Quantum of Effectiveness Evidence in FDA's Approval of Orphan Drugs
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

List of Covered Drugs
List of Covered Drugs Effective July 1, 2016 INTRODUCTION We are pleased to provide the 2011 Gold Coast Health Plan List of Covered Drugs as a useful reference and informational tool. The GCHP List of Covered Drugs can assist practitioners in selecting clinically appropriate and cost effective products for their patients. The information contained in the GCHP List of Covered Drugs is provided solely for the convenience of medical providers. We do not warrant or assure accuracy of such information nor is it intended to be comprehensive in nature. This List of Covered Drugs is not intended to be a substitute for the knowledge, expertise, skill and judgment of the medical provider in his or her choice of prescription drugs. All the information in this List of Covered Drugs is provided as a reference for drug therapy selection. Specific drug selection for an individual patient rests solely with the prescriber. We assume no responsibility for the actions or omissions of any medical provider based upon reliance, in whole or in part, on the information contained herein. The medical provider should consult the drug manufacturer's product literature or standard references for more detailed information. National guidelines can be found on the National Guideline Clearinghouse site at http://www.guideline.gov PREFACE The GCHP List of Covered Drugs is organized by sections. Each section is divided by therapeutic drug class primarily defined by mechanism of action. Unless exceptions are noted, generally all applicable dosage forms and strengths of the drug cited are included in the GCHP List of Covered Drugs. Generics should be considered the first line of prescribing. -

Carbon Monoxide Down-Regulates Α4β1 Integrin
Chigaev et al. BMC Immunology 2014, 15:52 http://www.biomedcentral.com/1471-2172/15/52 RESEARCH ARTICLE Open Access Carbon monoxide down-regulates α4β1 integrin-specific ligand binding and cell adhesion: a possible mechanism for cell mobilization Alexandre Chigaev1,2,3*, Yelena Smagley1,2,3 and Larry A Sklar1,2,3 Abstract Background: Carbon monoxide (CO), a byproduct of heme degradation, is attracting growing attention from the scientific community. At physiological concentrations, CO plays a role as a signal messenger that regulates a number of physiological processes. CO releasing molecules are under evaluation in preclinical models for the management of inflammation, sepsis, ischemia/reperfusion injury, and organ transplantation. Because of our discovery that nitric oxide signaling actively down-regulates integrin affinity and cell adhesion, and the similarity between nitric oxide and CO-dependent signaling, we studied the effects of CO on integrin signaling and cell adhesion. Results: We used a cell permeable CO releasing molecule (CORM-2) to elevate intracellular CO, and a fluorescent Very Late Antigen-4 (VLA-4, α4β1-integrin)-specific ligand to evaluate the integrin state in real-time on live cells. We show that the binding of the ligand can be rapidly down-modulated in resting cells and after inside-out activation through several Gαi-coupled receptors. Moreover, cell treatment with hemin, a natural source of CO, resulted in comparable VLA-4 ligand dissociation. Inhibition of VLA-4 ligand binding by CO had a dramatic effect on cell-cell interaction in a VLA-4/VCAM-1-dependent cell adhesion system. Conclusions: We conclude that the CO signaling pathway can rapidly down-modulate binding of the VLA-4 -specific ligand. -

List of Approved Ndas for Biological Products That Were Deemed to Be Blas on March 23, 2020
List of Approved NDAs for Biological Products That Were Deemed to be BLAs on March 23, 2020 On March 23, 2020, an approved application for a biological product under section 505 of the Federal Food, Drug, and Cosmetic Act (FD&C Act) was deemed to be a license for the biological product under section 351 of the Public Health Service Act (PHS Act) (see section 7002(e)(4)(A) of the Biologics Price Competition and Innovation Act of 2009). To enhance transparency and facilitate planning for the March 23, 2020, transition date, FDA compiled a preliminary list of approved applications for biological products under the FD&C Act that were listed in FDA’s Approved Drug Products with Therapeutic Equivalence Evaluations (the Orange Book) and that would be affected by this transition provision. FDA posted this list on the FDA website in December 2018, and periodically updated this list before the March 23, 2020, transition date. The September 2019 update to this preliminary list added certain administratively closed applications related to approved applications for biological products that were on the December 2018 version of this list. The January 2020 update to the preliminary list reflected a change to the definition of “biological product” made by the Further Consolidated Appropriations Act, 2020, which was enacted on December 20, 2019. Section 605 of this Act further amended the definition of a “biological product” in section 351(i) of the PHS Act to remove the parenthetical “(except any chemically synthesized polypeptide)” from the statutory category of “protein.” FDA has provided below a list of each approved application for a biological product under the FD&C Act that was deemed to be a license (i.e., an approved biologics license application (BLA)) for the biological product on March 23, 2020. -

The Rise of Orphan Drugs
The Rise of Orphan Drugs While drugs are being introduced at higher price points – orphan drugs are being introduced at price points that are many times that of other types of drugs. From 1998 to 2017, the average annual cost for orphan drugs increased 26-fold, while the cost for specialty and traditional drugs doubled. 4x They are being approved – and They are also being prescribed in increasing As a result, orphan drugs are entering the market – at higher numbers – often, for conditions that aren’t one of the biggest factors rates than ever before. Among orphan conditions and can be treated with driving out of control drug newly launched drugs, the share other therapies. In 2017, seven of the top prices, which puts coverage of orphan drugs increased more 10 best-selling drugs were orphan drugs and care out of reach for than 4-fold, from 10% to 44%, that were widely prescribed for non-orphan millions of hardworking over the same 20-year period. indications and off-label uses. American families. September 2019 /ahip @ahipcoverage AHIP | www.ahip.org Introduction Despite many efforts to contain health care costs, prescription Orphan Drug Act drug expenditures continue to grow. According to the Centers for Medicare and Medicaid Services (CMS) estimates, the total national The growth in orphan drug development prescription drug spending has reached $333.4 billion in 2017.1 In followed the passage of the Orphan Drug Act 3 the 5 years between 2013 and 2017, the national drug spending (ODA) in 1983. The ODA and its subsequent increased 25.7%. -

Medical Policy Statement
MEDICAL POLICY STATEMENT Effective Next Annual Last Review / Date Review Date Revision Date 06/15/2011 06/15/2012 06/15/2011 Author Shelley Jones RN, CCM, Wendy Null RPh CSMG Medical Policy Statements are derived from literature based and supported clinical guidelines, nationally recognized utilization and technology assessment guidelines, other medical management industry standards, and published MCO clinical policy guidelines. Medically necessary services are those health care services or supplies which are proper and necessary for the diagnosis or treatment of disease, illness, or injury and without which the patient can be expected to suffer prolonged, increased or new morbidity, impairment of function, dysfunction of a body organ or part or significant pain and discomfort. These services meet the standards of good medical practice in the local area, are the lowest cost alternative and are not provided mainly for the convenience of the member or provider. A. SUBJECT Alglucerase (Ceredase) Infusion B. BACKGROUND Alglucerase (Ceredase) is a modified form of the enzyme, ß-glucocerebrosidase (ß-D- glucosyl-N-acylsphingosine glucohydrolase). Alglucerase (Ceredase) catalyzes the hydrolysis of the glycolipid, glucocerebroside, to glucose and ceramide as part of the normal degradation pathway for membrane lipids. Glucocerebroside is primarily derived from hematologic cell turnover. Gaucher disease is characterized by a functional deficiency in ß-glucocerebrosidase enzymatic activity and the resultant accumulation of lipid glucocerebroside in tissue macrophages, which become engorged and are termed Gaucher cells. The patient selection criteria outlined was derived from the FDA-approved prescribing information for alglucerase (Ceredase), the studies that were presented to the FDA in support of the pre-market approval application, and studies in the peer-reviewed published medical literature. -

Emerging Concepts on the Anti-Inflammatory Actions of Carbon Monoxide-Releasing Molecules (CO-Rms)
Emerging concepts on the anti-inflammatory actions of carbon monoxide-releasing molecules (CO-RMs). Roberto Motterlini, Benjamin Haas, Roberta Foresti To cite this version: Roberto Motterlini, Benjamin Haas, Roberta Foresti. Emerging concepts on the anti-inflammatory actions of carbon monoxide-releasing molecules (CO-RMs).. Medical Gas Research, BioMed Central, 2012, 2 (1), pp.28. 10.1186/2045-9912-2-28. inserm-00769904 HAL Id: inserm-00769904 https://www.hal.inserm.fr/inserm-00769904 Submitted on 3 Jan 2013 HAL is a multi-disciplinary open access L’archive ouverte pluridisciplinaire HAL, est archive for the deposit and dissemination of sci- destinée au dépôt et à la diffusion de documents entific research documents, whether they are pub- scientifiques de niveau recherche, publiés ou non, lished or not. The documents may come from émanant des établissements d’enseignement et de teaching and research institutions in France or recherche français ou étrangers, des laboratoires abroad, or from public or private research centers. publics ou privés. Motterlini et al. Medical Gas Research 2012, 2:28 http://www.medicalgasresearch.com/content/2/1/28 MEDICAL GAS RESEARCH REVIEW Open Access Emerging concepts on the anti-inflammatory actions of carbon monoxide-releasing molecules (CO-RMs) Roberto Motterlini*, Benjamin Haas and Roberta Foresti* Abstract Carbon monoxide-releasing molecules (CO-RMs) are a class of organometallo compounds capable of delivering controlled quantities of CO gas to cells and tissues thus exerting a broad spectrum of pharmacological effects. CO-RMs containing transition metal carbonyls were initially implemented to mimic the function of heme oxygenase-1 (HMOX1), a stress inducible defensive protein that degrades heme to CO and biliverdin leading to anti-oxidant and anti-inflammatory actions. -

Cerezyme, INN- Imiglucerase
SCIENTIFIC DISCUSSION This module reflects the initial scientific discussion for the approval of Cerezyme. This scientific discussion has been updated until 01 August 2003. For information on changes after this date please refer to module 8B. 1. Introduction Gaucher disease, also called glucosylceramide lipidosis or ß-glucocerebrosidase (GCR) deficiency, is the most common of the sphingolipidoses or lipid storage diseases, a group of diseases that are inherited in an autosomal recessive manner. It is characterised by the accumulation of glucocerebroside in tissue macrophages. Gaucher disease presents in three subtypes: type 1, the non- neuronopathic form; type 2, the acute neuronopathic form; and 3, the chronic neuronopathic form. Of these, type 1, non-neuronopathic form, is the most frequent and type 2, acute neuronopathic, is the least frequent. It has been estimated that type 1 Gaucher disease affects more than 20,000 patients world-wide. The clinical features of Gaucher disease include anaemia and thrombocytopenia due to splenic sequestration and bone marrow replacement by accumulating Gaucher cells. Splenomegaly and hepatomegaly are other frequent signs. Skeletal disease eventually leading to pain, stress fractures and osteonecrosis are common symptoms in type 1 and 3 Gaucher disease. The neuronopathic forms also present neurological abnormalities such as seizures, dementia, spasticity, ataxia and loss of intellectual functions. Enzyme replacement therapy (ERT) of Gaucher disease has been made feasible by the introduction of mannose-terminated ß-glucocerebrosidase. Mannose is a sugar, which is abundant on the surfaces of micro-organisms. It may be bound by the mannose receptor of macrophages. The mannose- termination of ß-glucocerebrosidase leads to a selective uptake of the enzyme by macrophages that are present in liver, spleen and skeleton. -

From99mtc@Citrateand9smtc-Pertechnetateion Netate in Saline Solution and Subsequently Treated with a Sephadex G25 Column
jnin/CONCISE COMMUNICATION BINDING OF 9OmTcION TO HEMOGLOBIN MrinaI Kanti Dewanjee New England Medical Center, Tufts University School of Medicine, Boston, Massachusetts The mechanism and preferential site of bind removed, and the red cells were washed free of ing of 99―'Tcion to hemoglobin had been deter plasma with isotonic saline solution. The cells were mined by the separation of 9@Tc-hemoglobin then incubated with a small volume of oomTc@pertech@ from99mTc@citrateand9smTc-pertechnetateion netate in saline solution and subsequently treated with a Sephadex G25 column. This purified with the content of a kit containing mainly stannous fraction was analyzed by the HC1/acetone mix citrate and glucose. The method of labeling (6) is ture to determine the OsmTc activity distribution described below. with heme and globin. Most of the ssmTc activity Twenty milligrams of SnCl2 were dissolved in 20 is associated with globin fraction. The preferred ml of ACD solution (Abbott). The solution was fit chain for O9mTc ion binding was determined by tered with 0.22-micron Millipore filter paper. A 1-mi the splitting of otmTc.hemoglobin with para aliquot transferred to a serum vial was freeze-dried chloromercuribenzoate solution followed by sep and preserved under nitrogen atmosphere to prevent aration with a diethylaminoethyl cellulose col hydrolysis and oxidation of Sn(II) citrate. The kit umn equilibrated with phosphate buffer. The was reconstituted with I ml of isotonic saline solu @ tsmTc ion, like Cr' ion, tends to bind preferen tion, and the content was transferred to a washed red tially with the beta chain of hemoglobin. -

September 2017 ~ Resource #330909
−This Clinical Resource gives subscribers additional insight related to the Recommendations published in− September 2017 ~ Resource #330909 Medications Stored in the Refrigerator (Information below comes from current U.S. and Canadian product labeling and is current as of date of publication) Proper medication storage is important to ensure medication shelf life until the manufacturer expiration date and to reduce waste. Many meds are recommended to be stored at controlled-room temperature. However, several meds require storage in the refrigerator or freezer to ensure stability. See our toolbox, Medication Storage: Maintaining the Cold Chain, for helpful storage tips and other resources. Though most meds requiring storage at temperatures colder than room temperature should be stored in the refrigerator, expect to see a few meds require storage in the freezer. Some examples of medications requiring frozen storage conditions include: anthrax immune globulin (Anthrasil [U.S. only]), carmustine wafer (Gliadel [U.S. only]), cholera (live) vaccine (Vaxchora), dinoprostone vaginal insert (Cervidil), dinoprostone vaginal suppository (Prostin E2 [U.S.]), varicella vaccine (Varivax [U.S.]; Varivax III [Canada] can be stored in the refrigerator or freezer), zoster vaccine (Zostavax [U.S.]; Zostavax II [Canada] can be stored in the refrigerator or freezer). Use the list below to help identify medications requiring refrigerator storage and become familiar with acceptable temperature excursions from recommended storage conditions. Abbreviations: RT = room temperature Abaloparatide (Tymlos [U.S.]) Aflibercept (Eylea) Amphotericin B (Abelcet, Fungizone) • Once open, may store at RT (68°F to 77°F • May store at RT (77°F [25°C]) for up to Anakinra (Kineret) [20°C to 25°C]) for up to 30 days. -

FDA Approval Summary
Published OnlineFirst August 3, 2017; DOI: 10.1158/1078-0432.CCR-17-0898 CCR Drug Updates Clinical Cancer Research FDA Approval Summary: Trabectedin for Unresectable or Metastatic Liposarcoma or Leiomyosarcoma Following an Anthracycline- Containing Regimen Amy Barone, Dow-Chung Chi, Marc R. Theoret, Huanyu Chen, Kun He, Dubravka Kufrin, Whitney S. Helms, Sriram Subramaniam, Hong Zhao, Anuja Patel, Kirsten B. Goldberg, Patricia Keegan, and Richard Pazdur Abstract On October 23, 2015, the FDA approved trabectedin, a new log-rank test, P < 0.001). The most common adverse reactions molecular entity for the treatment of patients with unresectable or (20%) were nausea, fatigue, vomiting, constipation, decreased metastatic liposarcoma or leiomyosarcoma who received a prior appetite, diarrhea, peripheral edema, dyspnea, and headache. anthracycline-containing regimen. Approval was based on results Serious adverse reactions included anaphylaxis, neutropenic sep- of a single, randomized, active-controlled, 518-patient, multicen- sis, rhabdomyolysis, hepatotoxicity, cardiomyopathy, and extrav- ter study comparing the safety and efficacy of trabectedin 1.5 mg/ asation resulting in tissue necrosis. A postmarketing trial was m2 as a 24-hour continuous intravenous (i.v.) infusion once every required to evaluate the serious risk of cardiomyopathy. This 3 weeks with dacarbazine 1,000 mg/m2 i.v. once every 3 weeks. approval provides another treatment option in a setting where Treatment with trabectedin resulted in a statistically significant no drug has been shown to improve overall survival. A key improvement in progression-free survival (PFS), with a PFS of 4.2 regulatory consideration during review of this application was months and 1.5 months for trabectedin and dacarbazine, respec- the use of PFS as an endpoint to support regular approval of tively (HR, 0.55; 95% confidence interval, 0.44–0.70; unstratified trabectedin. -

Binding of Immunoglobulin G to Protoporphyrin IX and Its Derivatives: Evidence the Fab Domain Recognizes the Protoporphyrin Ring
antibodies Article Binding of Immunoglobulin G to Protoporphyrin IX and Its Derivatives: Evidence the Fab Domain Recognizes the Protoporphyrin Ring Koichi Orino Laboratory of Veterinary Biochemistry, School of Veterinary Medicine, Kitasato University, Aomori 034-8628, Japan; [email protected]; Tel.: +81-176-23-3471; Fax: +81-176-23-8703 Received: 15 November 2018; Accepted: 27 December 2018; Published: 4 January 2019 Abstract: Immunoglobulin G (IgG) is known to bind zinc via the Fc domain. In this study, biotinylated protoporphyrin IX (PPIX) was incubated with human IgG and then zinc-immobilized Sepharose beads (Zn-beads) were added to the mixture. After washing the beads, the binding of biotinylated PPIX with IgG trapped on Zn-beads was detected using alkaline phosphatase (ALP)-labeled avidin. Human IgG and its Fab domain coated on microtiter plate wells recognized biotin-labeled PPIX and its derivatives, Fe-PPIX and Zn-PPIX, whereas the Fc domain showed some extent of reaction only with Zn-PPIX. When rabbit anti-bovine transferrin (Tf) antibodies were incubated with biotinylated PPIX, the binding of anti-Tf antibodies with apo-Tf was indirectly detected using ALP-labeled avidin, suggesting that even if the antibody is modified with PPIX, the antibody-antigen reaction occurs. These results suggest that the IgG Fab domain recognizes PPIX and its derivatives, probably via the recognition of the PPIX ring. It is unlikely that binding between the Fab domain and PPIX affects the Fc domain-zinc interaction or antigen-antibody reaction. Keywords: antibody; Fab domain; Fc domain; protoporphyrin; zinc 1. Introduction In 1890, von Behring and Kitasato reported the presence of an agent in the blood that functioned as an anti-toxin, neutralizing diphtheria toxin, and this agent was eventually identified as the antibodies that control infection in body tissues [1,2]. -
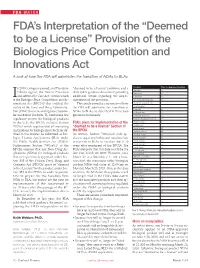
FDA's Interpretation of the “Deemed to Be a License”
FDA WATCH FDA’s Interpretation of the “Deemed to be a License” Provision of the Biologics Price Competition and Innovations Act A look at how the FDA will administer the transition of NDAs to BLAs n 2010, Congress passed, and President “deemed to be a license” provision and a Product Time to Approval (months) Aprotinin --- 4 Obama signed, the Patient Protection draft Q&A guidance document providing Beractant --- 1 Iand Affordable Care Act, within which additional details regarding the imple- Calfactant 35 is the Biologics Price Competition and In- mentation of the provision. Choriogonadotropin alfa 10 novations Act (BPCIA)2 that codified the This article provides a summary of how Chorionic gonadotropin* --- ability of the Food and Drug Administra- the FDA will administer the transition of Chymopapain --- Desirudin 33 tion (FDA) to review and approve biosimi- NDAs to BLAs, as described in these two Follitropin alfa 22 lar medicinal products. To harmonize the guidance documents. Follitropin alfa/beta 50 regulatory system for biological products Follicle stimulating hormone --- in the U.S., the BPCIA included Section FDA’s plans for Implementation of the Hyalurionidase 9 7002(e) which requires that all marketing “deemed to be a license” Section of Imiglucerase --- Insulin aspart 21 applications for biological products (as de- the BPCIA Insulin degludec 48 fined in the statute) be submitted as Bio- As written, Section 7002(e)(4) only ap- Insulin detemir 30 logics License Applications (BLA) under plies to approved NDAs and requires their Insulin glargine 12 the Public Health Services Act (PHSA). conversion to BLAs on the date that is 10 Insulin glulisine 10 Furthermore, Section 7002(e)(4) of the years after enactment of the BPCIA.