Comparative Study on Nutritional Status of Primary Level School Children Studying in Private and Public Schools of Babiya Vdc, Sunsari
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Study Report on "Comminity Based Organizations(Cbos): Landscape
Community Based Organizations (CBOs): Landscape, Capacity Assessment and Strengthening Strategy Study Report Prepared for PLAN Nepal Lalitpur, Nepal July, 2005 Democratizing civil society at grassroots SAGUN P.O. Box 7802, Kathmandu, Nepal Phone: 977 4247920, Fax: 9771 4229544 Email: [email protected] Community Based Organizations (CBOs): Landscape, Capacity Assessment and Strengthening Strategy Mukta S. Lama Suresh Dhakal Lagan Rai Study Report Prepared for PLAN Nepal Lalitpur, Nepal July, 2005 SAGUN P.O. Box 7802, Kathmandu, Nepal Phone: 977 4247920, Fax: 9771 4229544 Email: [email protected] ii Acknowledgements This report is a result of contribution of many people in multiple ways. Foremost, we extend our deepest and heartfelt gratitude to members of Community Based Organizations across the districts for sharing us with their time, insight and experiences. The study benefited greatly from support and cooperation of the Plan field staff and partner agencies in Sunsari, Morang, Makwanpur, Rautahat, Bara, and Banke districts and the Regional Operational Support Unit teams. We would like to thank Ms. Chhing Lamu Sherpa, Mr. Kalbhan Rai, Dr. Chandra K. Sen, Mr. R. P. Gupta and Krishna Ghimire for their valuable inputs on the study. Dr. Chandi Chapagai, Plan Nepal Country Training Coordinator deserves special thanks for coordinating the whole exercise. We would like to express our deep appreciation to Shobhakar Vaidhya for his keen interest, insightful comments and his enthusiasm for incorporating the learning into the institutional policies and procedures. Thanks are also due to the Ms. Minty Pande, Country Director for her encouragement and comments. Similarly we very much appreciate the support of Mr. -

Food Insecurity and Undernutrition in Nepal
SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics SMALL AREA ESTIMATION OF FOOD INSECURITY AND UNDERNUTRITION IN NEPAL GOVERNMENT OF NEPAL National Planning Commission Secretariat Central Bureau of Statistics Acknowledgements The completion of both this and the earlier feasibility report follows extensive consultation with the National Planning Commission, Central Bureau of Statistics (CBS), World Food Programme (WFP), UNICEF, World Bank, and New ERA, together with members of the Statistics and Evidence for Policy, Planning and Results (SEPPR) working group from the International Development Partners Group (IDPG) and made up of people from Asian Development Bank (ADB), Department for International Development (DFID), United Nations Development Programme (UNDP), UNICEF and United States Agency for International Development (USAID), WFP, and the World Bank. WFP, UNICEF and the World Bank commissioned this research. The statistical analysis has been undertaken by Professor Stephen Haslett, Systemetrics Research Associates and Institute of Fundamental Sciences, Massey University, New Zealand and Associate Prof Geoffrey Jones, Dr. Maris Isidro and Alison Sefton of the Institute of Fundamental Sciences - Statistics, Massey University, New Zealand. We gratefully acknowledge the considerable assistance provided at all stages by the Central Bureau of Statistics. Special thanks to Bikash Bista, Rudra Suwal, Dilli Raj Joshi, Devendra Karanjit, Bed Dhakal, Lok Khatri and Pushpa Raj Paudel. See Appendix E for the full list of people consulted. First published: December 2014 Design and processed by: Print Communication, 4241355 ISBN: 978-9937-3000-976 Suggested citation: Haslett, S., Jones, G., Isidro, M., and Sefton, A. (2014) Small Area Estimation of Food Insecurity and Undernutrition in Nepal, Central Bureau of Statistics, National Planning Commissions Secretariat, World Food Programme, UNICEF and World Bank, Kathmandu, Nepal, December 2014. -
Existing Environmental Conditions
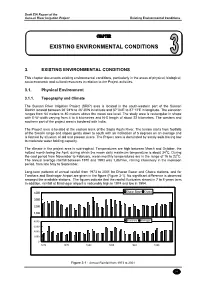
Draft EIA Report of the Sunsari River Irrigation Project Existing Environmental Conditions CHAPTER EXISTING ENVIRONMENTAL CONDITIONS 3. EXISTING ENVIRONMENTAL CONDITIONS This chapter documents existing environmental conditions, particularly in the areas of physical, biological, socio-economic and cultural resources in relation to the Project activities. 3.1. Physical Environment 3.1.1. Topography and Climate The Sunsari River Irrigation Project (SRIP) area is located in the south-western part of the Sunsari District located between 26°24′N to 26°30′N in latitude and 87°04′E to 87°12′E in longitude. The elevation ranges from 64 meters to 80 meters above the mean sea level. The study area is rectangular in shape with E-W width varying from 4 to 8 kilometres and N-S length of about 22 kilometres. The western and southern part of the project area is bordered with India. The Project area is located at the eastern bank of the Sapta Koshi River. The terrain starts from foothills of the Siwalik range and slopes gently down to south with an inclination of 5 degrees on an average and is formed by alluvium of old and present rivers. The Project area is dominated by sandy soils having low to moderate water holding capacity. The climate in the project area is sub-tropical. Temperatures are high between March and October, the hottest month being the April, during which the mean daily maximum temperature is about 340C. During the cool period from November to February, mean monthly temperatures are in the range of 16 to 220C. The annual average rainfall between 1970 and 1993 was 1,867mm, raining intensively in the monsoon period, from late May to September. -

District Transport Master Plan (DTMP)
Government of Nepal District Transport Master Plan (DTMP) Ministry of Federal Affairs and Local Development Department of Local Infrastructure Development and Agricultural Roads (DOLIDAR) District Development Committee, Morang February 2013 Prepared by the District Technical Office (DTO) for Morang with Technical Assistance from the Department of Local Infrastructure and Agricultural Roads (DOLIDAR), Ministry of Federal Affairs and Local Development and grant supported by DFID i FOREWORD It is my great pleasure to introduce this District Transport Master Plan (DTMP) of Morang district especially for district road core network (DRCN). I believe that this document will be helpful in backstopping to Rural Transport Infrastructure Sector Wide Approach (RTI SWAp) through sustainable planning, resources mobilization, implementation and monitoring of the rural road sub-sector development. The document is anticipated to generate substantial employment opportunities for rural people through increased and reliable accessibility in on- farm and off-farm livelihood diversification, commercialization and industrialization of agriculture sector. In this context, rural road sector will play a fundamental role to strengthen and promote overall economic growth of this district through established and improved year round transport services reinforcing intra and inter-district linkages . Therefore, it is most crucial in executing rural road networks in a planned way as per the District Transport Master Plan (DTMP) by considering the framework of available resources in DDC comprising both internal and external sources. Viewing these aspects, DDC Morang has prepared the DTMP by focusing most of the available resources into upgrading and maintenance of the existing road networks. This document is also been assumed to be helpful to show the district road situations to the donor agencies through central government towards generating needy resources through basket fund approach. -

Saath-Saath Project
Saath-Saath Project Saath-Saath Project THIRD ANNUAL REPORT August 2013 – July 2014 September 2014 0 Submitted by Saath-Saath Project Gopal Bhawan, Anamika Galli Baluwatar – 4, Kathmandu Nepal T: +977-1-4437173 F: +977-1-4417475 E: [email protected] FHI 360 Nepal USAID Cooperative Agreement # AID-367-A-11-00005 USAID/Nepal Country Assistance Objective Intermediate Result 1 & 4 1 Table of Contents List of Acronyms .................................................................................................................................................i Executive Summary ............................................................................................................................................ 1 I. Introduction ........................................................................................................................................... 4 II. Program Management ........................................................................................................................... 6 III. Technical Program Elements (Program by Outputs) .............................................................................. 6 Outcome 1: Decreased HIV prevalence among selected MARPs ...................................................................... 6 Outcome 2: Increased use of Family Planning (FP) services among MARPs ................................................... 9 Outcome 3: Increased GON capacity to plan, commission and use SI ............................................................ 14 Outcome -

Master Plan of Agricultural Marketing in Eastern Development Region of Nepal
MASTER PLAN OF AGRICULTURAL MARKETING IN EASTERN DEVELOPMENT REGION OF NEPAL Final Report Submitted To Government of Nepal Ministry of Agricultural Development Department of Agriculture Agri. Business Promotion & Marketing Development Directorate (ABPMDD) Harihar Bhawan, Lalitpur Submitted By: Business Promotion Research and Communication Pvt. Ltd., (BPRC) Putalisadak, Kathmandu, Nepal Tel # 0977-01-4442853/4436617, Fax # 0977-01-4436617 Post Box # 19006, Email # [email protected] July 2017 (Ashad, 2074) Preface BPRC is pleased to undertake this Study "Master Plan of Agri-Marketing in Eastern Development Region of Nepal". BPRC expresses its gratitude to Agri Business Promotion and Marketing Development Directorate (ABPMDD) to having entrusted this important task. It also expresses gratitude to Mr. Laxman Prasad Paudel, Program Director and his team for expert guidance and for providing suggestions throughout the study period and report writing. BPRC is also thankful to ABDMDD team for their valuable, constructive comments and suggestions which were provided during Inception report and draft report presentations. We also express graduate to Senior Agriculture Marketing Officers Mr. Rajendra Prasad Pradhan and Mr. Puspa Raj Shahi for providing necessary instructions during final report preparation. BPRC acknowledges with gratitude the contribution made by study team of the project, with their valuable contribution the project was successfully brought to its conclusion. BPRC is most grateful to Mrs. Naina Dhakal, Team Leader for the successful execution of this project and for steering the whole tasks of conducting field study till its conclusion. In addition, BPRC conveys its appreciation to the contribution made by Chief and SMS of District Agriculture Development Offices, Agro-Vets, Traders, Wholesalers, Representative of District Development Committee, Member of Market Management Committee, Commercial Farmers Representatives and Agri-Cooperatives etc. -

Global Initiative on Out-Of-School Children
ALL CHILDREN IN SCHOOL Global Initiative on Out-of-School Children NEPAL COUNTRY STUDY JULY 2016 Government of Nepal Ministry of Education, Singh Darbar Kathmandu, Nepal Telephone: +977 1 4200381 www.moe.gov.np United Nations Educational, Scientific and Cultural Organization (UNESCO), Institute for Statistics P.O. Box 6128, Succursale Centre-Ville Montreal Quebec H3C 3J7 Canada Telephone: +1 514 343 6880 Email: [email protected] www.uis.unesco.org United Nations Children´s Fund Nepal Country Office United Nations House Harihar Bhawan, Pulchowk Lalitpur, Nepal Telephone: +977 1 5523200 www.unicef.org.np All rights reserved © United Nations Children’s Fund (UNICEF) 2016 Cover photo: © UNICEF Nepal/2016/ NShrestha Suggested citation: Ministry of Education, United Nations Children’s Fund (UNICEF) and United Nations Educational, Scientific and Cultural Organization (UNESCO), Global Initiative on Out of School Children – Nepal Country Study, July 2016, UNICEF, Kathmandu, Nepal, 2016. ALL CHILDREN IN SCHOOL Global Initiative on Out-of-School Children © UNICEF Nepal/2016/NShrestha NEPAL COUNTRY STUDY JULY 2016 Tel.: Government of Nepal MINISTRY OF EDUCATION Singha Durbar Ref. No.: Kathmandu, Nepal Foreword Nepal has made significant progress in achieving good results in school enrolment by having more children in school over the past decade, in spite of the unstable situation in the country. However, there are still many challenges related to equity when the net enrolment data are disaggregated at the district and school level, which are crucial and cannot be generalized. As per Flash Monitoring Report 2014- 15, the net enrolment rate for girls is high in primary school at 93.6%, it is 59.5% in lower secondary school, 42.5% in secondary school and only 8.1% in higher secondary school, which show that fewer girls complete the full cycle of education. -
Integrating Biological Resources for Prosperity February 6-7, 2020, Biratnagar
Organizers National Conference on Integrating Biological Resources for Prosperity February 6-7, 2020, Biratnagar ABSTRACT xxxix National Conference on Integrating Biological Resources for Prosperity February 6-7, 2020, Biratnagar ABSTRACT Advisory Committee Hon. Mr. Jagadish Prasad Kusiyait, Minister for Industry, Tourism, Forest & Environment, Province 1 Hon. Mr. Subodh Raj Pyakurel, Vice Chairman, Provincial Planning Commission, Province 1 Mr. Bhim Parajuli, Mayor, Biratnagar Metropolitan City, Biratnagar, Morang Dr. Bishwa Nath Oli, Secretary, Ministry of Forests and Environment, GoN Prof. Dr. Sanu Devi Joshi, Academician NAST Prof. Dr. Pramod Kumar Jha, Professor Emeritus, CDB, TU; Academician NAST Dr. Baburam Timalsena, Campus Chief, Mahendra Morang AM Campus, TU, Biratnagar Mr. Mahesh Kumar Khatri, Campus Chief, Post Graduate Campus, TU, Biratnagar Prof. Dr. Dhan Bahadur Karki, Campus Chief, Central Campus of Technology, TU, Dharan Prof. Dr. Ram Kailash Prasad Yadav, Head, Central Department of Botany, TU, Kathmandu Prof. Dr. Tej Bahadur Thapa, Head, Central Department of Zoology, TU, Kathmandu Prof. Dr. Sasinath Jha, Chairman, Nepal Biological Society, Biratnagar Prof. Dr. Ram Bahadur Thapa, TU, Nepal Prof. Dr. Min Raj Dhakal, Director, Research, Purwanchal University, Biratnagar Dr. Bharat Raj Subba, Post Graduate Campus, TU, Biratnagar Prof. Dr. Kalu Ram Khambu, Mechi Multiple Campus, Bhadrapur, Jhapa Prof. Dr. Damodar Thapa Chhetry, HOD, DoZ, Post Graduate Campus, TU, Biratnagar Mr. Dhananjay Poudel, DG, Department of Plant Resources, Thapathali, Kathmandu Dr. Buddi Sagar Poudel, Chief, REDD Implementation Centre, Kathmandu Mr. Sushil Kumar Jha, Post Graduate Campus, TU, Biratnagar Dr. Ganesh Bahadur Thapa, Chief, Natural History Museum, TU, Kathmandu Mr. Shailendra Kumar Pokharel, Founder President/ ED, Conservation Development Foundation, Kathamandu ii Organizing Committee Chairman Prof. -
The Institute of Chartered Accountants of Nepal RA Firm Renewal List from 2074-04-01 to 2075-03-21 Sno
The Institute of Chartered Accountants of Nepal RA Firm Renewal List From 2074-04-01 to 2075-03-21 SNo. Firm No. Name Address Phone 1 2002 D. A. & Associates Suswagat Marga, Mahankal Sthan, 01-4822252 Bouda -6,Kathmandu 2 2003 S. R. Neupane & Co. S. R. Neupane & Co., Birgunj 9845054857 3 2005 Kumar Jung & Co. Kumar Jung & Co. Hattiban, Dhapakhel- 5250079 1, Laitpur 4 2006 Ram & Co. Ram & Co. , Gaurigunj, Chitawan 5 2007 R. R. Joshi & Co. R.R. Joshi & Co. KMPC Ward No. -33, 4421020 Ga-1/319, Maitidevi, Kathmandu 6 2008 A. Kumar & Co. Tripureshowr Teku Road, Kathmandu 14260563 7 2009 Narayan & Co. Pokhara 11, Phulbari. 9846041049 8 2011 N. Bhandari & Co. N. Bhandari & Co. Maharajgunj, 9841240367 Kathmandu 9 2012 Giri & Co. Giri & Co. Dilli Bazar , Kathmandu 9851061197 10 2013 Laxman & Associates Laxman & Associates, Gaur, Rautahat 014822062, 9845032829 11 2014 Roshan & Co. Lalitpur -5, Lagankhel. 01 5534729, 9841103592 12 2016 Upreti Associates KMPC - 35, Shrinkhala Galli, Block No. 01 4154638, 9841973372 373/9, POB No. 23292, Ktm. 13 2018 K. M. S. & Associates KMPC 2 Balkhu Ktm 9851042104 14 2019 Yadav & Co. Kanchanpur-6, Saptari 0315602319 15 2020 M. G. & Co. Pokhara SMPC Ward No. 8, Pokhara 061-524068 16 2021 R.G.M. & Associates Thecho VDC Ward No. 7, Nhuchchhe 5545558 Tole, Lalitpur 17 2023 Umesh & Co. KMPC Ward No. -14, Kuleshwor, 014602450, 9841296719 Kathmandu 18 2025 Parajuli & Associates Mahankal VDC Ward No. 3, Kathmandu 014376515, 014372955 19 2028 Jagannath Satyal & Co. Bhaktapur MPC Ward No. -2, Jagate, 16614964 Bhaktapur 20 2029 R. Shrestha & Co. Lalitpur -16, Khanchhe 015541593, 9851119595 21 2030 Bishnu & Co. -
Socio–Economic and Cultural Barriers for Utilization of Pre-Natal Health Service in Urawn Community of Sunsari
SOCIO–ECONOMIC AND CULTURAL BARRIERS FOR UTILIZATION OF PRE-NATAL HEALTH SERVICE IN URAWN COMMUNITY OF SUNSARI By Sunita Kumari Mehta Exam Roll N0: 2180123/2069 T.U. Regd. No. : 7-1-217-213-2004 A Thesis Submitted to Health Education Department in Partial Fulfillment of the Requirements for Master's Degree in Health Education TRIBHUWAN UNIVERSITY FACULTY OF EDUCATION JANATA MULTIPLE CAMPUS HEALTH EDUCATION DEPARTMENT ITAHARI-5, SUNSARI 2074 RECOMMENDATION This is to certify that Sunita Kumari Mehta has prepared the thesis entitled "Socio- Economic and Cultural Barriers to the Utilization of Prenatal Health Service in Urawn Community" under my guidance and supervision. I recommend this thesis for acceptance. ......................................... Mr. Manoj Kr. Chaudhary (Supervisor and Lecturer) Janata Multiple Campus Date: ii APPROVAL SHEET This thesis entitled "Socio-Economic and Cultural Barriers to the Utilization of Prenatal Health Service in Urawn Community" submitted by Sunita Kumari Mehta in partial fulfillment of the requirements for the Degree of Master's in health education has been approved. Thesis Evaluation Committee Signature Mr. Sanjib Kumar Yadav ....................... Head, Department of Health Education Chairman Janata Multiple Campus, Itahari, Sunsari Mr. Manoj Kumar Chaudhary ........................ Janata Multiple Campus, Teaching Assistant Supervisor Itahari, Sunsari .................................. External Observer Date: iii DECLARATION I hereby declare that this thesis has not been submitted for any other degree. Sunita Kumari Mehta iv ACKNOWLEDGEMENT My deepest gratitude goes to my teacher and thesis supervisor associate Lecturer Manoj Kr. Chaudhary, Health Education Department of Janata Multiple Campus, Itahari, Sunsari for his continued guidance, encouragement, motivation and support at each step of the study. His regular and extensive guidance and encouragement were the main source of inspiration to accomplish this study successfully. -

The Feasibility Study on the Sunsari River Irrigation Project in the Kingdom of Nepal
JAPAN INTERNATIONAL COOPERATION AGENCY (JICA) DEPARTMENT OF IRRIGATION MINISTRY OF WATER RESOURCES HIS MAJESTY’S GOVERNMENT OF NEPAL THE FEASIBILITY STUDY ON THE SUNSARI RIVER IRRIGATION PROJECT IN THE KINGDOM OF NEPAL FINAL REPORT APPENDIXES January, 2003 SANYU CONSULTANTS INC. AFA JR 03-05 CONTENTS APPENDIXES APPENDIX-1 SCOPE OF WORK, MMs AND CONCERNED OFFICERS APPENDIX-2 REGIONAL ECONOMY APPENDIX-3 RURAL SOCIOLOGY AND GENDER APPENDIX-4 METEOROLOGY, HYDROLOGY AND HYDRO-ANALYSIS APPENDIX-5 AGRICULTURE DEVELOPMENT APPENDIX-6 IRRIGATION AND DRAINAGE DEVELOPMENT APPENDIX-7 HYDRO-GEOLOGY AND GROUNDWATER DEVELOPMENT APPENDIX-8 IRRIGATION FACILITIES AND RURAL INFRASTRUCTURE APPENDIX-9 INSTITUTIONAL DEVELOPMENT APPENDIX-10 ENVIRONMENT APPENDIX-11 COST RECOVERY AND PROJECT EVALUATION APPENDIX-12 PROJECT COST ACRONYMS AND ABBREVIATIONS ADB Asian Development Bank ADBN Agriculture Development Bank of Nepal ADO Agriculture Development Officer AIC Agricultural Inputs Corporation AO Association Organizer (employed by SMIP) APP Agricultural Perspective Plan AREP Agricultural Research and Extension Project (WB funded) ASC Agriculture Service Center CBS Central Bureau of Statistics CDO Chief District Officer CE Collection Efficiency (of Irrigation Service Fee) CMC Chatra Main Canal EDR Eastern Development Region ERID Eastern Regional Irrigation Directorate CGWISP Community Groundwater Irrigation Sector Project (ADB funded) DAC District Agriculture Committee DADO District Agricultural Development Office DDC District Development Committee DIO District -

Fb C/Ljgb S"Df/ /Fpt आडिल कुमारी गुप्ता जगन्नाथ स
खुला प्रलतयोलगता配मक परीक्षाको वीकृ त नामावली वबज्ञापन नं. : २०७७/७८/२१ (प्रदेश नं. २) तह : ४ पदः सहायक रोल नं. उ륍मेदवारको नाम उ륍मेदवारको नाम ललंग सम्륍मललत हुन चाहेको समूह थायी म्ि쥍ला थायी न. पा. / गा.वव.स बािेको नाम बाबुको नाम 1 AACHAL RAUT cf+rn /fpt Female ख쥍ु ला, महिला, मधेशी Bara Nijgadh hgswf/L k|;fb c/ljGb s"df/ /fpt 2 AADALI KUMARI GUPTA आडिल कु मारी गुप्ता Female ख쥍ु ला, महिला, मधेशी Dhanusa Janakpur जगन्नाथ साह डिजय साह 3 AAISHA KHATOON cfO;f vft"g Female ख쥍ु ला, महिला, मधेशी Dhanusa Tarapatti Sirsiya dxdb cf]lndg dxdb /lkms 4 AAKASH KUMAR JHA cfsfz s"""df/ ‰mf Male ख쥍ु ला, मधेशी Dhanusa janakpurdham k"/Gb/ ‰mf clg?$ ‰mf 5 AAKRITI NIDHI आकृ डि डिडि Female ख쥍ु ला, महिला Dhanusa Janakpur हररिाथ डिडि सडु िल कु मार डिडि 6 AANAND KUMAR YADAV cfgGb s"df/ ofbj Male ख쥍ु ला, मधेशी Siraha Pipra Pra Pi d"lgnfn ofba dxfb]j ofbj 7 AARADHNA CHAUDHARY अराििा चौिरी Female ख쥍ु ला, महिला, मधेशी Mahottari Jaleshwar शभु करण चौिरी श्याम डकशोर चौिरी 8 AARATI KARN आरिी कणण Female ख쥍ु ला, महिला, मधेशी Dhanusa Tarapatti Sirsiya प्रमोद लाल कणण डिरेन्द्र लाल कण ण कायस्थ 9 AARTI CHAUDHARY आरिी चौिरी Female ख쥍ु ला, महिला, आहिवासी / जनजाति Bara Baragadi टुगर चौिरी zf]ef चौिरी 10 AARTI GIRI cf/lt lul/ Female ख쥍ु ला, महिला Dhanusa chhireswarnath v*\u axfb"/ lu/L kf]i^ axfb"/ lu/L 11 AARTI GUPTA आरिी गुप्ता Female ख쥍ु ला, महिला Parsa sabaithawa गौरी प्रसाद गुप्ता सरु ेश कु मार गुप्ता 12 AARTI KUMARI JHA cf/tL s'df/L emf Female ख쥍ु ला, महिला Dhanusa Laxmipur Bageba afn s[ifण emf OGb| gf/fo)f emf 13 AARTI KUMARI SHRESTHA cf/lt s"df/L >]i& Female ख쥍ु ला, महिला,