SARS-Cov-2 Epitope Mapping on Microarrays Highlights Strong Immune-Response to N Protein Region
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

"Epitope Mapping: B-Cell Epitopes". In: Encyclopedia of Life Sciences
Epitope Mapping: B-cell Advanced article Epitopes Article Contents . Introduction GE Morris, Wolfson Centre for Inherited Neuromuscular Disease RJAH Orthopaedic Hospital, . What Is a B-cell Epitope? . Epitope Mapping Methods Oswestry, UK and Keele University, Keele, Staffordshire, UK . Applications Immunoglobulin molecules are folded to present a surface structure complementary to doi: 10.1002/9780470015902.a0002624.pub2 a surface feature on the antigen – the epitope is this feature of the antigen. Epitope mapping is the process of locating the antibody-binding site on the antigen, although the term is also applied more broadly to receptor–ligand interactions unrelated to the immune system. Introduction formed of highly convoluted peptide chains, so that resi- dues that lie close together on the protein surface are often Immunoglobulin molecules are folded in a way that as- far apart in the amino acid sequence (Barlow et al., 1986). sembles sequences from the variable regions of both the Consequently, most epitopes on native, globular proteins heavy and light chains into a surface feature (comprised of are conformation-dependent and they disappear if the up to six complementarity-determining regions (CDRs)) protein is denatured or fragmented. Sometimes, by acci- that is complementary in shape to a surface structure on the dent or design, antibodies are produced against linear antigen. These two surface features, the ‘paratope’ on the (sequential) epitopes that survive denaturation, though antibody and the ‘epitope’ on the antigen, may have a cer- such antibodies usually fail to recognize the native protein. tain amount of flexibility to allow an ‘induced fit’ between The simplest way to find out whether an epitope is confor- them. -

Ige – the Main Player of Food Allergy
DDMOD-431; No of Pages 8 Vol. xxx, No. xx 2016 Drug Discovery Today: Disease Models Editors-in-Chief Jan Tornell – AstraZeneca, Sweden DRUG DISCOVERY Andrew McCulloch – University of California, SanDiego, USA TODAY DISEASE MODELS IgE – the main player of food allergy 1 2,3 2 Henrike C.H. Broekman , Thomas Eiwegger , Julia Upton , 4, Katrine L. Bøgh * 1 Department of Dermatology/Allergology, University Medical Centre Utrecht (UMCU), Utrecht, The Netherlands 2 Division of Immunology and Allergy, Food Allergy and Anaphylaxis Program, The Department of Paediatrics, Hospital for Sick Children, Toronto, Canada 3 Research Institute, Physiology and Experimental Medicine, The University of Toronto, Toronto, Canada 4 National Food Institute, Technical University of Denmark, Søborg, Denmark Food allergy is a growing problem worldwide, presently Section editor: affecting 2–4% of adults and 5–8% of young children. IgE Michelle Epstein – Medical University of Vienna, is a key player in food allergy. Consequently huge Department of Dermatology, DIAID, Experimental Allergy, Waehringer Guertel 18-20, Room 4P9.02, A1090, efforts have been made to develop tests to detect Vienna, Austria. either the presence of IgE molecules, their allergen binding sites or their functionality, in order to provide allergen ingestion [1], and involve one or more of the follow- information regarding the patient’s food allergy. The ing systems; the skin (pruritus, urticaria, or angioedema), the ultimate goal is to develop tools that are capable of gastro-intestinal tract (diarrhea, vomiting, contractions, in- creased bowel movement), the respiratory tract (asthma at- discriminating between asymptomatic sensitization tack, hoarseness, stridor/laryngeal angioedema) or the and a clinically relevant food allergy, and between cardiovascular system (dizziness, drop in blood pressure, loss different allergic phenotypes in an accurate and trust- of consciousness) [2,3]. -

Protein Epitope Mapping by Mass Spectrometry
Anal. Chem. 1994,66, 3723-3726 Protein Epitope Mapping By Mass Spectrometry Ylngmlng Zhao and Brian T. Chalt’ The Rockefeller University, 1230 York Avenue, New York, New York 10021 A mass spectrometricmethod is described for the rapid mapping antigen bound to an antibody. Alternatively, these workers of linear epitopes in proteins that are bound by monoclonal subjected the peptide to proteolytic digestion and identified antibodies. The method consists of three steps. In the first products that bound to the immobilized antibody. In both step, an antigen protein is digested by a proteolytic enzyme to cases, the peptides of interest were identified by 2Wfplasma produce an appropriate set of peptide fragments. In the second desorption mass spectrometry. step, peptide fragments containing the linear epitope are selected Matrix-assisted laser desorption mass spectrometry (MAL- and separated from the pool of peptide fragments by immu- DI-MS) is a recently developed method for measuring the noprecipitation with the monoclonal antibody. In the final molecular weights of peptides and proteins.12-14 The technique step, the immunoprecipitated peptides are identified by matrix- allows the accurate (better than O.l%), rapid (<1 min), and assisted laser desorption mass spectrometry. The method sensitive (<1 pmol) determination of the molecular weights allows the rapid determination of antigenic sites without tedious of components of complex mixtures of peptides. MALDI- peptide synthesis or protein mutagenesis. The approach is MS is finding wide use for the rapid identification of proteins demonstrated through the mapping of epitopes in two peptides and the elucidation of their primary structures (in particular, (melittin and glucagon-like peptide-1 7-37) against which the definition of posttranslational modifications.) monoclonal antibodies were raised. -
ENCODE DCC Antibody Validation Document
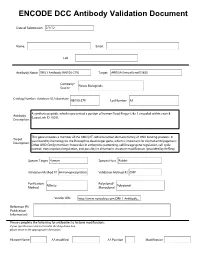
ENCODE DCC Antibody Validation Document Date of Submission Name: Email: Lab Antibody Name: Target: Company/ Source: Catalog Number, database ID, laboratory Lot Number Antibody Description: Target Description: Species Target Species Host Validation Method #1 Validation Method #2 Purification Polyclonal/ Method Monoclonal Vendor URL: Reference (PI/ Publication Information) Please complete the following for antibodies to histone modifications: if your specifications are not listed in the drop-down box, please write-in the appropriate information Histone Name AA modified AA Position Modification Validation #1 Analysis Insert Validation Image (click here) ARID3A (NB100-279) & (sc-8821) Immunoblot / Immunoprecipitation A. MW (kD) B. MW (kD) C. MW (kD) D. MW (kD) 150 150 150 150 100 100 100 100 75 75 75 75 50 50 50 50 38 38 38 38 25 25 25 20 20 20 25 15 15 15 15 Lane : 1 2 3 4 Lane : 1 2 3 Lane : 1 2 Lane : 1 2 3 A. Western Blot using NB100-279 on nuclear lysates from cell lines GM12878 (Lane1), K562 (Lane2), HeLaS3 (Lane3), and HepG2 (Lane4). B. Immunoprecipitation was performed on nuclear lysates from K562 cells using antibody NB100-279. Lane1: Nuclear lysate. Lane 3: Bound material from control immunoprecipitation with rabbit IgG. Lane 2: Bound material from immunoprecipitation with NB100-279. C. Western Blot using sc-8821 on nuclear lysates from cell lines GM12878 (Lane1), K562 (Lane2). D. Immunoprecipitation was performed on nuclear lysates from K562 cells using antibody sc-8821 and immunoblot with NB100-279. Lane1: Nuclear lysate. Lane 2: Bound material from immunoprecipitation with sc-8821. Lane 3: Bound material from control immunoprecipitation with Goat IgG. -
![Epitope Mapping of an Uncertain Endogenous Antigen Implies Secretogranin II Peptide Splicing [Version 2; Peer Review: 1 Approved, 2 Approved with Reservations]](https://docslib.b-cdn.net/cover/9315/epitope-mapping-of-an-uncertain-endogenous-antigen-implies-secretogranin-ii-peptide-splicing-version-2-peer-review-1-approved-2-approved-with-reservations-409315.webp)
Epitope Mapping of an Uncertain Endogenous Antigen Implies Secretogranin II Peptide Splicing [Version 2; Peer Review: 1 Approved, 2 Approved with Reservations]
F1000Research 2019, 8:1732 Last updated: 26 JUL 2021 RESEARCH ARTICLE Epitope mapping of an uncertain endogenous antigen implies secretogranin II peptide splicing [version 2; peer review: 1 approved, 2 approved with reservations] David R. Howlett 1, Iain J. Clarke2, Russell P. Newton3, John E. Hart4 1Wolfson Centre for Age Related Disease, Kings College London, London, SE1 1UL, UK 2School of Agriculture and Veterinary Science, Melbourne University, Parkville, Victoria, VIC 3010, Australia 3Biochemistry Group, Institute of Life Sciences, Medical School, Swansea University, Swansea, Wales, SA2 8PP, UK 4Endocrine Pharmaceuticals Ltd, Tadley, Hampshire, RG26 3TA, UK v2 First published: 09 Oct 2019, 8:1732 Open Peer Review https://doi.org/10.12688/f1000research.20633.1 Latest published: 05 Dec 2019, 8:1732 https://doi.org/10.12688/f1000research.20633.2 Reviewer Status Invited Reviewers Abstract Background: The search for a tissue-mass reducing reproductive 1 2 3 hormone involved a bioassay-guided physicochemical fractionation of sheep blood plasma. This brought forth a candidate protein whose version 2 apparent mass on gels and in mass spectrometry (MS) was 7-8 kDa, (revision) report report implying a polypeptide of ~70 residues. Four purification runs gave 05 Dec 2019 Edman N-terminal sequences relating to 1MKPLTGKVKEFNNI14. This is bioinformatically obscure and has been resistant to molecular version 1 biological investigation. The sequence was synthesized as the peptide 09 Oct 2019 report report EPL001, against which was raised a goat polyclonal antiserum, G530. Used in an antigen capture campaign, G530 pointed to the existence of a novel derivative of secretogranin II (SgII), the neuroendocrine 1. -
Highly Accurate and Reproducible Diagnosis of Peanut Allergy Using Epitope Mapping
medRxiv preprint doi: https://doi.org/10.1101/2020.06.19.20136002; this version posted June 20, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted medRxiv a license to display the preprint in perpetuity. It is made available under a CC-BY-NC-ND 4.0 International license . Highly Accurate and Reproducible Diagnosis of Peanut Allergy Using Epitope Mapping Paul Kearney1, Robert Getts1, Clive Hayward1, David Luta1, Alex Porter1, Marc Witmer1, George du Toit2, Gideon Lack2, R. Sharon Chinthrajah3, Stephen J Galli3,4, Kari Nadeau3, Galina Grishina5, Mayte Suárez-Fariñas5, Maria Suprun5, Hugh A Sampson5 1. AllerGenis LLC, Hatfield, PA, USA 2. King’s College London, London, UK 3. Sean N. Parker Center for Allergy and Asthma Research at Stanford University, Stanford, USA 4. Departments of Pathology and Microbiology & Immunology, Stanford University. 5. Department of Pediatrics, Allergy and Immunology, Icahn School of Medicine at Mount Sinai, New York, NY, USA Abstract Background: Misdiagnosis of peanut allergy is a significant clinical challenge. Here, a novel diagnostic blood-based test using a Bead-Based Epitope Assay (“peanut BBEA”) has been developed on the LEAP cohort and then independently validated on the CoFAR2 and POISED cohorts. Methods: Development of the peanut BBEA followed the National Academy of Medicine’s established guidelines with discovery performed on 133 subjects from the non- interventional arm of the LEAP trial and an independent validation performed on 81 subjects from the CoFAR2 study and 84 subjects from the POISED study. All subject samples were analyzed using the BBEA methodology. -

Inkjet Printing for the Production of Protein Microarrays Mcwilliam Et Al Mimb Protein Microarrays Chapter 21
Methods in Molecular Biology Protein Microarrays Chapter 21: Inkjet Printing for the Production of Protein Microarrays Iain McWilliam*, Marisa Chong Kwan, Duncan Hall Arrayjet Ltd., MIC, Roslin, EH25 9RE, UK * Corresponding Author Keywords i. Inkjet ii. Microarrayer iii. Protein microarray iv. Printing buffer v. Diagnostic microarray vi. Non-contact vii. JetSpyder viii. JetGuard ix. Microarray production x. Antibody microarray Introduction Since their inception in 1995, microarrays have been the icon of the ‘omics revolution. Whereas DNA can be printed onto a wide range of surface chemistries with a wide range of buffers, proteins must be printed in buffers which protect them and onto substrates which maintain their structural integrity, binding sites and activity. Common buffers for protein storage contain cryoprotectorants (e.g. glycerol (1) or ethylene glycol) which add to the often viscous nature of protein solutions, so the ability of a microarrayer to print such solutions without extensive modification is a distinct advantage when producing protein microarrays. The most popular substrates for protein microarrays, designed specifically with structural protection in mind, are made with thin nitrocellulose or hydrogel coatings and are fragile themselves, which encourages the use of a non—contact method of printing. When addressing production throughput requirements, the ability to handle multiple samples simultaneously and to print those samples quickly on—the—fly is important to minimise production timescales. The technology should also be scalable and robust enough to accommodate a shift from R+D level production to full—scale, manufacturing levels of production. Arrayjet has used the key factors of being able to print potentially viscous protein solutions with a non—contact printing method to develop a range of microarrayers, all centred around an industrially proven inkjet printhead, which are highly suited to printing high quality protein microarrays at all levels of production. -

Process Development for Manufacturing Stochastic Peptide Microarrays
Process Development for Manufacturing Stochastic Peptide Microarrays Zur Erlangung des akademischen Grades eines DOKTORS DER INGENIEURSWISSENSCHAFTEN (Dr.-Ing.) von der KIT-Fakultät für Maschinenbau des Karlsruher Instituts für Technologie (KIT) angenommene DISSERTATION von M.Sc. Roman Popov Tag der mündlichen Prüfung: 20. März 2018 Hauptreferent: apl. Prof. Dr. Alexander Nesterov-Müller Korreferenten: Prof. Dr. Jan Korvink Prof. Dr.-Ing. Matthias Franzreb Dieses Werk ist unter einer Creative Commons Namensnennung – Nicht-kommerziell – Weitergabe unter gleichen Bedingungen 4.0 International Lizenz (CC BY-NC-SA 4.0) lizensiert: https://creativecommons.org/licenses/by-nc-sa/4.0/deed.de This document is licensed under a Creative Commons Attribution- NonCommercial-ShareAlike 4.0 International License (CC BY-NC-SA 4.0): https://creativecommons.org/licenses/by-nc-sa/4.0/deed.en Abstract Tackling the challenges of developing therapies for cancer, infections, or immune system disorders requires understanding and manipulation of the metabolic pathways related to a disease state or a pathogen. An essential role in the corresponding biochemical cascades is played by proteins of various types, whose functions are manifested through their interactions with other molecules. In basic and applied research, the functionality and binding properties of proteins are more often studied using peptide microarrays, which are collections of protein fragments displayed on a solid support in a spot array format. Commercially available peptide microarrays are manufactured using various methods, which result in different spot densities and costs per spot. While being relatively simple and straightforward to implement, the wide-spread SPOT- technique provides less than a thousand of peptides on a standard size substrate, which is not sufficient for many biological applications. -

Molecular Immunology a Machine-Learning Approach for Predicting B-Cell Epitopes
Molecular Immunology 46 (2009) 840–847 Contents lists available at ScienceDirect Molecular Immunology journal homepage: www.elsevier.com/locate/molimm A machine-learning approach for predicting B-cell epitopes Nimrod D. Rubinstein, Itay Mayrose, Tal Pupko ∗ Department of Cell Research and Immunology, Tel Aviv University, Tel Aviv 69978, Israel article info abstract Article history: The immune activity of an antibody is directed against a specific region on its target antigen known as Received 25 May 2008 the epitope. Numerous immunodetection and immunotheraputics applications are based on the ability of Received in revised form 23 July 2008 antibodies to recognize epitopes. The detection of immunogenic regions is often an essential step in these Accepted 7 September 2008 applications. The experimental approaches used for detecting immunogenic regions are often laborious Available online 22 October 2008 and resource-intensive. Thus, computational methods for the prediction of immunogenic regions allevi- ate this drawback by guiding the experimental procedures. In this work we developed a computational Keywords: method for the prediction of immunogenic regions from either the protein three-dimensional structure Antigen Antibody or sequence when the structure is unavailable. The method implements a machine-learning algorithm Epitope that was trained to recognize immunogenic patterns based on a large benchmark dataset of validated Immunogenic regions epitopes derived from antigen structures and sequences. We compare our method to other available tools Prediction that perform the same task and show that it outperforms them. Properties © 2008 Elsevier Ltd. All rights reserved. Surface 1. Introduction Woods, 1981; Karplus and Schulz, 1985; Kolaskar and Tongaonkar, 1990; Kulkarni-Kale et al., 2005; Parker et al., 1986; Pellequer et The ability of an antibody to specifically bind an antigen is al., 1991). -

Polyclonal Epitope Cartography Reveals the Temporal Dynamics and Diversity of Human Antibody Responses to H5N1 Vaccination
bioRxiv preprint doi: https://doi.org/10.1101/2020.06.16.155754; this version posted June 17, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. Polyclonal epitope cartography reveals the temporal dynamics and diversity of human antibody responses to H5N1 vaccination Julianna Han1, Aaron J. Schmitz2, Sara T. Richey1, Ya-Nan Dai2, Hannah L. Turner1, Bassem M. Mohammed2, Daved H. Fremont2,3,4, Ali H. Ellebedy2,4, Andrew B. Ward1,5* 1Department of Integrative Structural and Computational Biology, The Scripps Research Institute, La Jolla, CA, 92037, USA. 2Department of Pathology and Immunology, Washington University School of Medicine, St Louis, MO, 63110, USA. 3Department of Biochemistry & Molecular Biophysics, Washington University School of Medicine, St. Louis, MO, 63110, USA. 4Department of Molecular Microbiology, Washington University School of Medicine, St. Louis, MO, 63110, USA. 5Lead contact *Correspondence: [email protected] (A.B.W.) SUMMARY Novel influenza A virus (IAV) strains elicit recall immune responses to conserved epitopes, making them favorable antigenic choices for universal influenza virus vaccines. Evaluating these immunogens requires a thorough understanding of the antigenic sites targeted by the polyclonal antibody (pAb) response, which single particle electron microscopy (EM) can sensitively detect. Here, we employed EM polyclonal epitope mapping (EMPEM) to extensively characterize the pAb response to hemagglutinin (HA) after H5N1 immunization in humans. Cross-reactive pAbs originating from memory B cells immediately bound the stem of HA and persisted for over a year post vaccination. -

Proteome-Wide Epitope Mapping Identifies a Resource of Antibodies
Signal Transduction and Targeted Therapy www.nature.com/sigtrans LETTER OPEN Proteome-wide epitope mapping identifies a resource of antibodies for SARS-CoV-2 detection and neutralization Signal Transduction and Targeted Therapy (2021) 6:166; https://doi.org/10.1038/s41392-021-00573-9 Dear Editor, The epitopes of 15 antibodies to the SARS-CoV-2 ORF1ab, M, E, Since December 2019, the coronavirus disease 2019 (COVID- ORF6, ORF7a, and ORF8 proteins were also analyzed (Supple- 19) caused by the severe acute respiratory syndrome mentary Table S2 and Fig. S2). Our analyses indicate that the coronavirus-2 (SARS-CoV-2) has become a worldwide pandemic.1 epitopes of ORF1ab antibodies are located on nsp1, nsp2, nsp3, Significant efforts have been made to generate antibodies to nsp12, and nsp13 proteins (Supplementary Fig. S2a). The epitopes help study COVID-19 pathogenesis, perform diagnostic testing, of two ORF3a antibodies (#45 and #46) are 266-EPTTTTSVPL-275, and develop treatment to neutralize SARS-CoV-2 activity. 176-TSPIS-180, respectively. Another ORF3a antibody (#47) has However, the specific sequence of amino acids recognized and two epitopes, including 246-IHTID-250 and 266-EPTTTTSVPL-275 bound by an antibody, the “epitope” is unknown for most (Supplementary Fig. S2b). Two rabbit polyclonal anti-M antibodies antibodies. In this study, we developed a high-throughput (#42, #43) bind to 186-RVAGDSGFAAYSRYR-200 and 206-LNTDH- epitope mapping platform using a peptide-based SARS-CoV-2 210, respectively (Supplementary Fig. S2c). The E protein antibody proteome microarray.2 to detect the binding epitopes of 57 (#44) has two epitopes, including 16-SVLLF-20 and 56- commercial antibodies to ORF1ab, nucleocapsid (N), spike (S), FYVYSRVKNLNSSRVPDLLV-75 (Supplementary Fig. -

Longitudinal Development of Antibody Responses in COVID-19 Patients of Different Severity with ELISA, Peptide, and Glycan Arrays: an Immunological Case Series
pathogens Article Longitudinal Development of Antibody Responses in COVID-19 Patients of Different Severity with ELISA, Peptide, and Glycan Arrays: An Immunological Case Series Jasmin Heidepriem 1,†, Christine Dahlke 2,3,4,*,† , Robin Kobbe 2, René Santer 5, Till Koch 2,3,4 , Anahita Fathi 2,3,4 , Bruna M. S. Seco 1 , My L. Ly 2,3,4, Stefan Schmiedel 2, Dorothee Schwinge 6, Sonia Serna 7 , Katrin Sellrie 1, Niels-Christian Reichardt 7,8, Peter H. Seeberger 1 , Marylyn M. Addo 2,3,4,* , Felix F. Loeffler 1,* and on behalf of the ID-UKE COVID-19 Study Group ‡ 1 Department of Biomolecular Systems, Max Planck Institute of Colloids and Interfaces, Am Muehlenberg 1, 14476 Potsdam, Germany; [email protected] (J.H.); [email protected] (B.M.S.S.); [email protected] (K.S.); [email protected] (P.H.S.) 2 Division of Infectious Diseases, First Department of Medicine, University Medical Center Hamburg-Eppendorf, 20251 Hamburg, Germany; [email protected] (R.K.); [email protected] (T.K.); [email protected] (A.F.); [email protected] (M.L.L.); [email protected] (S.S.) 3 Department of Clinical Immunology of Infectious Diseases, Bernhard Nocht Institute for Tropical Medicine, 20251 Hamburg, Germany 4 German Center for Infection Research, Partner Site Hamburg-Lübeck-Borstel-Riems, Citation: Heidepriem, J.; Dahlke, C.; 20251 Hamburg, Germany 5 Kobbe, R.; Santer, R.; Koch, T.; Fathi, Department of Pediatrics, University Medical Center Hamburg-Eppendorf, 20251 Hamburg, Germany; A.; Seco, B.M.S.; Ly, M.L.; Schmiedel, [email protected] 6 I.