Documentazione Scientifica
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

"National List of Vascular Plant Species That Occur in Wetlands: 1996 National Summary."
Intro 1996 National List of Vascular Plant Species That Occur in Wetlands The Fish and Wildlife Service has prepared a National List of Vascular Plant Species That Occur in Wetlands: 1996 National Summary (1996 National List). The 1996 National List is a draft revision of the National List of Plant Species That Occur in Wetlands: 1988 National Summary (Reed 1988) (1988 National List). The 1996 National List is provided to encourage additional public review and comments on the draft regional wetland indicator assignments. The 1996 National List reflects a significant amount of new information that has become available since 1988 on the wetland affinity of vascular plants. This new information has resulted from the extensive use of the 1988 National List in the field by individuals involved in wetland and other resource inventories, wetland identification and delineation, and wetland research. Interim Regional Interagency Review Panel (Regional Panel) changes in indicator status as well as additions and deletions to the 1988 National List were documented in Regional supplements. The National List was originally developed as an appendix to the Classification of Wetlands and Deepwater Habitats of the United States (Cowardin et al.1979) to aid in the consistent application of this classification system for wetlands in the field.. The 1996 National List also was developed to aid in determining the presence of hydrophytic vegetation in the Clean Water Act Section 404 wetland regulatory program and in the implementation of the swampbuster provisions of the Food Security Act. While not required by law or regulation, the Fish and Wildlife Service is making the 1996 National List available for review and comment. -

Hampton-Seabrook Estuary Habitat Restoration Compendium Alyson L
University of New Hampshire University of New Hampshire Scholars' Repository Institute for the Study of Earth, Oceans, and Space PREP Reports & Publications (EOS) 2009 Hampton-Seabrook Estuary Habitat Restoration Compendium Alyson L. Eberhardt University of New Hampshire - Main Campus, [email protected] David M. Burdick University of New Hampshire - Main Campus, [email protected] Follow this and additional works at: https://scholars.unh.edu/prep Part of the Marine Biology Commons Recommended Citation Eberhardt, Alyson L. and Burdick, David M., "Hampton-Seabrook Estuary Habitat Restoration Compendium" (2009). PREP Reports & Publications. 102. https://scholars.unh.edu/prep/102 This Report is brought to you for free and open access by the Institute for the Study of Earth, Oceans, and Space (EOS) at University of New Hampshire Scholars' Repository. It has been accepted for inclusion in PREP Reports & Publications by an authorized administrator of University of New Hampshire Scholars' Repository. For more information, please contact [email protected]. Hampton-Seabrook Estuary Habitat Restoration Compendium Alyson L. Eberhardt and David M. Burdick University of New Hampshire This project was funded by the NOAA Restoration Center in conjunction with the Coastal Zone Management Act by NOAA’s Office of Ocean and Coastal Resource Management in conjunction with the New Hampshire Coastal Program and US Environmental Protection Agency’s National Estuary Program through an agreement with the University of New Hampshire Hampton-Seabrook -

State of New York City's Plants 2018
STATE OF NEW YORK CITY’S PLANTS 2018 Daniel Atha & Brian Boom © 2018 The New York Botanical Garden All rights reserved ISBN 978-0-89327-955-4 Center for Conservation Strategy The New York Botanical Garden 2900 Southern Boulevard Bronx, NY 10458 All photos NYBG staff Citation: Atha, D. and B. Boom. 2018. State of New York City’s Plants 2018. Center for Conservation Strategy. The New York Botanical Garden, Bronx, NY. 132 pp. STATE OF NEW YORK CITY’S PLANTS 2018 4 EXECUTIVE SUMMARY 6 INTRODUCTION 10 DOCUMENTING THE CITY’S PLANTS 10 The Flora of New York City 11 Rare Species 14 Focus on Specific Area 16 Botanical Spectacle: Summer Snow 18 CITIZEN SCIENCE 20 THREATS TO THE CITY’S PLANTS 24 NEW YORK STATE PROHIBITED AND REGULATED INVASIVE SPECIES FOUND IN NEW YORK CITY 26 LOOKING AHEAD 27 CONTRIBUTORS AND ACKNOWLEGMENTS 30 LITERATURE CITED 31 APPENDIX Checklist of the Spontaneous Vascular Plants of New York City 32 Ferns and Fern Allies 35 Gymnosperms 36 Nymphaeales and Magnoliids 37 Monocots 67 Dicots 3 EXECUTIVE SUMMARY This report, State of New York City’s Plants 2018, is the first rankings of rare, threatened, endangered, and extinct species of what is envisioned by the Center for Conservation Strategy known from New York City, and based on this compilation of The New York Botanical Garden as annual updates thirteen percent of the City’s flora is imperiled or extinct in New summarizing the status of the spontaneous plant species of the York City. five boroughs of New York City. This year’s report deals with the City’s vascular plants (ferns and fern allies, gymnosperms, We have begun the process of assessing conservation status and flowering plants), but in the future it is planned to phase in at the local level for all species. -

Perennial Pepperweed Lepidium Latifolium L
perennial pepperweed Lepidium latifolium L. Synonyms: Cardaria latifolia (L.) Spach, Lepidium affine Ledebour, L. latifolium ssp. affine (Ledebour) Kitagawa, L. latifolium var. affine (Ledebour) C. A. Meyer, L. latifolium ssp. sibiricum Thellung, L. sibiricum Schweigger (1812), not Pallas (1776). Other common names: broadleaved pepperweed, broadleaved peppergrass, peppergrass mustard, perennial peppercress, tall whitetop, Virginia pepperweed Family: Brassicaceae Invasiveness Rank: 71 The invasiveness rank is calculated based on a species’ ecological impacts, biological attributes, distribution, and response to control measures. The ranks are scaled from 0 to 100, with 0 representing a plant that poses no threat to native ecosystems and 100 representing a plant that poses a major threat to native ecosystems. Description Perennial pepperweed grows from a widely spreading root system. Stems are numerous, erect, and 30 ½ to 91 cm tall. Basal leaves are entire to evenly toothed, up to 30 ½ cm long, and 5 to 7 ½ cm wide. Petioles are nearly equal to the blades in length. Stem leaves are reduced in size and lack petioles. Plants form dense clusters of flowers in pyramidal panicles. Flowers are white, very small, and approximately 1.5 mm long. Each fruit (silicle) contains 2 seeds (Douglas et al. 1998, Renz 2000, Whitson et al. 2000). Basal rosettes of Lepidium latifolium L. Photo by L. Mehrhoff. Ecological Impact Impact on community composition, structure, and interactions: Perennial pepperweed creates large, monospecific stands that displace native plants and animals (Corliss 1993, Renz 2000). Stands of perennial pepperweed increase the salt content of surrounding soil, favoring halophytes and eliminating other species. Infestations change plant species composition and diversity. -
Oriental Bittersweet Orientalcelastrus Bittersweet Orbiculatus Controlcontrol Guidelinesguidelines
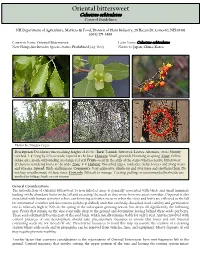
Oriental bittersweet OrientalCelastrus bittersweet orbiculatus ControlControl GuidelinesGuidelines NH Department of Agriculture, Markets & Food, Division of Plant Industry, 29 Hazen Dr, Concord, NH 03301 (603) 271-3488 Common Name: Oriental Bittersweet Latin Name: Celastrus orbiculatus New Hampshire Invasive Species Status: Prohibited (Agr 3800) Native to: Japan, China, Korea Photos by: Douglas Cygan Description: Deciduous vine reaching heights of 40-60'. Bark: Tannish, furrowed. Leaves: Alternate, ovate, bluntly toothed, 3-4'' long by 2/3’s as wide, tapered at the base. Flowers: Small, greenish, blooming in spring. Fruit: Yellow dehiscent capsule surrounding an orange-red aril. Fruits occur in the axils of the stems whereas native bittersweet (Celastrus scandens) fruits at the ends. Zone: 4-8. Habitat: Disturbed edges, roadsides, fields, forests and along rivers and streams. Spread: Birds and humans. Comments: Very aggressive, climbs up and over trees and smothers them. Do not buy wreaths made of these vines. Controls: Difficult to manage. Cutting, pulling, or recommended herbicide use applied to foliage, bark, or cut-stump. General Considerations The introduction of Oriental bittersweet to non infested areas is generally associated with birds and small mammals feeding on the abundant fruits in the fall and excreting the seeds as they move from one area to another. Dispersal is also associated with human activities where earth moving activities occur or when the vines and fruits are collected in the fall for ornamental wreathes and decorations (which is prohibited) and then carelessly discarded. Seed viability and germination rate is relatively high at 90% in the spring of the subsequent growing season, but drops off significantly the following year. -

Field Release of the Gall Mite, Aceria Drabae
United States Department of Field release of the gall mite, Agriculture Aceria drabae (Acari: Marketing and Regulatory Eriophyidae), for classical Programs biological control of hoary Animal and Plant Health Inspection cress (Lepidium draba L., Service Lepidium chalapense L., and Lepidium appelianum Al- Shehbaz) (Brassicaceae), in the contiguous United States. Environmental Assessment, January 2018 Field release of the gall mite, Aceria drabae (Acari: Eriophyidae), for classical biological control of hoary cress (Lepidium draba L., Lepidium chalapense L., and Lepidium appelianum Al-Shehbaz) (Brassicaceae), in the contiguous United States. Environmental Assessment, January 2018 Agency Contact: Colin D. Stewart, Assistant Director Pests, Pathogens, and Biocontrol Permits Plant Protection and Quarantine Animal and Plant Health Inspection Service U.S. Department of Agriculture 4700 River Rd., Unit 133 Riverdale, MD 20737 Non-Discrimination Policy The U.S. Department of Agriculture (USDA) prohibits discrimination against its customers, employees, and applicants for employment on the bases of race, color, national origin, age, disability, sex, gender identity, religion, reprisal, and where applicable, political beliefs, marital status, familial or parental status, sexual orientation, or all or part of an individual's income is derived from any public assistance program, or protected genetic information in employment or in any program or activity conducted or funded by the Department. (Not all prohibited bases will apply to all programs and/or employment activities.) To File an Employment Complaint If you wish to file an employment complaint, you must contact your agency's EEO Counselor (PDF) within 45 days of the date of the alleged discriminatory act, event, or in the case of a personnel action. -

National Wetlands Inventory Map Report for Quinault Indian Nation
National Wetlands Inventory Map Report for Quinault Indian Nation Project ID(s): R01Y19P01: Quinault Indian Nation, fiscal year 2019 Project area The project area (Figure 1) is restricted to the Quinault Indian Nation, bounded by Grays Harbor Co. Jefferson Co. and the Olympic National Park. Appendix A: USGS 7.5-minute Quadrangles: Queets, Salmon River West, Salmon River East, Matheny Ridge, Tunnel Island, O’Took Prairie, Thimble Mountain, Lake Quinault West, Lake Quinault East, Taholah, Shale Slough, Macafee Hill, Stevens Creek, Moclips, Carlisle. • < 0. Figure 1. QIN NWI+ 2019 project area (red outline). Source Imagery: Citation: For all quads listed above: See Appendix A Citation Information: Originator: USDA-FSA-APFO Aerial Photography Field Office Publication Date: 2017 Publication place: Salt Lake City, Utah Title: Digital Orthoimagery Series of Washington Geospatial_Data_Presentation_Form: raster digital data Other_Citation_Details: 1-meter and 1-foot, Natural Color and NIR-False Color Collateral Data: . USGS 1:24,000 topographic quadrangles . USGS – NHD – National Hydrography Dataset . USGS Topographic maps, 2013 . QIN LiDAR DEM (3 meter) and synthetic stream layer, 2015 . Previous National Wetlands Inventories for the project area . Soil Surveys, All Hydric Soils: Weyerhaeuser soil survey 1976, NRCS soil survey 2013 . QIN WET tables, field photos, and site descriptions, 2016 to 2019, Janice Martin, and Greg Eide Inventory Method: Wetland identification and interpretation was done “heads-up” using ArcMap versions 10.6.1. US Fish & Wildlife Service (USFWS) National Wetlands Inventory (NWI) mapping contractors in Portland, Oregon completed the original aerial photo interpretation and wetland mapping. Primary authors: Nicholas Jones of SWCA Environmental Consulting. 100% Quality Control (QC) during the NWI mapping was provided by Michael Holscher of SWCA Environmental Consulting. -

Fort Ord Natural Reserve Plant List
UCSC Fort Ord Natural Reserve Plants Below is the most recently updated plant list for UCSC Fort Ord Natural Reserve. * non-native taxon ? presence in question Listed Species Information: CNPS Listed - as designated by the California Rare Plant Ranks (formerly known as CNPS Lists). More information at http://www.cnps.org/cnps/rareplants/ranking.php Cal IPC Listed - an inventory that categorizes exotic and invasive plants as High, Moderate, or Limited, reflecting the level of each species' negative ecological impact in California. More information at http://www.cal-ipc.org More information about Federal and State threatened and endangered species listings can be found at https://www.fws.gov/endangered/ (US) and http://www.dfg.ca.gov/wildlife/nongame/ t_e_spp/ (CA). FAMILY NAME SCIENTIFIC NAME COMMON NAME LISTED Ferns AZOLLACEAE - Mosquito Fern American water fern, mosquito fern, Family Azolla filiculoides ? Mosquito fern, Pacific mosquitofern DENNSTAEDTIACEAE - Bracken Hairy brackenfern, Western bracken Family Pteridium aquilinum var. pubescens fern DRYOPTERIDACEAE - Shield or California wood fern, Coastal wood wood fern family Dryopteris arguta fern, Shield fern Common horsetail rush, Common horsetail, field horsetail, Field EQUISETACEAE - Horsetail Family Equisetum arvense horsetail Equisetum telmateia ssp. braunii Giant horse tail, Giant horsetail Pentagramma triangularis ssp. PTERIDACEAE - Brake Family triangularis Gold back fern Gymnosperms CUPRESSACEAE - Cypress Family Hesperocyparis macrocarpa Monterey cypress CNPS - 1B.2, Cal IPC -

Spiranthes Diluvialis) and for Designated Weeds
2000 Survey of BLM-Managed Public Lands in Southwestern Wyoming for Ute Ladies Tresses (Spiranthes diluvialis) and for Designated Weeds Report Prepared for the BLM Rock Springs Field Office by George P. Jones, Wyoming Natural Diversity Database (University of Wyoming) in partial fulfillment of Cooperative Agreement K910A970018, Task Order TO-13 April 2001 TABLE OF CONTENTS ABSTRACT.........................................................................................................................i BACKGROUND................................................................................................................. 1 METHODS.......................................................................................................................... 1 RESULTS............................................................................................................................ 2 SPIRANTHES DILUVALIS .................................................................................. 2 WEEDS ................................................................................................................... 2 DISCUSSION ..................................................................................................................... 2 REFERENCES.................................................................................................................... 3 APPENDIX 1: DESCRIPTIONS OF STREAM SEGMENTS .........................................8 APPENDIX 2: ABUNDANCE OF THE DESIGNATED WEEDS IN EACH STREAM SEGMENT........................................................................................................................18 -

10 Years of Conservation Science on the Zumwalt Prairie
10 YEARS OF CONSERVATION SCIENCE ON THE ZUMWALT PRAIRIE What Have We Learned? Geographically isolated and comprised mostly of private lands, scant scientific information exists regarding the soils, vegetation, wildlife and ecology of the Zumwalt Prairie. Science is at the core of the Nature Conservancy’s conservation approach and soon after the Conservancy acquired the Zumwalt Prairie Preserve in 2000, the organization recognized the need to support scientific inquiry into the prairie’s ecology and how human actions such as livestock grazing, fire, and invasive species affect it. Beginning with a study of the prairie’s raptor populations in 2003, the Conservancy has collaborated with universities and agencies for over ten years in its quest to find answers to key conservation questions. Over 10 published papers, dozens of reports and presentations have resulted in these efforts, broadening our knowledge of the biodiversity and ecological processes of the Zumwalt and informing stewardship and other conservation actions. Conservancy staff also serve on technical advisory groups, review boards, and in other roles to promote scientific inquiry and communication of information to landowners and other stakeholders. Short summaries of findings resulting from Zumwalt Science efforts are summarized below. For more information contact Rob Taylor ([email protected]). Many of the reports, lists, and publications cited here can be found on the Conservation Gateway at: https://www.conservationgateway.org/ConservationByGeography/NorthAmerica/UnitedStates/oregon/grasslands/zumwalt BIODIVERSITY While no formal “bio blitz” has ever been undertaken on the Zumwalt Prairie, various inventory, monitoring and research projects have contributed to our understanding of the biodiversity that inhabits this extraordinary grassland ecosystem. -

Washington Flora Checklist a Checklist of the Vascular Plants of Washington State Hosted by the University of Washington Herbarium
Washington Flora Checklist A checklist of the Vascular Plants of Washington State Hosted by the University of Washington Herbarium The Washington Flora Checklist aims to be a complete list of the native and naturalized vascular plants of Washington State, with current classifications, nomenclature and synonymy. The checklist currently contains 3,929 terminal taxa (species, subspecies, and varieties). Taxa included in the checklist: * Native taxa whether extant, extirpated, or extinct. * Exotic taxa that are naturalized, escaped from cultivation, or persisting wild. * Waifs (e.g., ballast plants, escaped crop plants) and other scarcely collected exotics. * Interspecific hybrids that are frequent or self-maintaining. * Some unnamed taxa in the process of being described. Family classifications follow APG IV for angiosperms, PPG I (J. Syst. Evol. 54:563?603. 2016.) for pteridophytes, and Christenhusz et al. (Phytotaxa 19:55?70. 2011.) for gymnosperms, with a few exceptions. Nomenclature and synonymy at the rank of genus and below follows the 2nd Edition of the Flora of the Pacific Northwest except where superceded by new information. Accepted names are indicated with blue font; synonyms with black font. Native species and infraspecies are marked with boldface font. Please note: This is a working checklist, continuously updated. Use it at your discretion. Created from the Washington Flora Checklist Database on September 17th, 2018 at 9:47pm PST. Available online at http://biology.burke.washington.edu/waflora/checklist.php Comments and questions should be addressed to the checklist administrators: David Giblin ([email protected]) Peter Zika ([email protected]) Suggested citation: Weinmann, F., P.F. Zika, D.E. Giblin, B. -

Thomas Coulter's Californian Exsiccata
Aliso: A Journal of Systematic and Evolutionary Botany Volume 37 Issue 1 Issue 1–2 Article 2 2019 Plantae Coulterianae: Thomas Coulter’s Californian Exsiccata Gary D. Wallace California Botanic Garden, Claremont, CA Follow this and additional works at: https://scholarship.claremont.edu/aliso Part of the Botany Commons Recommended Citation Wallace, Gary D. (2020) "Plantae Coulterianae: Thomas Coulter’s Californian Exsiccata," Aliso: A Journal of Systematic and Evolutionary Botany: Vol. 37: Iss. 1, Article 2. Available at: https://scholarship.claremont.edu/aliso/vol37/iss1/2 Aliso, 37(1–2), pp. 1–73 ISSN: 0065-6275 (print), 2327-2929 (online) PLANTAE COULTERIANAE: THOMAS COULTER’S CALIFORNIAN EXSICCATA Gary D. Wallace California Botanic Garden [formerly Rancho Santa Ana Botanic Garden], 1500 North College Avenue, Claremont, California 91711 ([email protected]) abstract An account of the extent, diversity, and importance of the Californian collections of Thomas Coulter in the herbarium (TCD) of Trinity College, Dublin, Ireland, is presented here. It is based on examination of collections in TCD, several other collections available online, and referenced literature. Additional infor- mation on historical context, content of herbarium labels and annotations is included. Coulter’s collections in TCD are less well known than partial duplicate sets at other herbaria. He was the first botanist to cross the desert of southern California to the Colorado River. Coulter’s collections in TCD include not only 60 vascular plant specimens previously unidentified as type material but also among the first moss andmarine algae specimens known to be collected in California. A list of taxa named for Thomas Coulter is included.