ACS/ASE Medical Student Core Curriculum: Vomiting, Diarrhea, And
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Adult Congenital Megacolon with Acute Fecal Obstruction and Diabetic Nephropathy: a Case Report
2726 EXPERIMENTAL AND THERAPEUTIC MEDICINE 18: 2726-2730, 2019 Adult congenital megacolon with acute fecal obstruction and diabetic nephropathy: A case report MINGYUAN ZHANG1,2 and KEFENG DING1 1Colorectal Surgery Department, Second Affiliated Hospital, School of Medicine, Zhejiang University, Hangzhou, Zhejiang 310000; 2Department of Gastrointestinal Surgery, Yinzhou Peoples' Hospital, Ningbo, Zhejiang 315000, P.R. China Received November 27, 2018; Accepted June 20, 2019 DOI: 10.3892/etm.2019.7852 Abstract. Megacolon is a congenital disorder. Adult congen- sufficient amount of bowel should be removed, particularly the ital megacolon (ACM), also known as adult Hirschsprung's aganglionic segment (2). The present study reports on a case of disease, is rare and frequently manifests as constipation. ACM a 56-year-old patient with ACM, fecal impaction and diabetic is caused by the absence of ganglion cells in the submucosa nephropathy. or myenteric plexus of the bowel. Most patients undergo treat- ment of megacolon at a young age, but certain patients cannot Case report be treated until they develop bowel obstruction in adulthood. Bowel obstruction in adults always occurs in complex clinical A 56-year-old male patient with a history of chronic constipa- situations and it is frequently combined with comorbidities, tion presented to the emergency department of Yinzhou including bowel tumors, volvulus, hernias, hypertension or Peoples' Hospital (Ningbo, China) in February 2018. The diabetes mellitus. Surgical intervention is always required in patient had experienced vague abdominal distention for such cases. To avoid recurrence, a sufficient amount of bowel several days. Prior to admission, chronic bowel obstruction should be removed, particularly the aganglionic segment. -

Inflammatory Bowel Disease Irritable Bowel Syndrome
Inflammatory Bowel Disease and Irritable Bowel Syndrome Similarities and Differences 2 www.ccfa.org IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 Important Differences Between IBD and IBS Many diseases and conditions can affect the gastrointestinal (GI) tract, which is part of the digestive system and includes the esophagus, stomach, small intestine and large intestine. These diseases and conditions include inflammatory bowel disease (IBD) and irritable bowel syndrome (IBS). IBD Help Center: 888.MY.GUT.PAIN 888.694.8872 www.ccfa.org 3 Inflammatory bowel diseases are a group of inflammatory conditions in which the body’s own immune system attacks parts of the digestive system. Inflammatory Bowel Disease Inflammatory bowel diseases are a group of inflamma- Causes tory conditions in which the body’s own immune system attacks parts of the digestive system. The two most com- The exact cause of IBD remains unknown. Researchers mon inflammatory bowel diseases are Crohn’s disease believe that a combination of four factors lead to IBD: a (CD) and ulcerative colitis (UC). IBD affects as many as 1.4 genetic component, an environmental trigger, an imbal- million Americans, most of whom are diagnosed before ance of intestinal bacteria and an inappropriate reaction age 35. There is no cure for IBD but there are treatments to from the immune system. Immune cells normally protect reduce and control the symptoms of the disease. the body from infection, but in people with IBD, the immune system mistakes harmless substances in the CD and UC cause chronic inflammation of the GI tract. CD intestine for foreign substances and launches an attack, can affect any part of the GI tract, but frequently affects the resulting in inflammation. -

The American Society of Colon and Rectal Surgeons' Clinical Practice
CLINICAL PRACTICE GUIDELINES The American Society of Colon and Rectal Surgeons’ Clinical Practice Guideline for the Evaluation and Management of Constipation Ian M. Paquette, M.D. • Madhulika Varma, M.D. • Charles Ternent, M.D. Genevieve Melton-Meaux, M.D. • Janice F. Rafferty, M.D. • Daniel Feingold, M.D. Scott R. Steele, M.D. he American Society of Colon and Rectal Surgeons for functional constipation include at least 2 of the fol- is dedicated to assuring high-quality patient care lowing symptoms during ≥25% of defecations: straining, Tby advancing the science, prevention, and manage- lumpy or hard stools, sensation of incomplete evacuation, ment of disorders and diseases of the colon, rectum, and sensation of anorectal obstruction or blockage, relying on anus. The Clinical Practice Guidelines Committee is com- manual maneuvers to promote defecation, and having less posed of Society members who are chosen because they than 3 unassisted bowel movements per week.7,8 These cri- XXX have demonstrated expertise in the specialty of colon and teria include constipation related to the 3 common sub- rectal surgery. This committee was created to lead inter- types: colonic inertia or slow transit constipation, normal national efforts in defining quality care for conditions re- transit constipation, and pelvic floor or defecation dys- lated to the colon, rectum, and anus. This is accompanied function. However, in reality, many patients demonstrate by developing Clinical Practice Guidelines based on the symptoms attributable to more than 1 constipation sub- best available evidence. These guidelines are inclusive and type and to constipation-predominant IBS, as well. The not prescriptive. -

PYLORIC STENOSIS of INFANCY-PERSPECTIVES Different Views from Different Bridges
Central Annals of Pediatrics & Child Health Perspective *Corresponding author IAN M. ROGERS, Department of Surgery, AIMST University, 46 Whitburn Road, Cleadon, Tyne and Wear, SR67QS, Kedah, Malaysia, Tel: 01915367944; PYLORIC STENOSIS OF INFANCY- 07772967160; Email: [email protected] Submitted: 18 March 2020 PERSPECTIVES Different views Accepted: 27 March 2020 Published: 30 March 2020 ISSN: 2373-9312 from different bridges Copyright © 2020 ROGERS IM IAN M ROGERS* OPEN ACCESS Department of Surgery, AIMST University, Malaysia Keywords Abstract • Neonatal hyperacidity; Neonatal hypergastrinaemia; Baby and parents perspectives of diagnosis Introduction: The differing experiences of the surgeon, he parent and the baby and treatment; Spectrum of presentation of are discussed in terms of what is presently known about the pathogenesis of pyloric pyloric stenosis of infancy; Primary hyperacidity stenosis of infancy (PS). pathogenesis of pyloric stenosis Methods: The experiences are culled from personal experience and from the comments made on online pressure and support groups for pyloric stenosis of infancy. These comments are reviewed from the standpoint of the Primary Hyperacidity pathogenesis of cause. Conclusion: The present perspectives of the PS surgeon and the difficulties experienced by the PS family fit well which the basic tenets of the Primary Hyperacidity theory. Reference to this theory allows a satisfactory explanation for difficulties in diagnosis and for the variability of presentation. INTRODUCTION In 1961 this theme was further developed by Dr Jacob. He again recognised the milder forms-those in which a long- term The Surgeon cure could similarly be achieved without surgery. A 1% mortality Everybody knows: For progressive pyloric stenosis of infancy in 100 patients was achieved with the usual medical measures (PS), pyloromyotomy reigns supreme! Impending catastrophe of which a reduced feeding regime was judged to be especially transformed safely, in a few minutes, into an enduring cure. -

A Case Report of Fibro-Stenotic Crohn's Disease in the Middle
DOI: https://doi.org/10.22516/25007440.185 Case report A Case Report of Fibro-Stenotic Crohn’s Disease in the Middle Ileum as the Initial Manifestation Adriana Margarita Rey,1 Gustavo Reyes,1 Fernando Sierra,1 Rafael García-Duperly,2 Rocío López,3 Leidy Paola Prada.4 1 Gastroenterologist in the Gastroenterology and Abstract Hepatology Service of the Hospital Universitario Fundación Santa Fe de Bogotá in Bogotá, Colombia Crohn’s disease (CD) is an inflammatory bowel disease that can affect the entire gastrointestinal tract. The small 2 Colon and Rectum Surgeon in the Department of intestine is affected in about 50% of patients among whom the terminal ileum is the area most commonly affected. Surgery of the Hospital Universitario Fundación Intestinal stenosis is a common complication in CD and approximately 30% to 50% of patients present Santa Fe de Bogotá in Bogotá, Colombia 3 Pathologist at of the Hospital Universitario Fundación stenosis or penetrating lesions at the time of diagnosis. Because conventional endoscopic techniques do not Santa Fe de Bogotá and Professor at Universidad de allow evaluation of small bowel lesions, techniques such as enteroscopy and endoscopic video-capsule were los Andes in Bogotá, Colombia developed. Each has advantages and indications. 4 Third Year Internal Medicine Resident at the Hospital Universitario Fundación Santa Fe de Bogotá in We present the case of a patient with CD with localized fibrostenosis in the middle ileum which is not a Bogotá, Colombia frequent site for this type of lesion. Author for correspondence: Adriana Margarita Rey. Bogotá D.C. Colombia [email protected] Keywords ........................................ -

Delayed Presentation of a Retained Fecalith
Open Access Case Report DOI: 10.7759/cureus.15919 Delayed Presentation of a Retained Fecalith Fawwad A. Ansari 1 , Muhammad Ibraiz Bilal 1 , Muhammad Umer Riaz Gondal 1 , Mehwish Latif 2 , Nadeem Iqbal 2 1. Medicine, Shifa International Hospital, Islamabad, PAK 2. Gastroenterology, Shifa International Hospital, Islamabad, PAK Corresponding author: Fawwad A. Ansari, [email protected] Abstract A fecalith is a common cause of acute appendicitis, and laparoscopic surgery is the mainstay of its management. Literature review shows that a fecalith may be retained in the gut following a laparoscopic appendectomy in some rare cases. In most cases, the fecalith becomes symptomatic with time due to the formation of an abscess, fistulous tract, or inflammation of the appendicular stump (stump appendicitis). We report a case of retained appendicular fecalith presenting with symptoms similar to acute appendicitis, 15 years after laparoscopic appendectomy. Categories: Gastroenterology, General Surgery Keywords: colonoscopy, acute appendicitis, appendectomy, fecalith, right iliac fossa pain, complications Introduction A fecalith is a hard stony mass of feces in the intestinal tract. Fecal impaction occurs when a large amount of fecal matter gets compacted and cannot get evacuated spontaneously [1]. In its extreme form, fecal impaction can lead to the formation of a fecalith due to the hardening of fecal material that forms a mass separate from other bowel contents [2]. It can occur in any part of the intestine [1]. Most often, a fecalith arises in the colon (mostly sigmoid) or rectum and very rarely in the small intestine [2]. Here we present a case of a retained appendicular fecalith in a patient who presented with an acute abdomen. -

Gastroenterology and the Elderly
3 Gastroenterology and the Elderly Thomas W. Sheehy 3.1. Esophagus 3.1.1. Dysphagia Esophageal disorders, such as esophageal motility disorders, infections, tumors, and other diseases, are common in the elderly. In the elderly, dysphagia usually implies organic disease. There are two types: (1) pre-esophageal and (2) esophageal. Both are further subdivided into motor (neuromuscular) or structural (intrinsic and extrinsic) lesions.! 3.1.2. Pre-esophageal Dysphagia Pre-esophageal dysphagia (PED) usually implies neuromuscular disease and may be caused by pseudobular palsy, multiple sclerosis, amy trophic lateral scle rosis, Parkinson's disease, bulbar poliomyelitis, lesions of the glossopharyngeal nerve, myasthenia gravis, and muscular dystrophies. Since PED is due to inability to initiate the swallowing mechanism, food cannot escape from the oropharynx into the esophagus. Such patients usually have more difficulty swallowing liquid THOMAS W. SHEEHY • The University of Alabama in Birmingham, School of Medicine, Department of Medicine; and Medical Services, Veterans Administration Medical Center, Birming ham, Alabama 35233. 87 S. R. Gambert (ed.), Contemporary Geriatric Medicine © Plenum Publishing Corporation 1983 88 THOMAS W. SHEEHY than solids. They sputter or cough during attempts to swallow and often have nasal regurgitation or aspiration of food. 3.1.3. Dysfunction of the Cricopharyngeus Muscle In the elderly, this is one of the more common forms of PED.2 These patients have the sensation of an obstruction in their throat when they attempt to swallow. This is due to incoordination of the cricopharyngeus muscle. When this muscle fails to relax quickly enough during swallowing, food cannot pass freely into the esophagus. If the muscle relaxes promptly but closes too quickly, food is trapped as it attempts to enter the esophagus. -

Adult Intussusception
1 Adult Intussusception Saulius Paskauskas and Dainius Pavalkis Lithuanian University of Health Sciences Kaunas Lithuania 1. Introduction Intussusception is defined as the invagination of one segment of the gastrointestinal tract and its mesentery (intussusceptum) into the lumen of an adjacent distal segment of the gastrointestinal tract (intussuscipiens). Sliding within the bowel is propelled by intestinal peristalsis and may lead to intestinal obstruction and ischemia. Adult intussusception is a rare condition wich can occur in any site of gastrointestinal tract from stomach to rectum. It represents only about 5% of all intussusceptions (Agha, 1986) and causes 1-5% of all cases of intestinal obstructions (Begos et al., 1997; Eisen et al., 1999). Intussusception accounts for 0.003–0.02% of all hospital admissions (Weilbaecher et al., 1971). The mean age for intussusception in adults is 50 years, and and the male-to-female ratio is 1:1.3 (Rathore et. al., 2006). The child to adult ratio is more than 20:1. The condition is found in less than 1 in 1300 abdominal operations and 1 in 100 patients operated for intestinal obstruction. Intussusception in adults occurs less frequently in the colon than in the small bowel (Zubaidi et al., 2006; Wang et al., 2007). Mortality for adult intussusceptions increases from 8.7% for the benign lesions to 52.4% for the malignant variety (Azar & Berger, 1997) 2. Etiology of adult intussusception Unlike children where most cases are idiopathic, intussusception in adults has an identifiable etiology in 80- 90% of cases. The etiology of intussusception of the stomach, small bowel and the colon is quite different (Table 1). -

An Osteopathic Approach to Gastrointestinal Disease
REVIEW An Osteopathic Approach to Gastrointestinal Disease: Somatic Clues for Diagnosis and Clinical Challenges Associated With Helicobacter pylori Antibiotic Resistance Alicia Smilowicz, DO From HealthCalls LLC The estimated prevalence of gastritis in the general US population is approxi- in Portland, Maine, and mately 50%. Patients with gastrointestinal disease often present to the primary the University of New England College of care practitioner with dyspepsia and abdominal pain. Osteopathic palpatory Osteopathic Medicine in evaluation suggests that there is an association among gastrointestinal dis- Biddeford, Maine. ease, the presence of posterior midthoracic pain, and chronic headache. On Financial Disclosures: the basis of findings from a review of the literature, the author assesses the po- None reported. tential etiologic mechanisms of this clinical association. Possible mechanisms Address correspondence to include the physiologic function of the vagus nerve, a neural convergence Alicia Smilowicz, DO, 466 Ocean Ave, Portland, model, and the inherent properties of Helicobacter pylori. To demonstrate the ME 04103-5718. clinical significance of these mechanisms, the author presents the case of a E-mail: docsmilo 30-year-old woman with headache, thoracic discomfort, and gastritis associ- @yahoo.com ated with H pylori infection. The author suggests that successful treatment of Received August 2, 2012; patients with gastrointestinal disease includes osteopathic manipulative treat- revision received November 21, 2012; ment, behavioral modification, and pharmacotherapy, even when challenged accepted by antibiotic resistance. January 6, 2013. J Am Osteopath Assoc. 2013;113(5):404-416 n the practice of clinical medicine, we commonly associate dyspepsia, abdominal pain, nausea, and anorexia with the possible existence of pathologic mechanisms for gastro- Iintestinal disease. -

Dilation and Adjunct Therapy for Strictures
Review Article Page 1 of 6 Dilation and adjunct therapy for strictures Richard Johnson, Eleanor C. Fung Department of Surgery, University at Buffalo Jacobs School of Medicine and Biomedical Sciences, Buffalo, NY, USA Contributions: (I) Conception and design: All authors; (II) Administrative support: None; (III) Provision of study materials or patients: None; (IV) Collection and assembly of data: All authors; (V) Data analysis and interpretation: All authors; (VI) Manuscript writing: All authors; (VII) Final approval of manuscript: All authors. Correspondence to: Eleanor C. Fung. 462 Grider Street, DK Miller Building 3rd Floor, Buffalo, NY 14215, USA. Email: [email protected]. Abstract: Strictures within the gastrointestinal tract (GIT) are a common issue faced by clinicians and can occur from a variety of benign and malignant etiologies. The goal of treatment is luminal enlargement to improve obstructive symptoms such as nausea, vomiting, abdominal pain, obstipation or bowel obstruction. Generally, strictures can be effectively managed using endoscopic techniques of which dilation is generally the most commonly used and is effective in the management of strictures throughout the GIT. This review article will detail the current technologies available for the treatment of gastrointestinal strictures including indications of use, efficacy and safety. Keywords: Stricture; dilation; endoscopy; stent; electroincisional therapy Received: 01 April 2019; Accepted: 11 June 2019; Published: 01 July 2019. doi: 10.21037/ales.2019.06.06 View this article at: http://dx.doi.org/10.21037/ales.2019.06.06 Introduction Dilation Strictures can occur at any level of the gastrointestinal The earliest treatments were focused on the esophagus as tract (GIT) from the esophagus to the colon. -

Epstein–Barr Virus and Helicobacter Pylori Co-Infection in Non-Malignant Gastroduodenal Disorders
pathogens Review Epstein–Barr Virus and Helicobacter Pylori Co-Infection in Non-Malignant Gastroduodenal Disorders Ramsés Dávila-Collado 1, Oscar Jarquín-Durán 1, Le Thanh Dong 2 and J. Luis Espinoza 3,* 1 Faculty of Medicine, UNIDES University, Managua 11001, Nicaragua; [email protected] (R.D.-C.); [email protected] (O.J.-D.) 2 Faculty of Medical Technology, Hanoi Medical University, Hanoi 116001, Vietnam; [email protected] 3 Faculty of Health Sciences, Kanazawa University, Kodatsuno 5-11-80, Kanazawa 920-0942, Ishikawa, Japan * Correspondence: luis@staff.kanazawa-u.ac.jp Received: 20 January 2020; Accepted: 5 February 2020; Published: 6 February 2020 Abstract: Epstein–Barr virus (EBV) and Helicobacter pylori (H. pylori) are two pathogens associated with the development of various human cancers. The coexistence of both microorganisms in gastric cancer specimens has been increasingly reported, suggesting that crosstalk of both pathogens may be implicated in the carcinogenesis process. Considering that chronic inflammation is an initial step in the development of several cancers, including gastric cancer, we conducted a systematic review to comprehensively evaluate publications in which EBV and H. pylori co-infection has been documented in patients with non-malignant gastroduodenal disorders (NMGDs), including gastritis, peptic ulcer disease (PUD), and dyspepsia. We searched the PubMed database up to August 2019, as well as publication references and, among the nine studies that met the inclusion criteria, we identified six studies assessing EBV infection directly in gastric tissues (total 949 patients) and three studies in which EBV infection status was determined by serological methods (total 662 patients). -
Recognizing-Consitpation-And-Bowel
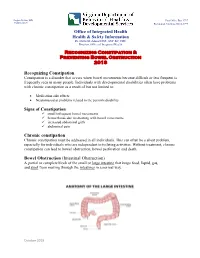
Hughes Melton, MD Post Office Box 1797 Commissioner Richmond, Virginia 23218-1797 Office of Integrated Health Health & Safety Information Dr. Dawn M. Adams DNP, ANP-BC, CHC Director, Office of Integrated Health Recognizing Constipation & Preventing Bowel Obstruction 2018 Recognizing Constipation Constipation is a disorder that occurs when bowel movements become difficult or less frequent is frequently seen in many people. Individuals with developmental disabilities often have problems with chronic constipation as a result of but not limited to: Medication side effects Neuromuscular problems related to the person's disability Signs of Constipation small infrequent bowel movements hemorrhoids due to straining with bowel movements increased abdominal girth abdominal pain Chronic constipation Chronic constipation must be addressed in all individuals. This can often be a silent problem, especially for individuals who are independent in toileting activities. Without treatment, chronic constipation can lead to bowel obstruction, bowel perforation and death. Bowel Obstruction (Intestinal Obstruction) A partial or complete block of the small or large intestine that keeps food, liquid, gas, and stool from moving through the intestines in a normal way. October 2018 Hughes Melton, MD Post Office Box 1797 Commissioner Richmond, Virginia 23218-1797 Bowel obstructions may be caused by a twist in the intestines. Intestines are called the gut. The large intestine includes the appendix, cecum, colon, and rectum and is 5 feet long. It absorbs water from stool and changes it from a liquid to a solid form. The small intestine is where most digestion occurs. It measures about 20 feet and includes the duodenum, jejunum, and ileum. o Digestion is the process of breaking down food into substances the body can use for energy, tissue growth, and repair.