Myoglobin and Creatine Kinase in Acute Myocardial Infarction
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Myoglobin Expression Under Hypoxic Condtions In
THESIS IN THE FACE OF HYPOXIA: MYOGLOBIN EXPRESSION UNDER HYPOXIC CONDTIONS IN CULTURED WEDDELL SEAL SKELETAL MUSCLE CELLS Submitted by Michael Anthony De Miranda Jr. Department of Biology In partial fulfillment of the requirements For the degree of Master of Science Colorado State University Fort Collins, Colorado Spring 2012 Master’s Committee: Advisor: Shane Kanatous Gregory Florant Scott Earley Copyright by Michael A. De Miranda Jr. 2012 All Rights Reserved ABSTRACT IN THE FACE OF HYPOXIA: MYOGLOBIN EXPRESSION UNDER HYPOXIC CONDITIONS IN CULTURED WEDDELL SEAL SKELETAL MUSCLE CELLS The hallmark adaptation to breath-hold diving in Weddell seals (Leptonychotes weddellii) is enhanced concentrations of myoglobin in their skeletal muscles. Myoglobin is a cytoplasmic hemoprotein that stores oxygen for use in aerobic metabolism throughout the dive duration. In addition, throughout the duration of the dive, Weddell seals rely on oxygen stored in myoglobin to sustain aerobic metabolism in which lipid is the primary contributor of acetyl CoA for the citric acid cycle. Together, enhanced myoglobin concentrations and a lipid-based aerobic metabolism represent some of the unique adaptations to diving found in skeletal muscle of Weddell seals. This thesis presents data that suggests cultured Weddell seal skeletal muscle cells inherently possess adaptations to diving such as increased myoglobin concentrations, and rely on lipids to fuel aerobic metabolism. I developed the optimum culture media for this unique primary cell line based on myoblast confluence, myoblast growth rates, myotube counts, and myotube widths. Once the culture media was established, I then determined the de novo expression of myoglobin under normoxic and hypoxic oxygen conditions and the metabolic profile of the myotubes under each oxygen condition. -

Myoglobin from Equine Skeletal Muscle
Myoglobin from equine skeletal muscle Catalog Number M0630 Storage Temperature –20 C CAS RN 100684-32-0 Precautions and Disclaimer This product is for R&D use only, not for drug, Product Description household, or other uses. Please consult the Safety Molecular mass:1 17.6 kDa Data Sheet for information regarding hazards and safe Extinction coefficient:2 EmM = 12.92 (555 nm) handling practices. pI:3 7.3 (major component) and 6.8 (minor component) Preparation Instructions Myoglobin from horse skeletal muscle is a single chain This protein is soluble in water (10 mg/ml), yielding a heme protein containing 153 amino acid residues. It clear, red brown solution. posesses no disulfide bridges or free -SH groups. Myoglobin contains 8 variously sized right-handed References helical regions, joined by non-ordered or random coil 1. Darbre, P.D. et al., Comparison of the myoglobin of regions. These 8 helices (A, B, C, D, E, F, G, and H) the zebra (Equus burchelli) with that of the horse are folded back on top of one another, and the heme is (Equus cabalus). Biochim. Biophys. Acta, 393(1), situated between helices E and F. The heme is almost 201-204 (1975). totally buried. Only the edge carrying the two 2. Bowen, W.J., The absorption spectra and extinction hydrophylic propionic acid groups is exposed. The coefficients of myoglobin. J. Biol. Chem., 179, 235- heme is held in position by a coordinating complex 245 (1949). between the central Fe(II) atom and 2 histidine residues 3. Radola, B.J., Isoelectric focusing in layers of (on helices E and F, respectively). -

A Short Review of Iron Metabolism and Pathophysiology of Iron Disorders
medicines Review A Short Review of Iron Metabolism and Pathophysiology of Iron Disorders Andronicos Yiannikourides 1 and Gladys O. Latunde-Dada 2,* 1 Faculty of Life Sciences and Medicine, Henriette Raphael House Guy’s Campus King’s College London, London SE1 1UL, UK 2 Department of Nutritional Sciences, School of Life Course Sciences, King’s College London, Franklin-Wilkins-Building, 150 Stamford Street, London SE1 9NH, UK * Correspondence: [email protected] Received: 30 June 2019; Accepted: 2 August 2019; Published: 5 August 2019 Abstract: Iron is a vital trace element for humans, as it plays a crucial role in oxygen transport, oxidative metabolism, cellular proliferation, and many catalytic reactions. To be beneficial, the amount of iron in the human body needs to be maintained within the ideal range. Iron metabolism is one of the most complex processes involving many organs and tissues, the interaction of which is critical for iron homeostasis. No active mechanism for iron excretion exists. Therefore, the amount of iron absorbed by the intestine is tightly controlled to balance the daily losses. The bone marrow is the prime iron consumer in the body, being the site for erythropoiesis, while the reticuloendothelial system is responsible for iron recycling through erythrocyte phagocytosis. The liver has important synthetic, storing, and regulatory functions in iron homeostasis. Among the numerous proteins involved in iron metabolism, hepcidin is a liver-derived peptide hormone, which is the master regulator of iron metabolism. This hormone acts in many target tissues and regulates systemic iron levels through a negative feedback mechanism. Hepcidin synthesis is controlled by several factors such as iron levels, anaemia, infection, inflammation, and erythropoietic activity. -

Delayed Onset Muscle Soreness in People with Diabetes; Biomarkers and Nutritional Supplementation Hani H
Loma Linda University TheScholarsRepository@LLU: Digital Archive of Research, Scholarship & Creative Works Loma Linda University Electronic Theses, Dissertations & Projects 12-1-2011 Delayed Onset Muscle Soreness in People with Diabetes; Biomarkers and Nutritional Supplementation Hani H. Al-Nakhli Loma Linda University Follow this and additional works at: http://scholarsrepository.llu.edu/etd Part of the Rehabilitation and Therapy Commons Recommended Citation Al-Nakhli, Hani H., "Delayed Onset Muscle Soreness in People with Diabetes; Biomarkers and Nutritional Supplementation" (2011). Loma Linda University Electronic Theses, Dissertations & Projects. 19. http://scholarsrepository.llu.edu/etd/19 This Dissertation is brought to you for free and open access by TheScholarsRepository@LLU: Digital Archive of Research, Scholarship & Creative Works. It has been accepted for inclusion in Loma Linda University Electronic Theses, Dissertations & Projects by an authorized administrator of TheScholarsRepository@LLU: Digital Archive of Research, Scholarship & Creative Works. For more information, please contact [email protected]. Loma Linda University School of Allied Health Professions in conjunction with the Faculty of Graduate Studies _____________________ Delayed Onset Muscle Soreness in People with Diabetes; Biomarkers and Nutritional Supplementation by Hani H. Al-Nakhli _____________________ A Dissertation submitted in partial satisfaction of the requirements for the degree Doctor of Philosophy in Rehabilitations Science _____________________ December, 2011 © 2011 Hani H. Al-Nakhli All Right Reserved Each person whose signature appears below certifies that this dissertation in his/her opinion is adequate, in scope and quality, as a dissertation for the degree Doctor of Philosophy. , Chairperson Jerrold S. Petrofsky, Professor of Physical Therapy, Director of Research Lee S. Berk, Associate Professor of Physical Therapy Richard Hubbard, Professor of Pathology Michael S. -

Attenuation of Glucose-Induced Myoglobin Glycation and the Formation of Advanced Glycation End Products (Ages) by (R)-Α-Lipoic Acid in Vitro
biomolecules Article Attenuation of Glucose-Induced Myoglobin Glycation and the Formation of Advanced Glycation End Products (AGEs) by (R)-α-Lipoic Acid In Vitro Hardik Ghelani 1,2, Valentina Razmovski-Naumovski 1,2,3, Rajeswara Rao Pragada 4 and Srinivas Nammi 1,2,* ID 1 School of Science and Health, Western Sydney University, Sydney, NSW 2751, Australia; [email protected] (H.G.); [email protected] (V.R.-N.) 2 National Institute of Complementary Medicine (NICM), Western Sydney University, Sydney, NSW 2751, Australia 3 South Western Sydney Clinical School, School of Medicine, University of New South Wales, Sydney, NSW 2052, Australia 4 Department of Pharmacology, College of Pharmaceutical Sciences, Andhra University, Visakhapatnam 530003, Andhra Pradesh, India; [email protected] * Correspondence: [email protected]; Tel.: +61-2-4620-3038; Fax: +61-2-4620-3025 Received: 1 December 2017; Accepted: 1 February 2018; Published: 8 February 2018 Abstract: High-carbohydrate containing diets have become a precursor to glucose-mediated protein glycation which has been linked to an increase in diabetic and cardiovascular complications. The aim of the present study was to evaluate the protective effect of (R)-α-lipoic acid (ALA) against glucose-induced myoglobin glycation and the formation of advanced glycation end products (AGEs) in vitro. Methods: The effect of ALA on myoglobin glycation was determined via the formation of AGEs fluorescence intensity, iron released from the heme moiety of myoglobin and the level of fructosamine. The extent of glycation-induced myoglobin oxidation was measured via the levels of protein carbonyl and thiol. Results: The results showed that the co-incubation of ALA (1, 2 and 4 mM) with myoglobin (1 mg/mL) and glucose (1 M) significantly decreased the levels of fructosamine, which is directly associated with the decrease in the formation of AGEs. -
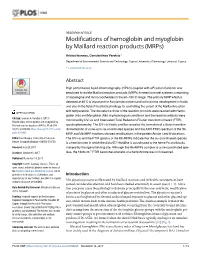
Modifications of Hemoglobin and Myoglobin by Maillard Reaction Products (Mrps)
RESEARCH ARTICLE Modifications of hemoglobin and myoglobin by Maillard reaction products (MRPs) Aristos Ioannou, Constantinos Varotsis* Department of Environmental Science and Technology, Cyprus University of Technology, Limassol, Cyprus * [email protected] a1111111111 a1111111111 Abstract a1111111111 High performance liquid chromatography (HPLC) coupled with a Fraction Collector was a1111111111 a1111111111 employed to isolate Maillard reaction products (MRPs) formed in model systems comprising of asparagine and monosaccharides in the 60±180ÊC range. The primary MRP which is detected at 60ÊC is important for Acrylamide content and color/aroma development in foods and also in the field of food biotechnology for controlling the extent of the Maillard reaction with temperature. The discrete fractions of the reaction products were reacted with Hemo- OPEN ACCESS globin (Hb) and Myoglobin (Mb) at physiological conditions and the reaction adducts were Citation: Ioannou A, Varotsis C (2017) monitored by UV-vis and Attenuated Total Reflection-Fourier transform infrared (FTIR) Modifications of hemoglobin and myoglobin by Maillard reaction products (MRPs). PLoS ONE spectrophotometry. The UV-vis kinetic profiles revealed the formation of a Soret transition 12(11): e0188095. https://doi.org/10.1371/journal. characteristic of a low-spin six-coordinated species and the ATR-FTIR spectrum of the Hb- pone.0188095 MRP and Mb-MRP fractions showed modifications in the protein Amide I and II vibrations. Editor: Ram Nagaraj, University of Colorado The UV-vis and the FTIR spectra of the Hb-MRPs indicate that the six-coordinated species Denver School of Medicine, UNITED STATES is a hemichrome in which the distal E7 Histidine is coordinated to the heme Fe and blocks Received: July 24, 2017 irreversibly the ligand binding site. -

Hemoglobin/Myoglobin Robert F.Diegelmann, Ph.D
Hemoglobin/Myoglobin Robert F.Diegelmann, Ph.D. OBJECTIVES 1. Describe the interactions of heme, globins and oxygen. 2. Discuss the mechanism responsible for SickleCell Anemia. 3. Understand the clinical significance of A1C hemoglobin. 4. Describe the basic biochemical mechanisms of O2 delivery & CO2 removal. RECOMMENDED RESOURCES Lehninger, Principles of Biochemistry, 5th edition, Chapter 5 Molecular Cell Biology, 5th edition; Lodish et al., page 67 http://web.indstate.edu/thcme/mwking/hemoglobinmyoglobin.html#hemoglobin Myoglobin (muscle) & Hemoglobin (Red Blood Cells) were the first proteins for which three dimensional structures were determined. Professor Max Perutz and his colleagues at Cambridge University determined Hemoglobin’s three dimensional structure in the late 1950s Therefore Hemoglobin is one of the most studied & best understood proteins. Figure 1. The Evolution of the Globin protein family Figure 2. Structural similarity of the Globin proteins Figure 3 Below is the basic heme group structure. It consists of a complex organic ring structure named Protoporphyrin. NOTE: Heme metabolism will be covered in more detail in another lecture. Protoporphyrin prosthetic group Porphyrin ring Fe binding site Methene bridge Substitution sites Figure 4 Oxygen is not very soluble in aqueous solutions and therefore needs a special molecule to be carried to tissues and cells. The Protoporphyrin ring structure of Heme binds a single iron atom in its ferrous (Fe 2+) . The iron atom has six coordination bonds, four are found bound to the nitrogens in the Porphyrin ring system and two additional sites perpendicular to the Porphyrin. The Cytochromes (a, b & c) are proteins that also consist of porphyrin structures. -

Managed Care & Healthcare Communications
n TRENDS FROM THE FIELD n Antiquated Tests Within the Clinical Pathology Laboratory Alan H. B. Wu, PhD; Kent Lewandrowski, MD; Ann M. Gronowski, PhD; David G. Grenache, PhD; Lori J. Sokoll, PhD; and Barbarajean Magnani, PhD, MD iven the current economic climate for medical practices, it Objective: To provide evidence supporting the discontinuation of laboratory tests that do not is the responsibility of clinical laboratory directors in hos- have clinical utility today. G pitals and medical centers to review their test menu and, Study Design: We selected 10 representative tests in collaboration with their clinical staff leaders, remove tests that do considered antiquated by most experts in the clinical laboratory medicine field: creatine kinase- not provide clinical value to a particular medical practice, whether MB, myoglobin, serum folate and red blood cell such testing is conducted in-house or sent to a reference laboratory. folate, amylase, lecithin/sphingomyelin ratio, qualitative serum human chorionic gonadotropin, However, many physicians who are experienced with the use of older prostatic acid phosphatase, bleeding time, and tests may resist adoption of newer technologies even if the tests have erythrocyte sedimentation rate. been shown to have superior clinical value or are recommended in Methods: Published literature was reviewed to provide evidence of the poor performance and/ contemporary clinical guidelines. Changing the testing menu can be or limited clinical utility of these tests. When a difficult process and should involve laboratorians and the medical available, subscriptions to the Proficiency Testing Program of the College of American Pathologists staff, especially the staff who frequently order the tests that are to were tracked from 1993 to 2008 as supporting be eliminated. -
Iron Overload and Iron Chelation: the Inside Story
Iron Overload and Iron Chelation: The Inside Story Jerry L. Spivak, MD Professor of Medicine and Oncology Johns Hopkins University School of Medicine Baltimore, Maryland [email protected] Iron as a Prosthetic Group • Oxygen transport - Hemoglobin, myoglobin • Cell proliferation - Ribonucleotide reductase • Electron transport - Flavoproteins • Respiratory enzymes - Cytochromes • Oxidases - Catalase • Reductases - Cytochromes Body Iron Stores (♂) Hemoglobin 2.5 gm Myoglobin/heme and nonheme 0.4 gm enzymes Ferritin/hemosiderin 1.0 gm(2/1ratio) Transferrin 0.005 gm There is no normal mechanism for iron excretion above physiologic losses “Tales From the Crypt” Iron Absorption and the Mucosal Iron Block Stomach Sugars, Duodenum pHamino acids pH and Vitamin C Fe++ Heme-Fe Fe +++ Dctyd (ferri-reductase) Heme-Fe Mature enterocyte DMT1 HCP-1 Ferritin Fe++ Fe+++ Mitochondria Hephaestin FPN (Hepcidin) Other processes Plasma transferrin Enterocyte precursor Enterocyte precursor (Macrophage) (Macrophage) Noniron-loaded Iron-loaded FPN (Ceruloplasmin) Ferritin/Fe++ Fe+++ Fe++ Hepcidin Other cells Iron Balance in Adults Gastrointestinal Absorption 1-2 mg/day Storage Iron Functional iron Liver cells and 18 mg Plasma transferrin Bone marrow Macrophages 4 mg Red cell hemoglobin 1000 mg Myoglobin Cytochromes 2500 mg Physiologic daily iron loss 1-2 mg/day Natural Modifiers of Iron Absorption Iron Absorption Inhibitors Spinach ,whole grains such as buckwheat and amaranth, other vegetables such as chard and rhubarb, as well as beans and nuts, all contain significant levels of oxalic acid, which binds with iron, inhibiting its absorption. Soy beans contain phytic acid, which also bind iron. Tea and coffee contain tannins, which block iron absorption. Clay and heavy metals also inhibit iron absorption. -

Liver Parameters As Part of a Non-Invasive Model for Prediction of All-Cause Mortality After Myocardial Infarction
Clinical research Liver parameters as part of a non-invasive model for prediction of all-cause mortality after myocardial infarction Theodor Baars1, Jan-Peter Sowa2, Ursula Neumann3, Stefanie Hendricks1, Mona Jinawy1, Julia Kälsch2, Guido Gerken2, Tienush Rassaf1, Dominik Heider3,4, Ali Canbay2 1Department for Cardiology, West German Heart and Vascular Centre Essen, Corresponding author: University Hospital, University Duisburg-Essen, Essen, Germany Prof. Ali Canbay MD 2Department of Gastroenterology and Hepatology, University Hospital, Department University Duisburg-Essen, Essen, Germany of Gastroenterology 3Department of Bioinformatics, Straubing Center of Science, University of Applied and Hepatology Science Weihenstephan-Triesdorf, Straubing, Germany University Hospital 4Department of Mathematics and Computer Science, University of Marburg, Marburg, University Duisburg-Essen Germany Leipzigerstr. 44 39120 Magdeburg Submitted: 9 June 2017 Essen, Germany Accepted: 29 June 2017 Phone: +49 3916713100 E-mail: ali.canbay@med. Arch Med Sci 2020; 16 (1): 71–80 ovgu.de DOI: https://doi.org/10.5114/aoms.2018.75678 Copyright © 2018 Termedia & Banach Abstract Introduction: Liver parameters are associated with cardiovascular disease risk and severity of stenosis. It is unclear whether liver parameters could predict the long-term outcome of patients after acute myocardial infarction (AMI). We performed an unbiased analysis of the predictive value of serum parameters for long-term prognosis after AMI. Material and methods: In a retrospective, observational, single-center, cohort study, 569 patients after AMI were enrolled and followed up until 6 years for major adverse cardiovascular events, including cardiac death. Patients were classified into non-survivors (n = 156) and survivors (n = 413). Demographic and laboratory data were analyzed using ensemble feature se- lection (EFS) and logistic regression. -

Review Myoglobin's Old and New Clothes
2713 The Journal of Experimental Biology 213, 2713-2725 © 2010. Published by The Company of Biologists Ltd doi:10.1242/jeb.043075 Review Myoglobin’s old and new clothes: from molecular structure to function in living cells Gerolf Gros1,*, Beatrice A. Wittenberg2,* and Thomas Jue3,*,† With an introduction and perspectives by Jonathan Wittenberg 1Zentrum Physiologie, Medizinische Hochschule Hannover, 30625 Hannover, Germany, 2Department of Physiology and Biophysics, Albert Einstein College of Medicine, Bronx, NY 10461, USA and 3Biochemistry and Molecular Medicine University of California Davis, Davis, CA 95616-8635, USA *These authors contributed equally to this work †Author for correspondence ([email protected]) Accepted 4 April 2010 Summary Myoglobin, a mobile carrier of oxygen, is without a doubt an important player central to the physiological function of heart and skeletal muscle. Recently, researchers have surmounted technical challenges to measure Mb diffusion in the living cell. Their observations have stimulated a discussion about the relative contribution made by Mb-facilitated diffusion to the total oxygen flux. The calculation of the relative contribution, however, depends upon assumptions, the cell model and cell architecture, cell bioenergetics, oxygen supply and demand. The analysis suggests that important differences can be observed whether steady- state or transient conditions are considered. This article reviews the current evidence underlying the evaluation of the biophysical parameters of myoglobin-facilitated oxygen diffusion in cells, specifically the intracellular concentration of myoglobin, the intracellular diffusion coefficient of myoglobin and the intracellular myoglobin oxygen saturation. The review considers the role of myoglobin in oxygen transport in vertebrate heart and skeletal muscle, in the diving seal during apnea as well as the role of the analogous leghemoglobin of plants. -

Myoglobin & Hemoglobin
Myoglobin && Hemoglobin Myoglobin, hemoglobin, cytochromes, catalase & tryptophan pyrrolase are hemoporteins. The heme present in myoglobin & hemoglobin is cyclic tetrapyrol compound contains iron in the ferrous state( Fe+2), this iron has six coordination positions, four of them bind to the four nitrogen atoms of pyrrole in a same plane while the fifth & sixth coordination positions are directed perpendicular to & directly above & below the plane of the heme ring. Oxidation of Fe+2 of myoglobin & hemoglobin to Fe+3 destroys their biological activity. Cyanide & carbon monoxide kill the human because they disrupt the physiologic function of the hemoprotein like cytochrome oxidase & hemoglobin. Biological function of hemoglobin & myoglobin Myoglobin store oxygen in the heart & skeletal muscles as a reserve against oxygen deprivation while hemoglobin transport O2 to the tissues & returns CO2 & protons to the lung. Myoglobin Myoglobin is a hemoprotein present in the heart & skeletal muscles that store oxygen as a reserve against oxygen deprivation. Its globin fraction is a monomer (monomeric protein) consists from 153- aminoacyl residue folds in eight α-helices conformation forming a compact shape of myoglobin ((globular protein)), each helix contains 7-20 aminoacyl residues, starting from amino terminal these helices are termed A-H. As any other globular protein the surface of myoglobin is polar with only two exceptions ((Histidines at E7 & F8 location)) while the interior contains only nonpolar residues. The heme of myoglobin lies in a crevice between E & F helices with a fifth coordination position of the iron is linked to nitrogen of proximal histidine((His F8)) while the distal histidine ((His E7)) lies on the side of the heme ring opposite to His F8.