Preventing the Spread of EVD in Liberia Through Community Engagement and Surveillance
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

TRC of Liberia Final Report Volum Ii
REPUBLIC OF LIBERIA FINAL REPORT VOLUME II: CONSOLIDATED FINAL REPORT This volume constitutes the final and complete report of the TRC of Liberia containing findings, determinations and recommendations to the government and people of Liberia Volume II: Consolidated Final Report Table of Contents List of Abbreviations <<<<<<<<<<<<<<<<<<<<<<<............. i Acknowledgements <<<<<<<<<<<<<<<<<<<<<<<<<<... iii Final Statement from the Commission <<<<<<<<<<<<<<<............... v Quotations <<<<<<<<<<<<<<<<<<<<<<<<<<<<<<. 1 1.0 Executive Summary <<<<<<<<<<<<<<<<<<<<<<<< 2 1.1 Mandate of the TRC <<<<<<<<<<<<<<<<<<<<<<<< 2 1.2 Background of the Founding of Liberia <<<<<<<<<<<<<<<... 3 1.3 History of the Conflict <<<<<<<<<<<<<<<<<<<................ 4 1.4 Findings and Determinations <<<<<<<<<<<<<<<<<<<< 6 1.5 Recommendations <<<<<<<<<<<<<<<<<<<<<<<<... 12 1.5.1 To the People of Liberia <<<<<<<<<<<<<<<<<<<. 12 1.5.2 To the Government of Liberia <<<<<<<<<<. <<<<<<. 12 1.5.3 To the International Community <<<<<<<<<<<<<<<. 13 2.0 Introduction <<<<<<<<<<<<<<<<<<<<<<<<<<<. 14 2.1 The Beginning <<................................................................................................... 14 2.2 Profile of Commissioners of the TRC of Liberia <<<<<<<<<<<<.. 14 2.3 Profile of International Technical Advisory Committee <<<<<<<<<. 18 2.4 Secretariat and Specialized Staff <<<<<<<<<<<<<<<<<<<. 20 2.5 Commissioners, Specialists, Senior Staff, and Administration <<<<<<.. 21 2.5.1 Commissioners <<<<<<<<<<<<<<<<<<<<<<<. 22 2.5.2 International Technical Advisory -
Newsletter Humanitarian Edition Issue
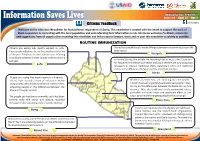
http://www.usaid.gov/ https://www.internews.org/ http://www.healthcommcapacity.org/ Humanitaritan Newsletter Information Saves Lives Issue #8 - April 25 - May 1 Citizens’ Feedback http://on.fb.me/1NM9DKthttps://www.facebook.com/internewsliberia?fref=ts/internewsliberia Welcome to the Internews Newsletter for humanitarian responders in Liberia. This newsletter is created with the intent to support the work of Ebola responders in connecting with the local population and understanding their information needs. Internews welcomes feedback, comments and suggestions from all organizations receiving this newsletter and invites you to forward, share and re-post this newsletter as widely as possible. ROUTINE IMMUNIZATION Citizens are asking why health workers in Lofa The residents would like to know the difference between the routine vaccine and the County have rolled out the routine vaccine at this time Ebola vaccine. of the year. They fear it is the Ebola vaccine, referring Gbarpolu to an Ebola outbreak in their county at the same time In Nimba County, the people are reporting that an NGO called Crusaders last year. Lofa for Peace and the Ministry of Health and Social Welfare are now using local languages to educate traditional chiefs, paramount rulers and traditional elders on the differences between routine and Ebola vaccines. Nimba People are saying that health workers in Fuamah district have trained a team of volunteers within Residents in River Cess are reporting that the health Bong County, who would move into all communities, ministry has been organizing awareness campaigns in their educating people on the differences between the county on the differences between the Ebola and routine Ebola and routine vaccine. -

Refugee Livelihood Assistance and Support for Economic Inclusion
Sep 27, 2021, 9:09:17 AM Call for Expression of Interest Refugee Livelihood Assistance and Support for Economic Inclusion HCR/LBR/2020/004 1 Timeline Posted Nov 12, 2020 Clarification Request Deadline Nov 23, 2020 Application Deadline Nov 26, 2020 Notification of Results Dec 11, 2020 Start Date Jan 1, 2021 End Date Dec 31, 2021 2 Locations A Liberia a Grand Kru County b Grand Gedeh County c Nimba d Margibi County 3 Sector(s) and area(s) of specialization A Livelihoods a Self reliance b Smallholder agricultural market support 4 Issuing Agency UNHCR 5 Project Background The purpose of this call for expression of interest is to identify interested and prospective partners (including organizations, NGOs, Associations, civil society institutions etc.) to support planning and implementation of protection and assistance to newly arrived refugees in Nimba, Grand Gedeh and Maryland Counties of Liberia. The specific locations for the projects are indicated below:Nimba County: SaclepeaGrand Gedeh County: Zwedru Maryland County: HarperMontserrado County: MonroviaThe application and expression of interest should outline:- Capacity, expertise, experience, structure of the applying organization in the provision of Livelihood assistance in a humanitarian setting, while integrating a protection and community based approach.- Organizations that are not UNHCR implementing partners are required to present previous audit reports along with the concept note.- Submit a concept note for designing and implementing programmes and activities which meet the objectives outlined below including desired outcomes and implementation approach. The concept note should be concise and contain clear information. A template is annexed to this call for expression.Agencies are encouraged to apply for more than one sector clearly showing the synergies between sectors, as well as their contribution towards innovative solutions. -

Land Commission Consultations
Republic of Liberia REPORT 2010 Land Commission Consultations Land Commission Consultations 2010 ACKNOWLEDGMENTS This report was compiled and written by the Program Staff of the Technical Secretariat of the Land Commission (LC) under the guidance and supervision of Mr. Stanley N. Toe, Land Policy and Program Development Officer. The Technical Secretariat extends its profound appreciation and gratitude to Chairman Brandy and other Commissioners of the LC for their unflinching support to this undertaking from the inception stage to the conclusion. We also acknowledge with thanks, the vital role played by Mrs. Guglielma da Passano, UN-Habitat Technical Advisor to the Land Commission in providing editorial guidance and useful feed- back during the entire exercise. An array of individuals and institutions also contributed immensely to the successful conduct of the county meetings. We hereby mention some of their names in recognition of their contributions in the form of financial and logistical support: the Minister and staff of the Ministry of Internal Affairs (MIA), superintendents and local officials of the counties, our international partners in particular, the UN-Habitat for providing the funding and logistical support for these consultative meetings. Also, the Norwegian Refugee Council (NRC) for logistical and related support during the consultative meetings in Nimba, Bong and Lofa Counties respectively and the United Nations Mission in Liberia (UNMIL). Finally, to the participants from the various counties, normally unheralded and acknowledged in matters such as this, we say in the proverbial Liberian jargon ‘thank you yah’ for taking time off your engaging schedules to honor our invitation to participate in these meetings. -

Download (2MB)
Pailey, Robtel Neajai (2014) The love of liberty divided us here? : factors leading to the introduction and postponement in passage of Liberia's Dual Citizenship Bill. PhD Thesis. SOAS, University of London. http://eprints.soas.ac.uk/id/eprint/20324 Copyright © and Moral Rights for this PhD Thesis are retained by the author and/or other copyright owners. A copy can be downloaded for personal non‐commercial research or study, without prior permission or charge. This PhD Thesis cannot be reproduced or quoted extensively from without first obtaining permission in writing from the copyright holder/s. The content must not be changed in any way or sold commercially in any format or medium without the formal permission of the copyright holders. When referring to this PhD Thesis, full bibliographic details including the author, title, awarding institution and date of the PhD Thesis must be given e.g. AUTHOR (year of submission) "Full PhD Thesis title", name of the School or Department, PhD PhD Thesis, pagination. The Love of Liberty Divided Us Here? Factors Leading to the Introduction and Postponement in Passage of Liberia’s Dual Citizenship Bill ROBTEL NEAJAI PAILEY Thesis submitted for the degree of PhD 2014 Department of Development Studies SOAS, University of London 1 Declaration for SOAS PhD Thesis I hAve reAd And understood regulAtion 17.9 of the RegulAtions for students of SOAS, University of London, concerning plAgiArism. I undertAke thAt All the materiAl presented for exAminAtion is my own work And hAs not been written for me, in whole or in part, by any other person. -

Liberia IDSR Epidemiology Bulletin 2017 Epi Week 38 (Sept
Liberia IDSR Epidemiology Bulletin 2017 Epi Week 38 (Sept. 18-24, 2017) Country Population: 4,373,279 l Volume 09, Issue 38 Sept. 18 – 24, 2017 l Data Source: CSOs from 15 Counties and Lab Highlights Figure 1. Public Health Events Reported in Epi- Keynotes and Events of Public Health week 38 Significance n A total of ninety-one suspected cases of immediately reportable diseases and events including 23 deaths were reported from 15 counties Health facility reporting completeness and timeliness are 98% and 94% respectively Measles outbreaks confirmed in Bong and Nimba Counties Eight neonatal deaths identified retrospectively in Bong County Grand Kru County reached alert threshold for meningitis with six suspected cases reported. o However, only one case was confirmed and the other five discarded due to negative lab results Reporting Coverage Table 1. Weekly IDSR Reporting Coverage, Liberia, Epi week 38, 2017 Number of Number of Number Expected Health Reports Received Completeness Timeliness 716 (94%) County Facility Report Received on Time (%) (%) Health facilities Bomi 23 23 0 100 0 out of 759 Bong 55 54 54 98 98 reported timely Gbarpolu 15 15 15 100 100 IDSR data Grand Bassa 33 33 33 100 100 Grand Cape Mount 32 32 32 100 100 Grand Gedeh 24 24 24 100 100 Grand Kru 19 19 19 100 100 91 (100%) Lofa 59 59 59 100 100 Health districts Margibi 44 44 44 100 100 reported IDSR Maryland 25 25 25 100 100 data Montserrado 283 283 283 100 100 Nimba 74 74 74 100 100 Rivercess 19 19 19 100 100 758(98%) River Gee 19 19 0 100 0 Health facilities Sinoe 35 35 35 100 100 reported IDSR Liberia (National) 759 758 716 97 94 data Legend ≥80 <80 All counties submitted weekly IDSR report on time except River Gee & Bomi counties The national target for weekly IDSR reporting is 80% IDSR Weekly Epidemiology and Surveillance Bulletin Page 1 Liberia IDSR Epidemiology Bulletin 2017 Epi Week 38 (Sept. -

Annex Xviii: Detailed Maps Per County
RURAL ENERGY STRATEGY AND MASTER PLAN FOR LIBERIA TECHNICAL REPORT ANNEX XVIII: DETAILED MAPS PER COUNTY 1 RURAL ENERGY ACTION PLAN PER COUNTY 1.1 BOMI Figure 1.1 – Infrastructure map for Bomi County – Phase 1. Annex XVIII| Page 1 LR.2016.R.001.2 RURAL ENERGY STRATEGY AND MASTER PLAN FOR LIBERIA TECHNICAL REPORT Figure 1.2 – Infrastructure map for Bomi County – Phase 2. Annex XVIII| Page 2 LR.2016.R.001.2 RURAL ENERGY STRATEGY AND MASTER PLAN FOR LIBERIA TECHNICAL REPORT Figure 1.3 – Infrastructure map for Bomi County – Phase 3. Annex XVIII| Page 3 LR.2016.R.001.2 RURAL ENERGY STRATEGY AND MASTER PLAN FOR LIBERIA TECHNICAL REPORT 1.2 BONG Figure 1.4 – Infrastructure map for Bong County – Phase 1. Annex XVIII| Page 4 LR.2016.R.001.2 RURAL ENERGY STRATEGY AND MASTER PLAN FOR LIBERIA TECHNICAL REPORT Figure 1.5 – Infrastructure map for Bong County – Phase 2. Annex XVIII| Page 5 LR.2016.R.001.2 RURAL ENERGY STRATEGY AND MASTER PLAN FOR LIBERIA TECHNICAL REPORT Figure 1.6 – Infrastructure map for Bong County – Phase 3. Annex XVIII| Page 6 LR.2016.R.001.2 RURAL ENERGY STRATEGY AND MASTER PLAN FOR LIBERIA TECHNICAL REPORT 1.3 GBARPOLU Figure 1.7 – Infrastructure map for Gbarpolu County – Phase 1. Annex XVIII| Page 7 LR.2016.R.001.2 RURAL ENERGY STRATEGY AND MASTER PLAN FOR LIBERIA TECHNICAL REPORT Figure 1.8 – Infrastructure map for Gbarpolu County – Phase 2. Annex XVIII| Page 8 LR.2016.R.001.2 RURAL ENERGY STRATEGY AND MASTER PLAN FOR LIBERIA TECHNICAL REPORT Figure 1.9 – Infrastructure map for Gbarpolu County – Phase 3. -

RSPO NOTIFICATION of PROPOSED NEW PLANTING This
RSPO NOTIFICATION OF PROPOSED NEW PLANTING This notification shall be on the RSPO website f`or 30 days as required by the RSPO procedures for new plantings (http://www.rspo.org/?q=page/53). It has also been posted on local on-site notice boards. Date of notification: Tick whichever is appropriate √ This is a completely new development and stakeholders may submit comments. This is part of an ongoing planting and is meant for notification only. Location of proposed new Tarjuowon District, Sinoe County, Republic of Liberia planting: Company Name Golden Veroleum (Liberia) Inc. Address 17th Street, Villa Samantha ( Beach Side), Sinkor, Monrovia, Liberia Phone +44 7780- 662 800 Contact David Rothschild (Director) E-mail [email protected] Contact Matt Karinen (Director) E-mail [email protected] RSPO Membership No.: 1-0102-11-000-00 Ordinary member Approved 29/08/2011, 1 Figure 1: Location Map of project Area in Tarjuowon District, Sinoe County, Republic of Liberia Figure 2: Location of the proposed Tarjuowon development area and protected areas in Liberia 2 Figure 3: Map of concession showing towns and villages and HCV set-asides in the area 3 1.0 Summary from SEI Assessments In 2010 an oil palm plantation concession agreement was signed between the Government of Liberia and GOLDEN VEROLEUM (LIBERIA) covering five (5) counties in Liberia: Grand Kru, Sinoe, Maryland, Rivercess and Grand Kru for a period of 65 years with an option for renewal. This agreement covers a total of approximately 500,000 acres (220,000 hectares). The concession agreement amongst other things provides for the implementation of a social and community development program, which includes the creation of about 35,000 jobs in 5 counties within a 15 year period, construction of employee housing, education, medical care, a Liberian smallholder program and the construction of about 16 mills and 2 sea ports within 15 years. -

Liberia Education Update May 2019
Liberia Education Update May 2019 Lofa Road on the way to Voinjama City, April 29, 2019. The rains have only just begun. Lofa River District I ended April and began May in the Lofa River District. District Superintendent, Rev. Cecelia Marpleh, and I traveled together in her pick-up truck from Gbarnga in Bong County to visit the Jemima Camp Freeman United Methodist School (UMS) in Voinjama City, Lofa County. I visited Voinjama several times since 2009 as we worked to renovate and reopen the school that was damaged and looted during the war. The school now has 115 students in nursery class through seventh grade. Water for Life built a latrine for the school with a gift from St. Paul’s UMC in Rochester, Michigan. There are 5 students in the 7th grade class and only one of them had a copy of the literature book, Why No One Knows When He Will Die. The need for required textbooks continues in schools throughout Liberia. While in Lofa, we also visited the recently established Foya United Methodist Church (UMC). The congregation speaks the Kisi language, but there was only a copy of the English King James Bible in the church. I was so happy to find a Kisi Bible at the Bible Society book store in Monrovia. I would like everyone to hear and receive the Word in the language they understand best. Back in Foya United Methodist Church, Lofa County Monrovia, I also found a copy of the literature book for April 30, 2019 each student in the 7th grade class. -

HIGH CONSERVATION VALUE PUBLIC SUMMARY Golden Veroleum Liberia’S Barclayville, Grand Cess, Gblebo and Trembo Districts Grand Kru County, Liberia
HIGH CONSERVATION VALUE PUBLIC SUMMARY Golden Veroleum Liberia’s Barclayville, Grand Cess, Gblebo and Trembo Districts Grand Kru County, Liberia . Date of report: June 2016 . Name of lead assessor: Solomon P. Wright . Contact information of lead assessor: Green Consultancy Inc, Abi Joudi Building, Apartment 3 Corner of Gurley & Broad Streets, Monrovia, Liberia . ALS license type: Provisional . Organisation commissioning HCV assessment: Golden Veroleum Liberia C/O David Rothchild, Director Contact: +44-7780-662-800 . Location of assessment: Barclayville, Grand Cess, Gblebo and Trembo Districts in Grand Kru County, Southern Eastern Liberia . Dates of assessment: November 2015 - May 2016 . Size of assessment area: 24,593 ha . Total HCVMA mapped: Finalized HCVMA = 2,097 ha. Draft HCVMA = an additional 1,027 ha mapped. The draft HCVMAs have been identified, described and mapped indicatively where possible, but will require definitive mapping by GVL to be included in the finalized HCVMA. Planned land use(s) for assessment area: Oil palm plantation . Certification scheme: RSPO AOI Area of Interest MOU Memorandum of Understanding CI Conservation International NGO Non-Governmental Organization CDA County Development Agency NPP New Planting Procedure DEM Digital Elevation Model NTFP Non-Forest Timber Product DBH Diameter at Breast Height OL / LT Open Land (an HCS category) ESIA Environmental and Social Impact Assessment RBA Rapid Biodiversity Assessment FCP Forest Conservation Policy RF Regenerating Forest FDA Forestry Development Authority RSPO Round Table on Sustainable Palm Oil FFI Fauna and Flora International SRV Short Regenerating Vegetation FGD Focus Group Discussion S / BM Scrub (an HCS category) FSC Forest Stewardship Council SAMFU Save My Future Foundation GAR Golden Agri-Resources SCNL Society for the Conservation of Nature in Liberia GIS Geographical Information System SOP Standard Operating Procedures GOL Government of Liberia SNF Short Stature Natural Forest GVL Golden Veroleum Liberia Inc. -

Local Government Law
TITLE 20 Local Government Law TABLE OF CONTENTS Chapter Page 1. Territorial Divisions of Liberia 395 2. Counties 395 3. Territories 403 4. Leeward Districts 404 5. Townships 404 Chap. XXXII - Act creating grades of District Commissioners 407 Chap. XXXIII - Act setting up Commission to evaluate regulations of interior service 410 Chap. XXII - Act relating to election of chiefs 411 LIBERIAN CODES REVISED, VOL. IV, PAGE: 394 LOCAL GOVERNMENT LAW Chapter 1. TERRITORIAL DIVISIONS OF LIBERIA § 1. County Area and Hinterland. The territory of the Republic shall be divided for the purpose of administration into the County Area and Hinterland. The County Area shall include all territory extending from the seaboard forty miles inland and from the Mano to the Cavalla Rivers. The Hinterland shall com- mence at the eastern boundary of the County Area; i.e., forty miles inland and extend eastward as far as the recognized limit of the Republic. It shall be bounded on the north by Sierra Leone, and on the south by the Ivory Coast. The Minister of Internal Affairs shall be the chief officer of the local governments of both the County Area and the Hinterland. He shall have power to make from time to time such regulations as are conducive to their successful government, subject to the approval of the President. All complaints concerning their administration shall be made to him, and all reports by their officers shall be submitted to him except where otherwise provided by statute. I Chapter 2. COUNTIES § 10. Division into counties. The County Area of the Republic shall be composed of the counties of Grand Cape Mount, Montserrado, Grand Bassa, Sinoe, and Maryland 2 , Bong, Nimba, Lofa, Grand Gedeh, Bomi, Grand Kru, Margibi, and 1. -

Liberia IDSR Epidemiology Bulletin
ATION N AL P U B L I C Liberia IDSR Epidemiology Bulletin H E A A L I T R 2018 Epi Week 2 (January 8-14, 2018) H E B I I N L S T F I O T U E T 01Country Population: 4,373,279 l Volume 10, Issue 2 Jan. 8-14, 2018 l Data Source: CSOs from 15 Counties and Lab Highlights Keynotes and Events of Public Health Figure 1. Public Health Events Reported in Epi-week 2 Significance A total of 178 suspected cases of immediately reportable diseases and events 26 deaths were reported from 15 counties. These include: o Three confirmed Lassa fever were reported Confirmed Measles outbreaks in Nimba and Montserrado Counties Health facility reporting completeness and timeliness are both 98% Reporting Coverage Table 1. Weekly IDSR Reporting Coverage, Liberia, Epi week 2, 2018 Number of Number Expected Report of Number 751(98%) from Health Reports Received Completeness Timeliness Health facilities County Facility Received on Time (%) (%) out of 759 Bomi 26 26 26 100 100 reported timely Bong 55 49 49 89 89 IDSR data Gbarpolu 15 15 15 100 100 Grand Bassa 33 33 33 100 100 Grand Cape Mount 34 34 34 100 100 91 (100%) Grand Gedeh 24 24 24 100 100 Health Grand Kru 19 19 19 100 100 districts reported IDSR Lofa 59 59 59 100 100 Margibi 44 44 44 100 100 data Maryland 25 25 25 100 100 Montserrado 283 279 279 99 99 Nimba 74 71 71 96 96 751(98%) Health Rivercess 19 19 19 100 100 River Gee 19 19 19 100 100 facilities Sinoe 35 35 35 100 100 reported IDSR data Liberia 764 751 751 98 98 Legend ≥80 <80 Twelve counties submitted weekly IDSR report on time The national target for weekly IDSR reporting is 80% IDSR Weekly Epidemiology and Surveillance Bulletin Page 1 ATION N AL P U B L I C Liberia IDSR Epidemiology Bulletin H E A A L I T R 2018 Epi Week 2 (January 8-14, 2018) H E B I I N L S T F I O T U E T Vaccine Preventable Diseases Measles One Hundred and Five (105) suspected cases were reported from Montserrado (45), Nimba (40), Grand Bassa (4) Bong (4), Margibi (3), Grand Kru (2), Grand Gedeh (2), Maryland (2), Bomi (1), Lofa (1) and Sinoe (1) Counties.