A Systematic Review of Selected Interventions for Worksite Health Promotion the Assessment of Health Risks with Feedback
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Descriptive Statistics (Part 2): Interpreting Study Results
Statistical Notes II Descriptive statistics (Part 2): Interpreting study results A Cook and A Sheikh he previous paper in this series looked at ‘baseline’. Investigations of treatment effects can be descriptive statistics, showing how to use and made in similar fashion by comparisons of disease T interpret fundamental measures such as the probability in treated and untreated patients. mean and standard deviation. Here we continue with descriptive statistics, looking at measures more The relative risk (RR), also sometimes known as specific to medical research. We start by defining the risk ratio, compares the risk of exposed and risk and odds, the two basic measures of disease unexposed subjects, while the odds ratio (OR) probability. Then we show how the effect of a disease compares odds. A relative risk or odds ratio greater risk factor, or a treatment, can be measured using the than one indicates an exposure to be harmful, while relative risk or the odds ratio. Finally we discuss the a value less than one indicates a protective effect. ‘number needed to treat’, a measure derived from the RR = 1.2 means exposed people are 20% more likely relative risk, which has gained popularity because of to be diseased, RR = 1.4 means 40% more likely. its clinical usefulness. Examples from the literature OR = 1.2 means that the odds of disease is 20% higher are used to illustrate important concepts. in exposed people. RISK AND ODDS Among workers at factory two (‘exposed’ workers) The probability of an individual becoming diseased the risk is 13 / 116 = 0.11, compared to an ‘unexposed’ is the risk. -

Risk Factors Associated with Maternal Age and Other Parameters in Assisted Reproductive Technologies - a Brief Review
Available online at www.pelagiaresearchlibrary.com Pelagia Research Library Advances in Applied Science Research, 2017, 8(2):15-19 ISSN : 0976-8610 CODEN (USA): AASRFC Risk Factors Associated with Maternal Age and Other Parameters in Assisted Reproductive Technologies - A Brief Review Shanza Ghafoor* and Nadia Zeeshan Department of Biochemistry and Biotechnology, University of Gujrat, Hafiz Hayat Campus, Gujrat, Punjab, Pakistan ABSTRACT Assisted reproductive technology is advancing at fast pace. Increased use of ART (Assisted reproductive technology) is due to changing living standards which involve increased educational and career demand, higher rate of infertility due to poor lifestyle and child conceivement after second marriage. This study gives an overview that how advancing age affects maternal and neonatal outcomes in ART (Assisted reproductive technology). Also it illustrates how other factor like obesity and twin pregnancies complicates the scenario. The studies find an increased rate of preterm birth .gestational hypertension, cesarean delivery chances, high density plasma, Preeclampsia and fetal death at advanced age. The study also shows the combinatorial effects of mother age with number of embryos along with number of good quality embryos which are transferred in ART (Assisted reproductive technology). In advanced age women high clinical and multiple pregnancy rate is achieved by increasing the number along with quality of embryos. Keywords: Reproductive techniques, Fertility, Lifestyle, Preterm delivery, Obesity, Infertility INTRODUCTION Assisted reproductive technology actually involves group of treatments which are used to achieve pregnancy when patients are suffering from issues like infertility or subfertility. The treatments can involve invitro fertilization [IVF], intracytoplasmic sperm injection [ICSI], embryo transfer, egg donation, sperm donation, cryopreservation, etc., [1]. -
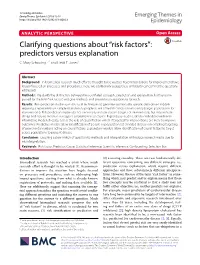
Clarifying Questions About “Risk Factors”: Predictors Versus Explanation C
Schooling and Jones Emerg Themes Epidemiol (2018) 15:10 Emerging Themes in https://doi.org/10.1186/s12982-018-0080-z Epidemiology ANALYTIC PERSPECTIVE Open Access Clarifying questions about “risk factors”: predictors versus explanation C. Mary Schooling1,2* and Heidi E. Jones1 Abstract Background: In biomedical research much efort is thought to be wasted. Recommendations for improvement have largely focused on processes and procedures. Here, we additionally suggest less ambiguity concerning the questions addressed. Methods: We clarify the distinction between two confated concepts, prediction and explanation, both encom- passed by the term “risk factor”, and give methods and presentation appropriate for each. Results: Risk prediction studies use statistical techniques to generate contextually specifc data-driven models requiring a representative sample that identify people at risk of health conditions efciently (target populations for interventions). Risk prediction studies do not necessarily include causes (targets of intervention), but may include cheap and easy to measure surrogates or biomarkers of causes. Explanatory studies, ideally embedded within an informative model of reality, assess the role of causal factors which if targeted for interventions, are likely to improve outcomes. Predictive models allow identifcation of people or populations at elevated disease risk enabling targeting of proven interventions acting on causal factors. Explanatory models allow identifcation of causal factors to target across populations to prevent disease. Conclusion: Ensuring a clear match of question to methods and interpretation will reduce research waste due to misinterpretation. Keywords: Risk factor, Predictor, Cause, Statistical inference, Scientifc inference, Confounding, Selection bias Introduction (2) assessing causality. Tese are two fundamentally dif- Biomedical research has reached a crisis where much ferent questions, concerning two diferent concepts, i.e., research efort is thought to be wasted [1]. -

Unlocking the Power of Pharmacovigilance* an Adaptive Approach to an Evolving Drug Safety Environment
Unlocking the power of pharmacovigilance* An adaptive approach to an evolving drug safety environment PricewaterhouseCoopers’ Health Research Institute Contents Executive summary 01 Background 02 The challenge to the pharmaceutical industry 02 Increased media scrutiny 02 Greater regulatory and legislative scrutiny 04 Investment in pharmacovigilance 05 The reactive nature of pharmacovigilance 06 Unlocking the power of pharmacovigilance 07 Organizational alignment 07 Operations management 07 Data management 08 Risk management 10 The three strategies of effective pharmacovigilance 11 Strategy 1: Align and clarify roles, responsibilities, and communications 12 Strategy 2: Standardize pharmacovigilance processes and data management 14 Strategy 3: Implement proactive risk minimization 20 Conclusion 23 Endnotes 24 Glossary 25 Executive summary The idea that controlled clinical incapable of addressing shifts in 2. Standardize pharmacovigilance trials can establish product safety public expectations and regulatory processes and data management and effectiveness is a core principle and media scrutiny. This reality has • Align operational activities across of the pharmaceutical industry. revealed issues in the four areas departments and across sites Neither the clinical trials process involved in patient safety operations: • Implement process-driven standard nor the approval procedures of the organizational alignment, operations operating procedures, work U.S. Food and Drug Administration management, data management, and instructions, and training -

Epidemiology of and Risk Factors for COVID-19 Infection Among Health Care Workers: a Multi-Centre Comparative Study
International Journal of Environmental Research and Public Health Article Epidemiology of and Risk Factors for COVID-19 Infection among Health Care Workers: A Multi-Centre Comparative Study Jia-Te Wei 1, Zhi-Dong Liu 1, Zheng-Wei Fan 2, Lin Zhao 1,* and Wu-Chun Cao 1,2,* 1 Institute of EcoHealth, School of Public Health, Cheeloo College of Medicine, Shandong University, Jinan 250012, Shandong, China; [email protected] (J.-T.W.); [email protected] (Z.-D.L.) 2 State Key Laboratory of Pathogen and Biosecurity, Beijing Institute of Microbiology and Epidemiology, Beijing 100071, China; [email protected] * Correspondence: [email protected] (L.Z.); [email protected] (W.-C.C.) Received: 31 August 2020; Accepted: 28 September 2020; Published: 29 September 2020 Abstract: Healthcare workers (HCWs) worldwide are putting themselves at high risks of coronavirus disease 2019 (COVID-19) by treating a large number of patients while lacking protective equipment. We aim to provide a scientific basis for preventing and controlling the COVID-19 infection among HCWs. We used data on COVID-19 cases in the city of Wuhan to compare epidemiological characteristics between HCWs and non-HCWs and explored the risk factors for infection and deterioration among HCWs based on hospital settings. The attack rate (AR) of HCWs in the hospital can reach up to 11.9% in Wuhan. The time interval from symptom onset to diagnosis in HCWs and non-HCWs dropped rapidly over time. From mid-January, the median time interval of HCW cases was significantly shorter than in non-HCW cases. -

Understanding Risk & Protective Factors for Suicide
Understanding Risk and Protective Factors for Suicide: A Primer for Preventing Suicide Risk and protective factors play a critical role in suicide prevention. For clinicians, identifying risk and protective factors provides critical information to assess and manage suicide risk in individuals. For communities and prevention programs, identifying risk and protective factors provides direction about what to change or promote. Many lists of risk factors are available throughout the field of suicide prevention. This paper provides a brief overview of the importance of risk and protective factors as they relate to suicide and offers guidance about how communities can best use them to decrease suicide risk. Contents: What are risk and protective factors? Risk factors are not warning signs. What are major risk and protective factors for suicide? Why are risk and protective factors important? Using risk and protective factors in the strategic planning process Key points about risk and protective factors for suicide prevention Additional resources Further reading References What are risk and protective factors? Risk factors are characteristics that make it more likely that individuals will consider, attempt, or die by suicide. Protective factors are characteristics that make it less likely that individuals will consider, attempt, or die by suicide. Risk and protective factors are found at various levels: individual (e.g., genetic predispositions, mental disorders, personality traits), family (e.g., cohesion, dysfunction), and community (e.g., availability of mental health services). They may be fixed (those things that cannot be changed, such as a family history of suicide) or modifiable (those things that can be changed, such as depression). -

The Global Occupational Health Network ISSUE No
The Global Occupational Health Network ISSUE No. 6WINTER 2003 GOHNETGOHNET GOHNET NEWSLETTER Dear GOHNET members and future members, From Workplace Health Promotion The 6th GOHNET Newsletter treats the topic of workplace health to Integrative Workplace Health promotion (WHP). WHP has a history of a few decades. In the Management: 1970s the concept focused on changing a single lifestyle habit or behaviour of the individual. The 1980s were dominated by more Trends and Development comprehensive wellness programmes at work, but still focused on the Cordia Chu ([email protected]), School of Public Health, individual. The 1990s brought an interdisciplinary approach involving Griffith University, Australia for the first time workers and management collectively trying to create a health-promoting workplace. The scope of work issues addressed cover environmental, social, ergonomic, and organisational work issues, In the last two decades, despite some very important advances as well as individual, family and community health issues. The trend by international agencies, governments, industries, unions and is to view the worker in a holistic manner and not in a purely medical academics, workplace fatalities, injuries and illnesses remain at way as is the case in most occupational health services today. unacceptably high levels. Developing nations are facing increasing health risks imposed by rapid industrialization and globalization WHP can be effective when the programme is well designed. WHP while developed nations are encountering problems -

Risk Factors
Chapter 3 Risk factors this page is intentionally blank Chief Medical Officer’s Report 2011 193 Chapter 3 – Overview Risk factors An understanding of the causal factors underlying patterns Tobacco use, for example, is the primary cause of early There is evidence that these proportions are falling, albeit at of health and well-being in the population is key to the death and ill health in England. Public health policies have a different rate across the socioeconomic gradient. But to commissioning and delivery of effective public health services. contributed to a progressive reduction in smoking rates effectively support people to make the change towards more in recent decades through a combination of measures healthy lives, those commissioning and delivering health Early death and disability do not occur in isolation: they are to regulate the promotion and supply of tobacco, and services need to recognise not only the varying prevalence of mediated through a complex interplay of social, economic to help smokers quit. Nevertheless, many young people, individual risk factors across groups in the population and the and environmental factors, as well as by individual specific particularly those from more deprived backgrounds and from life course, but also that the majority of people have multiple determinants of health. This chapter focuses on the risks to some ethnic groups, continue to be exposed to second- risks to their health. health presented by the lifestyles that people lead: factors hand smoke at home; many go on to become smokers such as smoking, poor diet and high risk alcohol consumption themselves because they perceive it to be a normal part of Fair Society, Healthy Lives notes that only 4% of NHS funding collectively constitute some of the most important direct adult life3. -
Introduction to Public Health Instructor Name Title Organization
Public Health 101 Series Introduction to Public Health Instructor name Title Organization Note: This slide set is in the public domain and may be customized as needed by the user for informational or educational purposes. Permission from the Centers for Disease Control and Prevention is not required, but citation of the source is appreciated. Course Topics Introduction to Public Health 1. Public Health Definition and Key Terms 2. History of Public Health 3. A Public Health Approach 4. Core Functions and Essential Services of Public Health 5. Stakeholder Roles in Public Health 6. Determining and Influencing the Public’s Health 2 Learning Objectives After this course, you will be able to • describe the purpose of public health • define key terms used in public health • identify prominent events in the history of public health • recognize the core public health functions and services • describe the role of different stakeholders in the field of public health • list some determinants of health • recognize how individual determinants of health affect population health 3 Topic 1 Public Health Definition and Key Terms 4 Public Health Defined “The science and art of preventing disease, prolonging life, and promoting health through the organized efforts and informed choices of society, organizations, public and private communities, and individuals.” —CEA Winslow Photo: IF Fisher and EL Fisk Winslow CEA. The untilled field of public health. Mod Med 1920;2:183–91. 5 The Mission of Public Health “Fulfilling society’s interest in assuring conditions in which people can be healthy.” —Institute of Medicine “Public health aims to provide maximum benefit for the largest number of people.” —World Health Organization 6 Public Health Key Terms clinical care: prevention, treatment, and management of illness and the preservation of mental and physical well-being through the services offered by medical and allied health professions; also known as health care. -
Good Pharmacovigilance Practices for the Americas ISBN 978-92-75-13160-2 PANDRH Technical Document Nº 5 Pan American Network on Drug Regulatory Harmonization
PANDRH Technical Document Nº 5 Pan American Network on Drug Regulatory Harmonization PANDRH Technical Document Nº 5 Technical PANDRH Working Group on Pharmacovigilance Good Pharmacovigilance Good Pharmacovigilance Practices for the Americas Good Pharmacovigilance Practices for the Practices for the Americas ISBN 978-92-75-13160-2 PANDRH Technical Document Nº 5 Pan American Network on Drug Regulatory Harmonization Worki ng Group on Pharmacov iigil ilance Good Pharmacovigilance Practices for the Americas Washington, DC June 2011 PAHO Headquarters Library – Catalogued at the source Pan American Health Organization. “Good Pharmacovigilance Practices for the Americas”. Washington, D.C.: PAHO, © 2011. (PANDRH Technical Document Nº 5). 73 p. ISBN 978-92-75-13160-2 Published in Spanish with the title: “Buenas Prácticas de Farmacovigilancia para las Américas” Published in Portuguese with the title: “Boas práticas de farmacovigilância para as Américas” I Title 1. PHARMACOEPIDEMIOLOGY – legislation and jurisprudence 2. NATIONAL HEALTH SURVEILLANCE SYSTEM 3. PHARMACEUTICAL LEGISLATION – standards 4. DRUG LEGISLATION – economics 5. DRUGS AND NARCOTICS CONTROL 6. HEALTH POLICIES 7. AMERICAS NLM QV 733.DA1 Approved by the V PANDRH Conference in 2008. Validated in 2010. © Pan American Health Organization, 2011 All rights reserved. Requests for this publication should be directed to the Area of Health Systems based on Primary Health Care, Project on Essential Medicines and Technologies, Pan American Health Organization / World Health Organization, 525 23rd St., NW, Washington, D.C., USA [phone: +(202) 974-3483; e-mail: cas- [email protected]]. Requests for authorization to reproduce or translate PAHO publications—whether for sale or noncommercial distribution—should be directed to the Area of Knowledge Management and Communications (KMC) at the above address [fax: +(202) 974-3652; e-mail: [email protected]]. -

American College of Sports Medicine (ACSM) Risk Factor Screening January 5, 2015 Written by Jefrey W
American College of Sports Medicine (ACSM) Risk Factor Screening January 5, 2015 Written By Jefrey W. Ryg, PT, DPT, OCS, FAAOMPT, ATC, CSCS Te Functional Movement Screen (FMS) is utilized to iden- individuals with underlying heart disease, ofen without tify healthy individuals at risk for future injury in sports. signs and symptoms, or among those who initiate vigorous Tis series of seven tests assists Physical Terapists in their exercise from a sedentary lifestyle. In younger athletes, <30 identifcation and treatment of known musculoskeletal risk in males and <40 in females, the underlying cause of cardio- factors prior to participation. In addition, to the musculo- vascular injury is likely congenital in nature (heart defect, skeletal screenings, the of season also allows us to screen arrythmias) and our ability to accurately screen these causes the cardiovascular system in order to prevent illness, disease with a participation exam is debateable in the literature. or injury. Fortunately, these events in younger athletes are rare approximately 1 event in 133,000 and 769,000 men and Te Centers for Disease Control, American College of women, respectively3. Te American Heart Association Sports Medicine (ACSM) and American Heart Association recommends cardiovascular screening for high school and recommend >5 days of week of moderate or >3 days per college age individuals at 2 and 4 year intervals or more week vigorous cardiorespiratory (aerobic) exercise per week frequently for individuals with known disease. to improve ftness and reduce risk of illness and disease1. Specifcally, this dosage of exercise has been shown to As we age our risk for cardiovascular events reduce all cause mortality and reduce the risk of developing (males>females) with exercise increases, regardless of other coronary heart disease, stroke, type 2 diabetes, and cancer1. -

7 Epidemiology: a Tool for the Assessment of Risk
7 Epidemiology: a tool for the assessment of risk Ursula J. Blumenthal, Jay M. Fleisher, Steve A. Esrey and Anne Peasey The purpose of this chapter is to introduce and demonstrate the use of a key tool for the assessment of risk. The word epidemiology is derived from Greek and its literal interpretation is ‘studies upon people’. A more usual definition, however, is the scientific study of disease patterns among populations in time and space. This chapter introduces some of the techniques used in epidemiological studies and illustrates their uses in the evaluation or setting of microbiological guidelines for recreational water, wastewater reuse and drinking water. 7.1 INTRODUCTION Modern epidemiological techniques developed largely as a result of outbreak investigations of infectious disease during the nineteenth century. © 2001 World Health Organization (WHO). Water Quality: Guidelines, Standards and Health. Edited by Lorna Fewtrell and Jamie Bartram. Published by IWA Publishing, London, UK. ISBN: 1 900222 28 0 136 Water Quality: Guidelines, Standards and Health Environmental epidemiology, however, has a long history dating back to Roman and Greek times when early physicians perceived links between certain environmental features and ill health. John Snow’s study of cholera in London and its relationship to water supply (Snow 1855) is widely considered to be the first epidemiological study (Baker et al. 1999). Mapping cases of cholera, Snow was able to establish that cases of illness were clustered in the streets close to the Broad Street pump, with comparatively few cases occurring in the vicinity of other local pumps. Epidemiological investigations can provide strong evidence linking exposure to the incidence of infection or disease in a population.