A Case Report of Fibro-Stenotic Crohn's Disease in the Middle
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Inflammatory Bowel Disease Irritable Bowel Syndrome
Inflammatory Bowel Disease and Irritable Bowel Syndrome Similarities and Differences 2 www.ccfa.org IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 Important Differences Between IBD and IBS Many diseases and conditions can affect the gastrointestinal (GI) tract, which is part of the digestive system and includes the esophagus, stomach, small intestine and large intestine. These diseases and conditions include inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS). IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 www.ccfa.org 3 Inflammatory bowel diseases are a group of inflammatory conditions in which the body’s own immune system attacks parts of the digestive system. Inflammatory Bowel Disease Inflammatory bowel diseases are a group of inflamma- Causes tory conditions in which the body’s own immune system attacks parts of the digestive system. The two most com- The exact cause of IBD remains unknown. Researchers mon inflammatory bowel diseases are Crohn’s disease believe that a combination of four factors lead to IBD: a (CD) and ulcerative colitis (UC). IBD affects as many as 1.4 genetic component, an environmental trigger, an imbal- million Americans, most of whom are diagnosed before ance of intestinal bacteria and an inappropriate reaction age 35. There is no cure for IBD but there are treatments to from the immune system. Immune cells normally protect reduce and control the symptoms of the disease. the body from infection, but in people with IBD, the immune system mistakes harmless substances in the CD and UC cause chronic inflammation of the GI tract. CD intestine for foreign substances and launches an attack, can affect any part of the GI tract, but frequently affects the resulting in inflammation. -

Adult Intussusception
1 Adult Intussusception Saulius Paskauskas and Dainius Pavalkis Lithuanian University of Health Sciences Kaunas Lithuania 1. Introduction Intussusception is defined as the invagination of one segment of the gastrointestinal tract and its mesentery (intussusceptum) into the lumen of an adjacent distal segment of the gastrointestinal tract (intussuscipiens). Sliding within the bowel is propelled by intestinal peristalsis and may lead to intestinal obstruction and ischemia. Adult intussusception is a rare condition wich can occur in any site of gastrointestinal tract from stomach to rectum. It represents only about 5% of all intussusceptions (Agha, 1986) and causes 1-5% of all cases of intestinal obstructions (Begos et al., 1997; Eisen et al., 1999). Intussusception accounts for 0.003–0.02% of all hospital admissions (Weilbaecher et al., 1971). The mean age for intussusception in adults is 50 years, and and the male-to-female ratio is 1:1.3 (Rathore et. al., 2006). The child to adult ratio is more than 20:1. The condition is found in less than 1 in 1300 abdominal operations and 1 in 100 patients operated for intestinal obstruction. Intussusception in adults occurs less frequently in the colon than in the small bowel (Zubaidi et al., 2006; Wang et al., 2007). Mortality for adult intussusceptions increases from 8.7% for the benign lesions to 52.4% for the malignant variety (Azar & Berger, 1997) 2. Etiology of adult intussusception Unlike children where most cases are idiopathic, intussusception in adults has an identifiable etiology in 80- 90% of cases. The etiology of intussusception of the stomach, small bowel and the colon is quite different (Table 1). -
Recognizing-Consitpation-And-Bowel
Hughes Melton, MD Post Office Box 1797 Commissioner Richmond, Virginia 23218-1797 Office of Integrated Health Health & Safety Information Dr. Dawn M. Adams DNP, ANP-BC, CHC Director, Office of Integrated Health Recognizing Constipation & Preventing Bowel Obstruction 2018 Recognizing Constipation Constipation is a disorder that occurs when bowel movements become difficult or less frequent is frequently seen in many people. Individuals with developmental disabilities often have problems with chronic constipation as a result of but not limited to: Medication side effects Neuromuscular problems related to the person's disability Signs of Constipation small infrequent bowel movements hemorrhoids due to straining with bowel movements increased abdominal girth abdominal pain Chronic constipation Chronic constipation must be addressed in all individuals. This can often be a silent problem, especially for individuals who are independent in toileting activities. Without treatment, chronic constipation can lead to bowel obstruction, bowel perforation and death. Bowel Obstruction (Intestinal Obstruction) A partial or complete block of the small or large intestine that keeps food, liquid, gas, and stool from moving through the intestines in a normal way. October 2018 Hughes Melton, MD Post Office Box 1797 Commissioner Richmond, Virginia 23218-1797 Bowel obstructions may be caused by a twist in the intestines. Intestines are called the gut. The large intestine includes the appendix, cecum, colon, and rectum and is 5 feet long. It absorbs water from stool and changes it from a liquid to a solid form. The small intestine is where most digestion occurs. It measures about 20 feet and includes the duodenum, jejunum, and ileum. o Digestion is the process of breaking down food into substances the body can use for energy, tissue growth, and repair. -

Patient Selection Criteria
M∙ACS MACS Patient Selection Criteria The objective is to screen, on a daily basis, the Acute Care Surgical service “touches” at your hospital to identify patients who meet criteria for further data entry. The specific patient diseases/conditions that we are interested in capturing for emergent general surgery (EGS) are: 1. Acute Appendicitis 2. Acute Gallbladder Disease a. Acute Cholecystitis b. Choledocholithiasis c. Cholangitis d. Gallstone Pancreatitis 3. Small Bowel Obstruction a. Adhesive b. Hernia 4. Emergent Exploratory Laparotomy (Refer to the ex-lap algorithm under the Diseases or Conditions section below for inclusion/exclusion criteria.) The daily census for patients admitted to the Acute Care Surgery Service or seen as a consult will have to be screened. There may be other sources to accomplish this screening such as IT and we are interested in learning about these sources from you. From this census, a list can be compiled of patients with the aforementioned diseases/conditions. The first level of data entry involves capture and entry of the patient into the MACS Qualtrics database. All patients with the identified diseases/conditions will have data entered regardless of whether or not they received an operation during admission/ED visit. The second level of data entry takes place if an existing MACS patient returns to the hospital (ED or admission) or has outcome events identified within the 30-day post-operative time frame if the patient had surgery, or within 30 days from discharge for the non-operative patients. You will see that we are capturing diagnostic, interventional, and therapeutic data that extend beyond what is typically captured for MSQC patients. -

Small Bowel Obstruction Following Appendectomy: a Retrospective Study
New Indian Journal of Surgery21 Original Article January - March 2012, Volume 3 Number 1 Small Bowel Obstruction Following Appendectomy: A Retrospective Study Jyothi S Karegoudar*, Prabhakar PJ**, Rajashri S Patil***, VIjayanath V**** *Asso. Prof in General Surgery, ** Prof & HOD in General Surgery, ***Asst. Prof (biostatistician), S. S. I. M. S & R. C., Davangere, Karnataka State, ****MD, DNB, MNAMS, Associate Professor, Department of Forensic Medicine & Toxicology, Vinayaka Mission’s Kirupananda Variyar Medical College & Hospital, Salem,Tamil Nadu, India. Abstract appendectomy adhesive small bowel The incidence of post-operative small bowel obstruction occurs in 1 to 1.5% of all patients obstruction after standard, open appendectomy was within 14 years of the operation.[1] calculated during five year duration at S. S. Institute Appendectomy is one of the most frequently and Research Centre, Davangere, Karnataka State. performed emergency surgery, and it is Post-operative small bowel obstruction is one of associated with various short and long term the adverse effects of appendectomy but its frequency morbidities. Postoperative small bowel varies from centre to centre. The incidence of small obstruction is recognized as long term adverse bowel obstruction is significantly high in perforated effect of appendectomy.[2] appendicitis, midline incisions, and chronic appendicular pathology. The midline incision has The frequency of this complication is not increased the frequency of post-operative adhesions. well known but the reported risk ranges from This study was conducted to determine the 0.2- 10.7%.[3] The post-operative adhesions incidence of this complication among our patients are a significant problem after colorectal who had open appendectomy and identify the factors surgery. -

Colonic Ischemia 9/21/14, 9:02 PM
Colonic ischemia 9/21/14, 9:02 PM Official reprint from UpToDate® www.uptodate.com ©2014 UpToDate® Colonic ischemia Authors Section Editors Deputy Editor Peter Grubel, MD John F Eidt, MD Kathryn A Collins, MD, PhD, FACS J Thomas Lamont, MD Joseph L Mills, Sr, MD Martin Weiser, MD All topics are updated as new evidence becomes available and our peer review process is complete. Literature review current through: Aug 2014. | This topic last updated: Aug 25, 2014. INTRODUCTION — Intestinal ischemia is caused by a reduction in blood flow, which can be related to acute arterial occlusion (embolic, thrombotic), venous thrombosis, or hypoperfusion of the mesenteric vasculature causing nonocclusive ischemia. Colonic ischemia is the most frequent form of intestinal ischemia, most often affecting the elderly [1]. Approximately 15 percent of patients with colonic ischemia develop gangrene, the consequences of which can be life-threatening, making rapid diagnosis and treatment imperative. The remainder develops nongangrenous ischemia, which is usually transient and resolves without sequelae [2]. However, some of these patients will have a more prolonged course or develop long-term complications, such as stricture or chronic ischemic colitis. The diagnosis and treatment of patients can be challenging since colonic ischemia often occurs in patients who are debilitated and have multiple medical problems. The clinical features, diagnosis, and treatment of ischemia affecting the colon and rectum will be reviewed here. Acute and chronic intestinal ischemia of the small intestine are discussed separately. (See "Acute mesenteric ischemia" and "Chronic mesenteric ischemia".) BLOOD SUPPLY OF THE COLON — The circulation to the large intestine and rectum is derived from the superior mesenteric artery (SMA), inferior mesenteric artery (IMA), and internal iliac arteries (figure 1). -

Assessment of Small Bowel Obstruction in Patients Following Appendicitis: an Institutional Based Study
Original Research Article. Assessment of Small Bowel Obstruction in Patients Following Appendicitis: An Institutional Based Study Atahussain Poonawala1, Nilofer Poonawala2* 1Assistant Professor, Department of General Surgery, Vedantaa Institute of Medical Sciences, Palghar, Maharashtra, India. 2Assistant Professor, Department of Obstetrics and Gynaecology, Vedantaa Institute of Medical Sciences, Palghar, Maharashtra, India. ABSTRACT Background: Small bowel obstruction (SBO) is a pathological may be seen in few cases of appendectomy. condition which occurs when the intestinal contents are prevented from moving along the length of the intestine. The Key words: Appendectomy, Phlegmonous, Small Bowel present study was conducted to assess the cases of small Obstruction. bowel obstruction following appendectomy. *Correspondence to: Materials & Methods: The present study was conducted on Dr. Nilofer Poonawala, 42 cases of appendicitis of both genders. In all patients, Assistant Professor, laparoscopic appendectomy was planned. Patients were Department of Obstetrics and Gynaecology, recalled to note any kind of complication arising from the Vedantaa Institute of Medical Sciences, procedure. Palghar, Maharashtra, India. Results: Out of 42 patients, males were 26 and females were Article History: 16. Age group 20-30 years had 5 males and 3 females, 30-40 Received: 28-11-2019, Revised: 25-12-2019, Accepted: 21-01-2020 years had 9 males and 5 females and 40-50 years had 12 Access this article online males and 8 females. The difference was significant (P< 0.05). Website: Quick Response code Macroscopic feature of appendix during procedure was www.ijmrp.com phlegmonous in 12 and gangrenous in 30 cases. The DOI: difference was significant (P< 0.05). 10.21276/ijmrp.2020.6.1.016 Conclusion: Small bowel obstruction is a complication which INTRODUCTION Appendectomy is one of the most common procedures performed Intestinal obstruction is most commonly caused by intra- which may be due to appendicitis or frequent pain in appendix. -
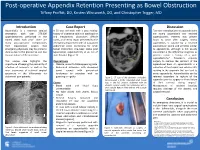
Introduction Discussion Conclusion Case Report
Post-operative Appendix Retention Presenting as Bowel Obstruction Tiffany Proffitt, DO, Kristen Whitworth, DO, and Christopher Trigger, MD Introduction Case Report Discussion Appendicitis is a common surgical A 50 year old male with a past medical Two rare complications of appendectomy emergency with over 270,000 history of ulcerative colitis on azathioprine are stump appendicitis and retained appendectomies performed in the and mesalamine, clostridium difficile appendicoliths. Patients may present United States each year.1 There are colitis, and hernia repair presented to the hours to years after surgery. Stump many post-operative complications emergency department with an outpatient appendicitis is caused by a retained from laparoscopic surgery that abdominal series concerning for small appendicular stump and presents similar emergency physicians may be prone to bowel obstruction one-week status post to appendicitis, although is not usually dismiss due to the prevalence and less laparoscopic appendectomy at an out of considered in the differential diagnosis as invasive nature of the procedure. state hospital (Figure 1). patients report a history of a prior appendectomy.2 Treatment requires This unique case highlights the Physical Exam surgery to remove the remnant of the importance of keeping the possibility of • Afebrile, uncomfortable appearing male appendiceal base. An appendicolith is a infection of remnants as well as the • Abdominal distension with decreased collection of fecal debris and calcium salts rarer occurrence of retained surgical bowel sounds with generalized residing in the appendix that can lead to specimens in the differentials for tenderness to palpation with no acute appendicitis. Appendicoliths can be abdominal pain patients. guarding or rigidity Figure 2. -

Gastric Outlet Obstruction in a Patient with Bouveret's
Nabais et al. BMC Research Notes 2013, 6:195 http://www.biomedcentral.com/1756-0500/6/195 CASE REPORT Open Access Gastric outlet obstruction in a patient with Bouveret’s syndrome: a case report Celso Nabais*, Raquel Salústio, Inês Morujão, Francisco V Sousa, Eusébio Porto, Carlos Cardoso and Caldeira Fradique Abstract Background: Gallstone ileus accounts for 1% to 4% of cases of mechanical bowel obstruction, but may be responsible for up to 25% of cases in older age groups. In non-iatrogenic cases, gallstone migration occurs after formation of a biliary-enteric fistula. In fewer than 10% of patients with gallstone ileus, the impacted gallstones are located in the pylorus or duodenum, resulting in gastric outlet obstruction, known as Bouveret’s syndrome. Case presentation: We report an 86-year-old female who was admitted to hospital with a 10-day history of persistent vomiting and prostration. She was in hypovolemic shock at the time of arrival in the emergency department. Investigations revealed a gallstone in the duodenal bulb and a cholecystoduodenal fistula. She underwent surgical gastrolithotomy. Unfortunately, she died of aspiration pneumonia on the fourth postoperative day. Conclusion: This case shows the importance of considering Bouveret’s syndrome in the differential diagnosis of gastric outlet obstruction, especially in the elderly, even in patients with no previous history of gallbladder disease. Keywords: Bouveret’s syndrome, Gallstone ileus, Gastric outlet obstruction, Cholecystoduodenal fistula Background syndrome in which other comorbidities added to the Gallstone ileus is a rare complication of gallstone diagnostic challenge. disease, causing 1% to 4% of cases of mechanical bowel obstruction. -

Tracy Aldridge, MD Constipation Bowel Obstruction
11/18/2013 Tracy Aldridge, MD Constipation ◦ Occasional- episode of constipation which resolves easily from time to time. Everyone has occasional constipation. ◦ Chronic- requiring treatment with medications to control symptoms and maintain regular bowel movements. Bowel Obstruction ◦ Small Bowel Obstruction ◦ Large Bowel Obstruction 1 11/18/2013 Small intestine ◦ (also called the small bowel) Large intestine ◦ (also called the large bowel, or colon) Constipation is defined as having a bowel movement fewer than three times per week. Stools are usually hard, dry, small in size, and difficult to eliminate. Normal bowel function can range from three times a day or three times a week, depending on the person. 2 11/18/2013 Developmental disabilities ◦ Less active, poor dietary fiber, less fluid intake Neuromuscular disorders ◦ Abnormal nerve and muscle response or coordination in the bowel Cerebral palsy ◦ Poor nerve responses within the bowel causing motility problems Medication side effects ◦ Slowing of the transit time or alteration of bowel consistency or fluid content Spending a lot of time on the toilet Stra ining a nd g ru nt ing while pass ing stoo l Hard, small, dry feces Bloating and complaints of stomach discomfort Engages in rectal digging 3 11/18/2013 Conservative and/or preventive measures ◦ Increase fluid intake if able ◦ Increase fiber intake ◦ Increase physical activity Laxative medications ◦ Stimulants (such as senna, docusate) These help stimulate the intestine to move food and fluid through. ◦ Stool softeners (colace) Increase the liquid content of the stool to make it easier to pass ◦ Lubricant laxatives (mineral oil) ◦ Osmot ic agents (suc h as Milk of M agnesi a, Mira lax) These act like a sponge, drawing fluid into the bowel to help with elimination. -

Recurrent Large Bowel Obstruction Caused by Necrotizing Pancreatitis: a Rare Manifestation
Open Access Case Report DOI: 10.7759/cureus.12307 Recurrent Large Bowel Obstruction Caused by Necrotizing Pancreatitis: A Rare Manifestation Mehak Bassi 1 , Anjali Desai 2 , C.S. Pitchumoni 3 1. Internal Medicine, Saint Peter's University Hospital, New Brunswick, USA 2. Medicine, Robert Wood Johnson University Hospital, New Brunswick, USA 3. Gastroenterology and Hepatology, Saint Peter’s University Hospital, New Brunswick, USA Corresponding author: Mehak Bassi, [email protected] Abstract Mechanical obstruction of the colon is rare with necrotizing pancreatitis but is associated with high morbidity and mortality. However, pancreatic ileus, colonic necrosis, and pancreatic colonic fistulae with necrotizing pancreatitis are well known. The anatomic proximity of the pancreas to the transverse colon becomes clinically relevant when a patient with pancreatitis demonstrates a localized ileus of the transverse colon (an old term “the colon cut-off sign”), even when the disease is mild, or lower gastrointestinal bleeding secondary to necrosis of the segment in severe acute pancreatitis. We present the case of a 25- year-old female with choledocholithiasis who presented with severe abdominal pain and was found to have recurrent large bowel obstruction secondary to walled-off pancreatic necrosis. Bowel obstruction is a rare complication of walled-off necrosis, but clinicians should be aware of it due to significantly increased mortality rates. Recurrent bowel obstructions are rarely known in necrotizing pancreatitis and may warrant a bowel resection either electively or acutely. Walled-off necrosis does not respond to typical treatment of symptomatic pseudocysts, which includes endoscopic cystogastrostomy or percutaneous drainage with small-bore catheters. Endoscopic or surgical necrosectomy is necessary for the resolution of walled-off necrosis to evacuate the non-liquefied components. -

Stone Ileus: an Unusual Presentation of Crohn's Disease
Ma, et al. Int J Surg Res Pract 2016, 3:046 International Journal of Volume 3 | Issue 2 ISSN: 2378-3397 Surgery Research and Practice Case Report: Open Access Stone Ileus: An Unusual Presentation of Crohn’s Disease Charles Ma and H Tracy Davido Department of Critical Care and Acute Care Surgery, University of Minnesota Health, USA *Corresponding author: H Tracy Davido MD, Assistant Professor of Surgery, Department of Critical Care and Acute Care Surgery, University of Minnesota Health, 11-115A Phillips Wangensteen Building, 420 Delaware St. SE, MMC 195, Minneapolis, MN 55455, USA, Tel: 612-626-6441, E-mail: [email protected] Introduction Case Report Stone ileus, also known as enterolith ileus enterolithiaisis, is a rare A 67-year-old morbidly obese woman came to the emergency complication of cholelithiasis and an even rarer symptom of Crohn’s department at our institution with an upper respiratory infection, disease. Gallstone ileus is secondary to fistula formation between decreased appetite, and malaise. Her past medical history was the gallbladder and the gastrointestinal (GI) system. Enterolithiasis significant for an open cholecystectomy more than 30 years earlier. of Crohn’s disease is thought to arise from the stasis of succus She had no additional past surgical history or diagnoses. The initial within the small bowel eventually leading to stone formation and workup revealed acute renal failure, with significant electrolyte growth. Both gallstone ileus and enterolithiasis of Crohn’s disease abnormalities and dehydration. She underwent intravenous fluid can result in subsequent mechanical bowel obstruction. Gallstone resuscitation and electrolyte replacement in the Medical Intensive ileus accounts for 1% to 4% of mechanical bowel obstructions, with Care Unit; however, while hospitalized, she developed new-onset higher a incidence in women over age 60 [1].