional endoscopic techniques do not Santa Fe de Bogotá and Professor at Universidad de allow evaluation of small bowel lesions, techniques such as enteroscopy and endoscopic video-capsule were los Andes in Bogotá, Colombia developed. Each has advantages and indications. 4 Third Year Internal Medicine Resident at the Hospital Universitario Fundación Santa Fe de Bogotá in We present the case of a patient with CD with localized fibrostenosis in the middle ileum which is not a Bogotá, Colombia frequent site for this type of lesion. Author for correspondence: Adriana Margarita Rey. Bogotá D.C. Colombia [email protected] Keywords ........................................ -

Diagnostic Imaging Features of Necrotizing Enterocolitis: a Narrative Review
Review Article Diagnostic imaging features of necrotizing enterocolitis: a narrative review Francesco Esposito1, Rosanna Mamone1, Marco Di Serafino2, Carmela Mercogliano3, Valerio Vitale4, Gianfranco Vallone5, Patrizia Oresta1 1Department of Radiology, Santobono-Pausilipon Children Hospital, Naples; Italy; 2Department of Emergency Radiology, 3Department of Neonatology, San Carlo Hospital, Potenza; Italy; 4Department of Imaging and Radiation therapy, Azienda Socio-Sanitaria Territoriale di Lecco, A. Manzoni Hospital, Lecco, Italy; 5Department of Radiology, Section of Pediatric Diagnostics, University Hospital “Federico II”, Naples, Italy Correspondence to: Dr. Francesco Esposito. Santobono Hospital, Via M. Fiore, 6, 80100 Napoli, Naples, Italy. Email: [email protected]. Abstract: Necrotizing enterocolitis (NEC) is an inflammatory process, characterized by intestinal necrosis of variable extension, leading to perforation, generalized peritonitis and death. The classical pathogenetic theory focuses on mucosal damage related to a stress induced intestinal ischemia leading to mucosal injury and bacterial colonization of the wall. A more recent hypothesis emphasizes the role of immaturity of gastrointestinal and immune system, particularly of the premature, responsible of bowel wall vulnerability and suffering. NEC is the most common gastrointestinal emergency in the newborn, with a higher incidence in the preterm; improvement of neonatal resuscitation techniques enables the survival of premature of very low birth weight (VLBW) with prolongation -

Adult Intussusception
1 Adult Intussusception Saulius Paskauskas and Dainius Pavalkis Lithuanian University of Health Sciences Kaunas Lithuania 1. Introduction Intussusception is defined as the invagination of one segment of the gastrointestinal tract and its mesentery (intussusceptum) into the lumen of an adjacent distal segment of the gastrointestinal tract (intussuscipiens). Sliding within the bowel is propelled by intestinal peristalsis and may lead to intestinal obstruction and ischemia. Adult intussusception is a rare condition wich can occur in any site of gastrointestinal tract from stomach to rectum. It represents only about 5% of all intussusceptions (Agha, 1986) and causes 1-5% of all cases of intestinal obstructions (Begos et al., 1997; Eisen et al., 1999). Intussusception accounts for 0.003–0.02% of all hospital admissions (Weilbaecher et al., 1971). The mean age for intussusception in adults is 50 years, and and the male-to-female ratio is 1:1.3 (Rathore et. al., 2006). The child to adult ratio is more than 20:1. The condition is found in less than 1 in 1300 abdominal operations and 1 in 100 patients operated for intestinal obstruction. Intussusception in adults occurs less frequently in the colon than in the small bowel (Zubaidi et al., 2006; Wang et al., 2007). Mortality for adult intussusceptions increases from 8.7% for the benign lesions to 52.4% for the malignant variety (Azar & Berger, 1997) 2. Etiology of adult intussusception Unlike children where most cases are idiopathic, intussusception in adults has an identifiable etiology in 80- 90% of cases. The etiology of intussusception of the stomach, small bowel and the colon is quite different (Table 1). -

Gallstone Ileus As an Unexpected Complication of Cholelithiasis: Diagnostic Difficulties and Treatment
Turkish Journal of Trauma & Emergency Surgery Ulus Travma Acil Cerrahi Derg 2010;16 (4):344-348 Original Article Klinik Çalışma Gallstone ileus as an unexpected complication of cholelithiasis: diagnostic difficulties and treatment Kolelitiazisin beklenmedik komplikasyonu, safra taşı ileusu: Tanı zorlukları ve tedavi Savaş YAKAN,1 Ömer ENGİN,1 Tahsin TEKELİ,1 Bülent ÇALIK,2 Ali Galip DENEÇLİ,1 Ahmet ÇOKER,3 Mustafa HARMAN4 BACKGROUND AMAÇ Gallstone ileus is a rare complication of cholelithiasis, Safra taşı ileusu safra taşı hastalığının nadir ve genelde mostly in the elderly. The aim of this study was to evaluate yaşlılarda görülen bir komplikasyonudur. Çalışmamızın our experience with 12 gallstone ileus cases and discuss amacı safra taşı ileusu tanısı alan 12 hastayla ilgili dene- current opinion as reported in the literature. yimimizi değerlendirmek ve güncel literatür eşliğinde tar- tışmaktır. METHODS Data of 12 patients operated between January 1998 and GEREÇ VE YÖNTEM January 2008 with gallstone ileus were retrospectively Kliniğimizde Ocak 1998-2008 yılları arasında safra taşı ile- studied. usu nedeniyle ameliyat edilen 12 olgunun dosyaları retros- pektif olarak incelendi. RESULTS There were 12 cases (9 F, 75%; 3 M, 25%) with a mean age BULGULAR of 63.6 (50-80) years. Median duration of symptoms before Hastaların 9’u (%75) kadın, 3’ü (%25) erkek olup orta- admission to the hospital was 4.1 (1-15) days. Preoperative lama yaş 63,6 idi (dağılım, 50-80). Semptomların başla- diagnosis was made in only five cases (41.6%). Enteroli- masından hastaneye başvurmaya kadar geçen süre ortala- thotomy was done in nine cases (75%). Enterolithotomy and ma 4,1 (dağılım, 1-15) gün bulundu. -
Recognizing-Consitpation-And-Bowel
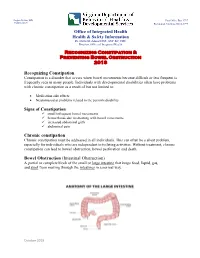
Hughes Melton, MD Post Office Box 1797 Commissioner Richmond, Virginia 23218-1797 Office of Integrated Health Health & Safety Information Dr. Dawn M. Adams DNP, ANP-BC, CHC Director, Office of Integrated Health Recognizing Constipation & Preventing Bowel Obstruction 2018 Recognizing Constipation Constipation is a disorder that occurs when bowel movements become difficult or less frequent is frequently seen in many people. Individuals with developmental disabilities often have problems with chronic constipation as a result of but not limited to: Medication side effects Neuromuscular problems related to the person's disability Signs of Constipation small infrequent bowel movements hemorrhoids due to straining with bowel movements increased abdominal girth abdominal pain Chronic constipation Chronic constipation must be addressed in all individuals. This can often be a silent problem, especially for individuals who are independent in toileting activities. Without treatment, chronic constipation can lead to bowel obstruction, bowel perforation and death. Bowel Obstruction (Intestinal Obstruction) A partial or complete block of the small or large intestine that keeps food, liquid, gas, and stool from moving through the intestines in a normal way. October 2018 Hughes Melton, MD Post Office Box 1797 Commissioner Richmond, Virginia 23218-1797 Bowel obstructions may be caused by a twist in the intestines. Intestines are called the gut. The large intestine includes the appendix, cecum, colon, and rectum and is 5 feet long. It absorbs water from stool and changes it from a liquid to a solid form. The small intestine is where most digestion occurs. It measures about 20 feet and includes the duodenum, jejunum, and ileum. o Digestion is the process of breaking down food into substances the body can use for energy, tissue growth, and repair. -

Ileus with Hypothyroidism
Ileus With Hypothyroidism Mason Thompson, MD, and Paul M. Fischer, MD Augusta, G eorgia he symptoms of constipation and gaseous disten vealed no signs of hypothyroidism except for a flat T sion are often seen in patients with hypothy affect. These studies showed a free thyroxine (T4) level roidism and are evidence of diminished bowel motility. of 4.7 /xg/mL and a thyroid-stimulating hormone (TSH) In its extreme this problem can result in an acute ileus level of 41.1 /uU/mL. or “pseudo-obstruction.” 1 This dramatic presentation She was placed on L-thyroxine and had no further may be the first indication to the clinician that the difficulty with ileus. Her L-thyroxine was unfortu patient is hypothyroid. This report describes two cases nately omitted approximately one year later for a of myxedema ileus with unusual presentations and re period of 19 days during an admission to the psychiat views the literature on this condition. ric floor. During this period she developed symptoms of acute hypothyroidism manifested by massive edema, shortness of breath, and lethargy. A TSH read CASE R E P O R TS ing was later reported to be greater than 50 /uU/mL during this acute withdrawal period prior to restarting CASE 1 the L-thyroxine. These symptoms promptly abated A previously healthy 48-year-old woman was admitted after restarting her thyroid medication. for lower abdominal pain. An ultrasound examination revealed a cystic mass in the left pelvis, which was felt CASE 2 to be an ovarian remnant resulting from a previous abdominal hysterectomy and a bilateral salpingo- A 48-year-old woman presented with a 36-hour history oophorectomy. -

Patient Selection Criteria
M∙ACS MACS Patient Selection Criteria The objective is to screen, on a daily basis, the Acute Care Surgical service “touches” at your hospital to identify patients who meet criteria for further data entry. The specific patient diseases/conditions that we are interested in capturing for emergent general surgery (EGS) are: 1. Acute Appendicitis 2. Acute Gallbladder Disease a. Acute Cholecystitis b. Choledocholithiasis c. Cholangitis d. Gallstone Pancreatitis 3. Small Bowel Obstruction a. Adhesive b. Hernia 4. Emergent Exploratory Laparotomy (Refer to the ex-lap algorithm under the Diseases or Conditions section below for inclusion/exclusion criteria.) The daily census for patients admitted to the Acute Care Surgery Service or seen as a consult will have to be screened. There may be other sources to accomplish this screening such as IT and we are interested in learning about these sources from you. From this census, a list can be compiled of patients with the aforementioned diseases/conditions. The first level of data entry involves capture and entry of the patient into the MACS Qualtrics database. All patients with the identified diseases/conditions will have data entered regardless of whether or not they received an operation during admission/ED visit. The second level of data entry takes place if an existing MACS patient returns to the hospital (ED or admission) or has outcome events identified within the 30-day post-operative time frame if the patient had surgery, or within 30 days from discharge for the non-operative patients. You will see that we are capturing diagnostic, interventional, and therapeutic data that extend beyond what is typically captured for MSQC patients. -

Small Bowel Obstruction Following Appendectomy: a Retrospective Study
New Indian Journal of Surgery21 Original Article January - March 2012, Volume 3 Number 1 Small Bowel Obstruction Following Appendectomy: A Retrospective Study Jyothi S Karegoudar*, Prabhakar PJ**, Rajashri S Patil***, VIjayanath V**** *Asso. Prof in General Surgery, ** Prof & HOD in General Surgery, ***Asst. Prof (biostatistician), S. S. I. M. S & R. C., Davangere, Karnataka State, ****MD, DNB, MNAMS, Associate Professor, Department of Forensic Medicine & Toxicology, Vinayaka Mission’s Kirupananda Variyar Medical College & Hospital, Salem,Tamil Nadu, India. Abstract appendectomy adhesive small bowel The incidence of post-operative small bowel obstruction occurs in 1 to 1.5% of all patients obstruction after standard, open appendectomy was within 14 years of the operation.[1] calculated during five year duration at S. S. Institute Appendectomy is one of the most frequently and Research Centre, Davangere, Karnataka State. performed emergency surgery, and it is Post-operative small bowel obstruction is one of associated with various short and long term the adverse effects of appendectomy but its frequency morbidities. Postoperative small bowel varies from centre to centre. The incidence of small obstruction is recognized as long term adverse bowel obstruction is significantly high in perforated effect of appendectomy.[2] appendicitis, midline incisions, and chronic appendicular pathology. The midline incision has The frequency of this complication is not increased the frequency of post-operative adhesions. well known but the reported risk ranges from This study was conducted to determine the 0.2- 10.7%.[3] The post-operative adhesions incidence of this complication among our patients are a significant problem after colorectal who had open appendectomy and identify the factors surgery.