Sanitation, Ek Prem Katha: the Mpi Act of Sanitation on Education in Indian Government Schools Romanshi Gupta
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Ananda Katha
ANANDA KATHA BY NAGINA PRASAD CONTENTS Introduction 1 Chapter One October 1953: My friend Chandranathji and my vision of Baba. Baba sends His blessings and accepts me as a disciple. My initiation in November 1953 2 Chapter Two I am persecuted by my boss. Baba explains the real meaning of ahim’sa and the importance of iis’t’a mantra. 9 Chapter Three Jamalpur and the tiger’s grave. 11 Chapter Four Baba explains the meaning of varn’aghdana and warns against mean mindedness. The downfall of my persecutor. 15 Chapter Five February 1954: I get a sympathetic boss and am transferred to Begusarai. Manan Prasad miraculously loses weight. 19 Chapter Six Rainy Season 1954: My boss Asthanaji takes initiation and Baba appears before him. 22 Chapter Seven September 1954: Baba gives me the boon of only getting demotion when I myself desire it. My daughter dies and is miraculously resurrected and my wife takes initiation. 26 Chapter Eight The sufi saint Dattaji and his prophecy about Baba 30 Chapter Nine Winter 1954: Baba solves my difficulties in meditation and explains how His assistance is given from a distance. Shyam Charan Lahiri becomes ‘Vajra Bhairav’ at the tiger’s grave. Baba’s disciples of His previous lives. The ‘white lady’. The power and use of iis’t’a and guru mantras. Bindeshwariji’s daughter is initiated and her life is extended. My methods of pracar. 33 Chapter Ten November 1954: Demonstrations. Sunday 7th: Samadhis Sunday 14th Savikalpa and Nirvikalpa samadhi. Sunday 21st: Demonstration of death. Sunday 28th: Nirvikalpa samadhi. 42 Chapter Eleven Deep Narayanji and Vishvanathji are initiated and I try to feed Harisadhanji. -

September 2018 | 12 Pages | for Free Circulation Only |
Conversations Today Your journal about the world of NGOs and Social Enterprises RNI No.TNENG/2013/52428 | Volume 6 | Issue 9 | September 2018 | 12 Pages | For Free Circulation Only | www.msdstrust.org PUBLISHED BY: P.N.SUBRAMANIAN on behalf of Manava Seva Dharma Samvardhani, COVER STORY 391/1, Venkatachalapathi Nagar, Alapakkam, Chennai - 600 116 and printed by him at FOR THE LOVE OF WORDS Express Press, Express Gardens, No.29, About Katha, an NGO based in New Delhi, that Second Main Road, Ambattur Industrial Estate, brings children living in poverty into reading and Chennai - 600 058. Phone : 044-42805365 quality education Editor : Marie Banu 6 Alumni Talk Profile Chit Chat Promising a good beginning Freedom In-Step With Progress “I wake up every day feeling alive to my responsibilities.” Satyadev’s efforts to revive About Freedom For You interest in vedic mathematics Foundation, an organisation An exclusive interview with 3 and Abacus in pre-school 9 based in Navi Mumbai 12 Mr M. Mahadeven education Focus 2 Conversations Today • September 2018 Buy your fancy stuff FROM THE from an Indian slum EDITOR One woman is helping to transform Asia’s biggest slum into a global online market place. Dear Reader, “If you can read this, thank a teacher.” – Harry Truman All those who have been a part of any learning or training process or have been through the education system are aware of the significance of teachers. Teachers are like lamps that spread knowledge, awareness, and help channel the innate intelligence of students into something truly fulfilling and enriching. Teachers not only play a crucial role in imparting knowledge, but also help to inculcate compassion, empathy, and shape the perceptions of learners. -
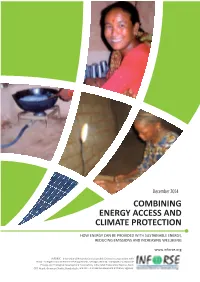
Combining Energy Access and Climate Protection
December 2014 COMBINING ENERGY ACCESS AND CLIMATE PROTECTION HOW ENERGY CAN BE PROVIDED WITH SUSTAINABLE ENERGY, REDUCING EMISSIONS AND INCREASING WELLBEING www.inforse.org ENDA - Energie-Environnement-Développement, Senegal; INSEDA - Integrated Sustainable CRT-Nepal; Grameen Shakti, Bangladesh; Combining Energy Access and Climate Protection: How Energy Can be Provided Sustainably, Reducing Emissions and Increasing Well-being Table of Contents Energy Access and Climate Protection – Overview and Summary ... page 3 Mali: Solar Lantern for Rural Household Lighting and Cell Phone Charging by Mali Folkecenter ... page 7 Mali: Jatropha Oil Production for Local Energy Use by Mali Folkecenter … page 11 Togo: Solar Lamp for a Households by ATODES/ENDA … page 15 Senegal: Baking Ovens: Improved Hybrid Ovens Using Gas/Woodfuel by ENDA … page 21 Senegal: Removal of the Subsidy on LPG by ENDA … page 24 India: Carbon Credit for Household Biogas Plants, by INSEDA … page 28 India: Bamboo Used at Biogas, Solar within Eco-Village Developments by INSEDA and WAFD … page 35 India: Solar Dryers for Income Generation by. AIWC … page 44 Sri Lanka: 'Anagi' Improved Cookstoves' Commercialisation by IDEA … page 52 Nepal: Improved Water Mills by CRT Nepal ... page 61 Bangladesh: Solar Home Systems with Micro Credits by Grameen Shakti … page 69 Contacts … page 74 Published by International Network for Sustainable Energy, INFORSE, 2014. 2 Introduction This publication highlights sustainable energy solutions that improve energy access and livelihood even as they reduce greenhouse-gas emissions. It was produced by INFORSE, the International Network for Sustainable Energy, in cooperation with ENDA/INFORSE-West Africa, INSEDA/INFORSE-South Asia, as well as other INFORSE members as Mali Folkecenter, CRT Nepal, and Grameen Shakti. -

Accountability Report
Accountability Report OıStatus of Commitments and Announcements Six Months on from Global Citizen Festival India on November 19, 2016 May 2017: Version 1.0 All Rights Reserved Global Citizen India 2 Introduction to the Global Citizen India Accountability Report Six months ago, on November 19, 2016, Mumbai was home to Driven by the shared ideals of actualizing the potential of young one of India’s largest ever entertainment events, hosted by people in India, and of channeling their collective voices as a Global Citizen Festival India, a partnership between Global catalyst for social change, the Global Education and Leadership Citizen and The Global Education & Leadership Foundation Foundation (tGELF) partnered with Global Citizen in 2016 to embark (tGELF). As an 80,000+ crowd gathered to celebrate the Global on the fifteen-year resolution of the Sustainable Development Goals Citizen Festival India with Coldplay, Jay Z, Amitabh Bachchan, (SDGs) together. Global Citizen India sought to address three A. R. Rahman, Vidya Balan, Demi Lovato, and two dozen specific SDGs in our 2016 campaign: Bollywood stars taking the stage, it was clear that it would be a night to remember. • SDG4: Quality Education – With the world’s largest population of youth, education must be one of India's top priorities. As UN India notes, "a quality education is the foundation of sustainable And, indeed, it was a night to remember, but not merely for its development, and therefore of the Sustainable Development scale and star power. Global Citizen India quickly became a Goals. As a policy intervention, education is a force multiplier movement uniting policymakers, corporate leaders, pop culture which enables self-reliance, boosts economic growth by icons, faith leaders and citizens for an ambitious goal: ending enhancing skills, and improves people’s lives by opening up extreme poverty by 2030. -

For Elimination of Lymphatic Filariasis in South-East Asia Region
Regional Programme Review Group (RPRG) For Elimination of Lymphatic Filariasis in South-East Asia Region Report of the Seventh Meeting Jakarta, Indonesia, 19–20 April, 2010 Regional Office for South-East Asia SEA-CD-211 Distribution: Limited Regional Programme Review Group (RPRG) For Elimination of Lymphatic Filariasis in South-East Asia Region Report of the Seventh Meeting Jakarta, Indonesia, 19–20 April, 2010 Regional Office for South-East Asia © World Health Organization 2010 This document is not issued to the general public, and all rights are reserved by the World Health Organization (WHO). The document may not be reviewed, abstracted, quoted, reproduced or translated, in part or in whole, without the prior written permission of WHO. No part of this document may be stored in a retrieval system or transmitted in any form or by any means – electronic, mechanical or other – without the prior written permission of WHO. The views expressed in documents by named authors are solely the responsibility of those authors. Printed in India Contents Page 1. Opening session ............................................................................................. 1 2. Status of lymphatic filariasis elimination .......................................................... 2 3. Progress made by Member States ................................................................... 4 3.1 Bangladesh............................................................................................. 4 3.2 India ..................................................................................................... -

Registered Charity Religious Organisation--Yes Bank
List of Charitable Organization, Trusts & Temples Charity Name Busines Filing Status Radiology Education Foundation AC Conference Registered Charity Bharatiya Vidya Bhavan Registered Charity neem foundation Registered Charity The Nalanda Foundation Registered Charity KATHA Registered Charity Needy Illiterate Children Education Registered Charity sri malayalaswamy seva samastha Registered Charity Indian Society of Agribusiness Professionals Registered Charity World Islamic Network Registered Charity Netizen Registered Charity SRI KOLLUR SEVA CHARITABLE SOCIETY Registered Charity Rotary Club Of Bombay Charities Trust No. 3 Registered Charity Dream Foundation Registered Charity swami nithyananda ashram public trust Registered Charity Global NRI Foundation Registered Charity The Biblio Charitable Trust Registered Charity SOMAIYA VIDYAVIHAR Registered Charity The Medplan Conservatory Society Registered Charity SSSMM Trust Registered Charity K.C. Mahindra Education Trust Registered Charity Vuyiroli Welfare Society Registered Charity Manashakti REST New Way Registered Charity Centre For Education and Documentation Registered Charity S.M. Nanavati Public charitable Trust Registered Charity Mar Gregorios Rehabilitation Centre for the Blind Registered Charity AICOG2005 Registered Charity Prashanti Medical Services and Research Foundation Registered Charity M.S. Chellamuthu Trust and Research Foundation Registered Charity INTEGRATED WOMEN DEVELOPMENT INSTITUTE (IWDI) Registered Charity Shree Vishwa Kapol Samaj Registered Charity GHRIACT , Nagpur -

(REACH India) for the Period of October 1, 2005 to September 31
American Institutes for Research Academy for Educational Development Aga Khan Foundation CARE Reaching and Educating At Risk Children (REACH India) Discovery Channel Global Education For the period of October 1, 2005 to September 31, 2006 Fund Education Development Center Howard University International Reading Association The Joseph P. Kennedy, Jr. Foundation Juárez and Associates, Inc. Submitted by: Michigan State University American Institutes for Research With: Sesame Workshop Juarez and Associates World Education Save the Children Federation, USA University of Pittsburgh U.S. Agency for International Development Cooperative Agreement No. GDG-A-00-03-00006-00 World Education American Institutes for Research 1000 Thomas Jefferson St. NW Washington, DC 20007 www.equip123.net 3 Table of Contents I. Executive Summary........................................................................................3 II. Introduction....................................................................................................6 III. Achievements.................................................................................................7 IV. Project Update – Regions...............................................................................8 A Delhi..................................................................................................8 a. Direct Service Delivery Grantees 1. AADI 2. CEMD 3. DISHA 4. KATHA 5. SARD b. Capacity Building Grantees 6. Deepalaya 7. Prayas B Jharkhand..........................................................................................12 -
View Annual Report
Experiential Leadership Enabling Personalized Customer Journeys Through Technology Annual Report 2017-18 HIGHLIGHTS Net Profit 17,487 crore An increase of 20.2% compared to the previous year. Balance Sheet Size 1,063,934 crore An increase of 23.2% compared to the previous year. Total Deposits 788,771 crore An increase of 22.5% compared to the previous year. Total Advances 658,333 crore An increase of 18.7% compared to the previous year. Capital Adequacy Ratio 14.8% Tier I Capital Ratio 13.2% Gross Non-performing Assets 1.30% of Gross Advances Network Banking outlets: 4,787 ATMs: 12,635 Cities/Towns: 2,691 TABLE OF CONTENTS Board and Management 2 AGM and Record Date Details 5 Evolving into an Experience Business, Digitally 6 Parivartan – A Step towards Progress 10 Working with the Government 12 Graphical Highlights 14 Financial Highlights 18 Directors’ Report 20 Independent Auditors’ Report 77 Financial Statements 80 Basel III- Pillar 3 Disclosures 155 Independent Auditors’ Report for 156 Consolidated Financial Statements Consolidated Financial Statements 160 Secretarial Auditor’s Certificate 209 on Corporate Governance Corporate Governance 210 Shareholder Information 234 BOARD AND MANAGEMENT BOARD OF DIRECTORS Shyamala Gopinath Bobby Parikh Partho Datta Malay Patel Chairperson Umesh Chandra Srikanth Nadhamuni Keki Mistry Sarangi Aditya Puri Paresh Sukthankar Kaizad Bharucha Managing Director Deputy Managing Director Executive Director KEY MANAGERIAL PERSONS Aditya Puri Paresh Sukthankar Kaizad Bharucha Managing Director Deputy Managing Director -

National Volunteering Week 2021
NATIONAL VOLUNTEERING 18–24 JANUARY WEEK 2021 REPORT Contents Overview Thoughts from Leaders Journey thus far Highlights of the week Corporate participation NVW 2021 statistics NVW 2021 footprint Social media dashboard Social media highlights Partners Way ahead Calendar of activities NATIONAL VOLUNTEERING WEEK 2021 4 NATIONAL VOLUNTEERING WEEK 2021 Overview Confederation of Indian Industry (CII) a collective of businesses through its in- stitution India@75 Foundation has been working on a nation-building agenda for over a decade. In 2008, CII evolved a vision for the nation through a pan India consultative process called ‘India@75 – The People’s Agenda’. It embarked on an industry-led movement to achieve the vision objective of an inclusively developed India by the year 2022 by focusing on seven growth areas. It entailed Industry collaborating both internally and with different stakeholder groups to synergize their efforts and align the same with national priorities to accentuate the process set by the Government of India. At the core of India@75’s vision is collaboration and people’s participation. Volun- teering is an enabler for both. National Volunteering Week (NVW) was instituted in 2014, held from 18 to 24 January every year and since then it has grown from strength to strength. It is an effort to showcase volunteering as a simple and most powerful form of multi-stakeholder collaboration that can be pivotal in addressing some of the most critical gaps in the country’s development agenda. Every year, non-profits, academic institutions, corporates, other organization from across the country come together to organize activities specifically for this week. -

People Like Us Pavan Varma
PEOPLE LIKE US PAVAN VARMA Preface This book, which brings together the column People Like Us, which I wrote for several months for The Hindustan Times, will give you the examples of people and institutions who have somehow broken through the haze of cynicism, and have contributed in personally satisfying ways to society over and above the normal preoccupations of a metropolis. The examples are largely from in and around New Delhi, but I have not the slightest doubt that they are a representative sample of what a few — alas just a few —are doing elsewhere in India too. These individuals and organizations need your help and involvement. In helping them you will only, in the long run, be helping yourself. The purpose of this book is to try and revive the project of social sensitivity —pivotal for the survival of any civil society. It is a book that can change your life and with it the destiny of India too. I am grateful to Har-Anand Publications who so readily collaborated in the publication of the book. I owe a special note of thanks to Narendra Kumar with whom I first discussed the project, and to his son, Ashish Gosain, who so efficiently brought it to fruition. My gratitude is also due to Rohit Babbar, my colleague, who helped in the making of the columns. I need hardly add that this book would not have been possible but for the fullest cooperation of those who are featured in them. I remain indebted to them. PAVAN K. VARMA Contents Help Age India: Because We too Will be Old Sai Kripa at NOIDA — Anjina Rajagopal Child Relief and You — Praveen Sharma & Radha Roy Sarkar A Home for Our Children — Meera Mahadevan A People’s Movement against Pollution — Satya Sheel & Saurabh Khosla Why Can’t Delhi be Kottayam?- T. -

Mango-Souvenir Final
Directorate of Extension Souvenir Pusa Mango Day-2015 Wednesday, July 15, 2015 Venue Dr. B.P. Pal Auditorium, IARI, New Delhi ICAR-Indian Agricultural Research Institute New Delhi 110012 SouvenirSouvenir Directorate of Extension Pusa Mango Day-2015 Wednesday, July 15, 2015 Venue Dr. B.P. Pal Auditorium IARI, New Delhi ICAR-Indian Agricultural Research Institute New Delhi 110012 ©2015 ICAR-Indian Agricultural Research Institute, New Delhi Citation IARI. 2015. Souvenir of the Pusa Mango Day-2015 compiled and edited by Dr K. Usha, Dr S.K. Singh, Dr A.K. Dubey, Dr M.K. Verma, Dr Manish Srivastav and Dr R.M. Sharma, Division of Fruits and Horticultural Technology, ICAR-Indian Agricultural Research Institute, New Delhi 110012, held on July 15th, 2015, 46 p. + x Editors Dr K. Usha Dr S.K. Singh Dr A.K. Dubey Dr M.K. Verma Dr Manish Srivastav Dr R.M. Sharma Acknowledgement The financial assistance received from NABARD and Directorate of Extension, Krishi Vistar Sadan, Ministry of Agriculture Govt. of India. Declaration The views presented in this document are those of the author(s) and not necessarily that of the publishers Published by The Director ICAR-Indian Agricultural Research Institute New Delhi 110012 Printed at Venus Printers and Publishers, B-62/8, Naraina Industrial Area, Phase-II, New Delhi-110028 Ph. : 45576780, M. : 9810089097, E-mail: [email protected] Pusa Mango Day-2015 Division of Fruits & Horticultural Technology ICAR-Indian Agricultural Research Institute, New Delhi Date: July 15, 2015 Venue: Dr B.P. Pal Auditorium Committees Organizing Committee Dr Ravinder Kaur, Director, IARI Chairperson Dr K.V. -

Human Values and Professional Ethics
Human Values and Professional Ethics Editors : Dr. P.K. Varshney Syad Abdul Wahid Shah Deepak Kumar Sharma i Human Values and Professional Ethics Editors : Dr. P.K. Varshney Syad Abdul Wahid Shah Deepak Kumar Sharma ISBN : 978-81-943559-8-4 Printed by: Ocean Publication Near Hanuman Temple, Miston Ganj, Rampur (U.P.)-244901 #9045440373 Published by: Govt. Raza P.G. College Rampur (U.P.)-244901 (Etsblished 1949, Completed III Cycle of NAAC) Affiliated to M.J.P. Rohilkhand University, Bareilly (U.P.) Website : www.grpgcrampur.com Foreword “Education occupies a very important place in human life. Education is capable of making life meaningful and to give proper momentum to the development of society. In today's technological and materialistic era, our fundamental and moral values are being lost, and only material comforts remain part of the blind race for prosperity, with which we can be rich physically but we are becoming weak spiritually and mentally. Therefore, there is a need to know, understand and adopt these human values so that along with the material progress, we can flourish the human civilization and culture and inspire the whole world to contemplate the new direction. As a result of this endeavor, this book with 17 sub-topics and related issues is being presented in the hands of readers, academics, teachers, researchers and students with the aim to bring this important subject to the public and to embrace human values and morality in life. Dr. P.K. Varshney Syad Abdul Wahid Shah Deepak Kumar Sharma iv Index S.No. Topic/Author Pg.