The Nephrotic Syndrome in Early Infancy: a Report of Three Cases* by H
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Focal Segmental Glomerulosclerosis in Systemic Lupus Erythematosus
Relato de Caso Focal Segmental Glomerulosclerosis in Systemic Lupus Erythematosus: One or Two Glomerular Diseases? Glomerulosclerose Segmentar e Focal em Lúpus Eritematoso Sistêmico: Uma ou Duas Doenças? Rogério Barbosa de Deus1, Luis Antonio Moura1, Marcello Fabiano Franco2, Gianna Mastroianni Kirsztajn1 1 Nephrology Division and 2 Department of Pathology - Universidade Federal de São Paulo – EPM/UNIFESP- São Paulo. ABSTRACT Some patients with clinical and/or laboratory diagnosis of systemic lupus erythematosus (SLE) present with nephritis which from the morphological point of view does not fit in one of the 6 classes described in the WHO classification of lupus nephritis. On the other hand, nonlupus nephritis in patients with confirmed SLE is rarely reported. This condition may not be so uncommon as it seems. The associated glomerular lesions most frequently described are amyloidosis and focal segmental glomerulosclerosis (FSGS). We report on a 46 year-old, caucasian woman, who fulfilled the American College of Rheumatology criteria for SLE diagnosis: arthritis, positive anti-DNA, ANA, anti-Sm antibodies, and cutaneous maculae. During the follow-up, she presented arthralgias, alopecia, vasculitis, lower extremities edema and decreased serum levels of C3 and C4. Proteinuria was initially nephrotic, but reached negative levels. The serum creatinine varied from 0.7 to 3.0 mg/dl. The patient was submitted to the first renal biopsy at admission and to the second one, 3 years later, with diagnosis of minimal change disease and FSGS, respectively. No deposits were demonstrated by immunofluorescence. In the present case, we believe that the patient had SLE and developed an idiopathic disease of the minimal change disease-FSGS spectrum. -
What Is Lupus Nephritis
What is lupus nephritis (LN)? Lupus nephritis (LN) is inflammation of the kidney that occurs as a common symptom of systemic lupus erythematosus (SLE), also known as lupus. Proteins in the immune system called antibodies damage important structures in the kidney. ⅱ Why are the kidneys important? To understand how lupus nephritis damages the kidney, it is important to understand how the kidneys work. The kidneys’ main function is to filter out excess waste and water from the blood through the urine. Kidneys also balance the salts and minerals circulating in the blood, help control blood pressure and make red blood cells. So, when the kidneys are damaged or fail, they can’t do their job as well. As a result, the kidneys are not able to filter out waste and water into the urine causing it to stay in the blood. What are the signs and symptoms of LN? Signs to ask the doctor about include blood in the urine or foamy urine which can mean that there is excess protein. Other signs to notice are swelling of legs, ankles, hands or tissue around the eyes as well as weight gain that can be caused by fluid the body isn’t getting rid of. ⅲ Symptoms of lupus nephritis also include high blood pressure, joint/muscle pain, high levels of waste (creatinine) in the blood, or impaired/failing kidney. ⅳ How common is LN? Lupus nephritis is the most common complication of lupus. Five out of 10 adults with lupus will have lupus nephritis, while eight out of 10 children with lupus will have kidney damage, which usually stems from lupus nephritis. -

Risk of Renal Function Decline in Patients with Ketamine-Associated Uropathy
International Journal of Environmental Research and Public Health Article Risk of Renal Function Decline in Patients with Ketamine-Associated Uropathy Shih-Hsiang Ou 1,2,3, Ling-Ying Wu 4, Hsin-Yu Chen 1,2, Chien-Wei Huang 1,2, Chih-Yang Hsu 1,2, Chien-Liang Chen 1,2 , Kang-Ju Chou 1,2, Hua-Chang Fang 1,2 and Po-Tsang Lee 1,2,* 1 Division of Nephrology, Department of Internal Medicine, Kaohsiung Veterans General Hospital, Kaohsiung 813, Taiwan; [email protected] (S.-H.O.); [email protected] (H.-Y.C.); [email protected] (C.-W.H.); [email protected] (C.-Y.H.); [email protected] (C.-L.C.); [email protected] (K.-J.C.); [email protected] (H.-C.F.) 2 Faculty of Medicine, School of Medicine, National Yang-Ming University, Taipei 112, Taiwan 3 Graduate Institute of Clinical Medicine, College of Medicine, Kaohsiung Medical University, Kaohsiung 807, Taiwan 4 Department of Obstetrics and Gynecology, Kaohsiung Chang Gung Memorial Hospital, Kaohsiung 833, Taiwan; [email protected] * Correspondence: [email protected]; Tel.: +886-7342-2121 (ext. 8090) Received: 8 August 2020; Accepted: 29 September 2020; Published: 4 October 2020 Abstract: Ketamine-associated diseases have been increasing with the rise in ketamine abuse. Ketamine-associated uropathy is one of the most common complications. We investigated the effects of ketamine-associated uropathy on renal health and determined predictors of renal function decline in chronic ketamine abusers. This retrospective cohort study analyzed 51 patients (22 with ketamine- associated hydronephrosis and 29 with ketamine cystitis) from Kaohsiung Veterans General Hospital in Taiwan. -

Acute Nephritis. (Diffuse)
Postgrad Med J: first published as 10.1136/pgmj.13.136.39 on 1 February 1937. Downloaded from February, 1937 CLASSIFICATION OF NEPHRITIS 39 CLASSIFICATION OF NEPHRITIS. By JOHN GRAY, M.D. (Reader in Pathology, British Post-Graduate Medical School.) In some ways, classification of nephritis is a rather discouraging, as well as a difficult, task, for it is likely that with fuller knowledge of causation we will eventually be enabled to improve on and to simplify any classification possible at present. In the meantime, it is very difficult to decide on the respective merits of the numerous classifications suggested. On the other hand, however, it is true that the multiplicity of the terms which have been used to define various groups of nephritic cases rather tends to exaggerate the number of really important differences of opinion. Many opposing terms in use imply little fundamental difference of opinion, and simply indicate a preference for some particular label for a given type of case. On many points there is, except for this question of nomenclature, fairly general agreement, and it is perhaps as well to begin by indicating some of these, before entering on any discussion of those of a more controversial nature. Few, for instance, would object to the statement that the terms acute, sub- acute, and chronic nephritis provide a useful primary grouping for the majority Protected by copyright. of cases of true nephritis; nor, one thinks, would many take exception to the statement that, of the allied diseases which must be considered with nephritis, easily the most important is non-nephritic hypertension-whatever term is used to describe that condition. -

Path Renal Outline
Path Renal Outline Krane’s Categorization of Disease + A lot of Extras Kidney Disease Acute Renal Failure Intrinsic Kidney Disease Pre‐Renal Renal Intrinsic Post‐Renal Sodium Excretion <1% Glomerular Disease Tubulointerstitial Disease Sodium Excretion < 1% Sodium Excretion >2% Labs aren’t that useful BUN/Creatinine > 20 BUN/Creatinine < 10 CHF, Cirrhosis, Edema Urinalysis: Proteinuria + Hematuria Benign Proteinuria Spot Test Ratio >1.5, Spot Test Ratio <1.5, Acute Tubular Acute Interstitial Acute 24 Urine contains > 2.0g/24hrs 24 Urine contains < 1.0g/24hrs Necrosis Nephritis Glomerulonephritis Nephrotic Syndrome Nephritic Syndrome Inability to concentrate Urine RBC Casts Dirty Brown Casts Inability to secrete acid >3.5g protein / 24 hrs (huge proteinuria) Hematuria and Proteinuria (<3.5) Sodium Excretion >2% Edema Hypoalbuminemia RBC Casts Hypercholesterolemia Leukocytes Salt and Water Retention = HTN Focal Tubular Necrosis Edema Reduced GFR Pyelonephritis Minimal change disease Allergic Interstitial Nephritis Acute Proliferative Glomerulonephritis Membranous Glomerulopathy Analgesic Nephropathy Goodpasture’s (a form of RPGN) Focal segmental Glomerulosclerosis Rapidly Progressive Glomerulonephritis Multiple Myeloma Post‐Streptococcal Glomerulonephritis Membranoproliferative Glomerulonephritis IgA nephropathy (MPGN) Type 1 and Type 2 Alport’s Meleg‐Smith’s Hematuria Break Down Hematuria RBCs Only RBC + Crystals RBC + WBC RBC+ Protein Tumor Lithiasis (Stones) Infection Renal Syndrome Imaging Chemical Analysis Culture Renal Biopsy Calcium -

Management of the Nephrotic Syndrome GAVIN C
Arch Dis Child: first published as 10.1136/adc.43.228.257 on 1 April 1968. Downloaded from Personal Practice* Arch. Dis. Childh., 1968, 43, 257. Management of the Nephrotic Syndrome GAVIN C. ARNEIL From the Department of Child Health, University of Glasgow The nephrotic syndrome may be defined as gross (3) Idiopathic nephrosis. This may be re- proteinuria, predominantly albuminuria, with con- garded either as a primary disease, or as a secondary sequent selective hypoproteinaemia; usually accom- disorder, with the primary cause or causes still panied by oedema, ascites, and hyperlipaemia, and unknown. It is the common form of nephrosis in sometimes by systemic hypertension, azotaemia, or childhood, but the less common in adult patients. excessive erythrocyturia. Unless otherwise specified, the present discussion concerns idiopathic nephrosis. Grouping of Nephrotic Syndrome The syndrome falls into three groups. Assessment of the Case Full history and examination helps to exclude (1) Congenital nephrosis. A group of dis- many secondary forms of the disease. Blood orders present at and presenting soon after birth, pressure is recorded employing as broad a cuff as which are familial and may be acquired or inherited. practicable, and the width of the cuff used is Persistent oedema attracts attention in the first recorded as of importance in comparative estima- weeks of life. The disease may be rapidly lethal, tions. A careful search for concomitant infection but occasionally the patient will survive for a year is made, particularly to exclude pneumococcal copyright. or more without fatal infection or lethal azotaemia. peritonitis or low grade cellulitis. In a patient The disease pattern tends to run true within a previously treated elsewhere, evidence of steroid family. -

Nephritic Syndrome and Membranoproliferative Glomerulonephritis
Nephritic Syndrome and Membranoproliferative Glomerulonephritis Excerpts of Renal Pathophysiology Synopsis of Nephritic Syndrome and Membranoproliferative Glomerulonephritis (MPGN) 6. What are the major causes of nephritic syndrome? Your patient is an 18 year-old woman who is seen for the complaint of occasional vomiting, back pain, swollen ankles, and oliguria. She has a 4-year history of P____________________________________ arthritic joint pain. She previously tested positive for I ____________________________________ serum antinuclear antibody (ANA). On examination she G____________________________________ has a blood pressure of 160/90 mmHg. Urinalysis is Rapidly progresses__________________ significant for hematuria, and serology shows high BUN to and creatinine levels. To confirm your clinical suspicion, you schedule her for renal biopsy and H____________________________________ immunofluorescence evaluation. Results of the biopsy A____________________________________ show a tram-track appearance of the glomerular M____________________________________ basement membrane and sub-endothelial deposits of immune complexes. 1. It is apparent that the patient has renal disease. Which of the two patterns of renal disease, nephrotic or nephritic, is supported by the given findings? _______________________________________ _______________________________________ Hematuria! 2. What is the classic triad of nephritic syndrome? PIG Rapidly Progresses to HAM! _______________________________________ _______________________________________ "If slaughterhouses -

Chapter 10: Radiation Nephropathy
Chapter 10: Radiation Nephropathy † Amaka Edeani, MBBS,* and Eric P. Cohen, MD *Kidney Diseases Branch, National Institute of Diabetes and Digestive and Kidney Diseases, National Institutes of Health, Bethesda, Maryland; and †Nephrology Division, Department of Medicine, University of Maryland School of Medicine, and Baltimore Veterans Affairs Medical Center, Baltimore, Maryland INTRODUCTION Classical radiation nephropathy occurred after external beam radiation for treatment of solid The occurrence of renal dysfunction as a consequence cancers such as seminomas (6); the incidence has of ionizing radiation has been known for more than declined with the advent of more effective chemo- 100 years (1,2). Initial reports termed this condition therapy. In recent years, radiation nephropathy has “radiation nephritis,” but that is a misnomer, because occurred due to TBI used as part of chemo-irradiation it is not an inflammatory condition. Renal radiation conditioning just before hematopoietic stem cell injury may be avoided by the exclusion of an ade- transplantation (HSCT) and also from targeted ra- quate volume of kidney exposure during radiation dionuclide therapy used for instance in the treatment therapy, but the kidneys’ central location can make of neuroendocrine malignancies. TBI may be myelo- this difficult to impossible when tumors of the abdo- ablative or nonmyeloablative, with myeloablative men or retroperitoneum are treated, or during total regimens using radiation doses of 10–12 Gy to de- body irradiation (TBI) (3). stroy or suppress the recipient’s bone marrow. These doses are given in a single fraction or in nine fractions over 3 days (4). In addition, TBI for bone marrow BACKGROUND/CLINICAL SIGNIFICANCE transplantation (BMT) is preceded or accompanied by cytotoxic chemotherapy, which potentiates the Radiation nephropathy is renal injury and loss of effects of ionizing radiation (7). -

Kidney Disease: the Basics
Kidney Disease: The Basics Note: Footnotes in body text may not run sequentially due to ongoing updates. However, they do correspond correctly to the numbers in the reference list. Fast Facts Kidney disease, also known as chronic kidney disease or CKD, causes more deaths than breast cancer or prostate cancer (NVS 2021 report of 2018 data).1 It is the under-recognized public health crisis. • Kidney disease affects an estimated 37 million people in the U.S. (15% of the adult population; more than 1 in 7 adults).2,3,4 • Approximately 90% of those with kidney disease don’t know they have it.2 • And 2 of 5 adults with severe kidney disease don’t know they have it.2 • 1 in 3 adults in the U.S. (approximately 80 million) is at risk for kidney disease.2,5 • Kidney disease is more common in women (14%) than men (12%).2 But for every 2 women who develop end- stage kidney disease (ESKD), 3 men’s kidneys fail.2 • Kidney disease is a leading cause of death in the U.S.1,6,7 • About 1 in 2 people with very low kidney function (not on dialysis) don’t know they have kidney disease.2,13 • Approximately 1 in 3 adults with diabetes and 1 in 5 adults with high blood pressure may have kidney disease.2 • COVID-19 is targeting people with kidney disease, kidney transplant patients, and those at risk for kidney disease. [See www.kidney.org/covid-19] What is Kidney Disease? Chronic kidney disease (CKD) means your kidneys are damaged and losing their ability to keep you healthy by filtering your blood. -

People with Lupus Are Much More Likely to Have Kidney Disease Than People Who Don't Have Lupus
Lupus and kidney disease What does kidney disease have to do with lupus? People with lupus are much more likely to have kidney disease than people who don't have lupus. The kidneys are the organs that make urine. Kidneys filter the blood by putting the waste products into the urine where they can leave the body. Kidney disease can cause blood and protein in the urine, swelling of the body, high blood pressure, and other symptoms. "Lupus nephritis" is the medical name for a type of kidney disease in people with lupus. People who have lupus can also get kidney disease caused by other problems. For example, if someone with lupus also has diabetes, the diabetes might be the cause of kidney problems. The way we find out is by doing a kidney biopsy. Types of Lupus Nephritis: There are several types or “classes” of lupus nephritis. They range from Class I to Class 6: Class 1 disease is mild, Classes 2 and 5 are moderate Classes 3 and 4 are aggressive, Class 6 indicates severe non-reversible disease. What are the symptoms of lupus nephritis? Foamy Urine- This is often one of the first signs of lupus nephritis Blood in the Urine- This is also often one of the first signs of lupus nephritis Swelling- Usually in the legs, feet, or ankles and less often in the hands or face. This tends to worsen as the day progresses or after sitting (this is called edema) High Blood Pressure Changes in Frequency of Urination– Either much more or much less Vomiting- Toxins that build up because the kidney is unable to remove them from the body can result in abnormal function of the liver and the process of digestion. -
Nephritis Fact Sheet
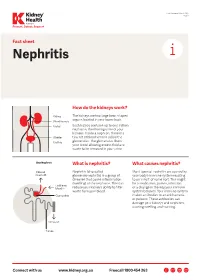
Last Reviewed March 2017 Page 1 Prevent, Detect, Support. Fact sheet Nephritis How do the kidneys work? The kidneys are two large bean-shaped organs located in your lower back. Each kidney contains up to one million nephrons, the filtering units of your kidneys. Inside a nephron, there is a tiny set of blood vessels called the glomerulus. The glomerulus filters your blood allowing excess fluid and waste to be removed in your urine. What is nephritis? What causes nephritis? Nephritis (also called Most types of nephritis are caused by glomerulonephritis) is a group of your body’s immune system reacting diseases that cause inflammation to an ‘insult’ of some sort. This might (swelling) of the nephrons. This can be a medication, poison, infection reduce your kidney’s ability to filter or a change in the way your immune waste from your blood. system behaves. Your immune system makes antibodies to attack bacteria or poisons. These antibodies can damage your kidneys and nephrons, causing swelling and scarring. Connect with us www.kidney.org.au Freecall 1800 454 363 Kidney Health Australia Nephritis Last Reviewed March 2017 Prevent, Detect, Support. Page 2 What are the different types of nephritis? There are many different types of Different types of nephritis include: Nephrotic syndrome: Damage to the nephritis. It can vary from a mild, nephrons causes them to leak large Focal nephritis: Less than a half of non-damaging condition to a serious amounts of protein into your urine your nephrons have scarring, and problem causing kidney failure. Some but little blood. Losing this protein blood and a small amount of protein types of nephritis appear mild at means your body does not have are found in your urine. -

Chronic Kidney Disease in South Carolina
Chronic Kidney Disease in South Carolina WHAT IS KIDNEY DISEASE1? KIDNEY DISEASE IN S.C. • Chronic Kidney Disease (CKD) reduces the body’s ability Mortality to filter blood, remove waste and extra water, and keep beneficial electrolytes in balance. • 868 people died from Kidney Disease in 2013 (most recent data available). The mortality rate decreased from • Left untreated, CKD can lead to kidney failure. 19.8 in 2010 to 16.0 in 2013 but still remains above the • When this happens, dialysis or a kidney transplant is the national rate. only option for keeping a person alive. • Deaths from Nephritis, Nephrotic Syndrome, and • Early kidney disease is a silent problem! Nephrosis are the 8th leading cause of death. U.S. STATISTICS • More than 20 million Americans have chronic kidney disease1. • Many more Americans, including anyone with high blood pressure, diabetes, or a family history of kidney disease, are at an increased risk2. • The number of people developing kidney failure has doubled each decade for the last two decades3. • End-Stage Renal Disease (ESRD) resulted in 88,638 deaths in 20124. • Treating Medicare patients aged 65 or older with kidney • Mortality from Kidney Disease for blacks in South disease cost the United States $44.6 billion in 20125. Carolina is more than twice as high as whites. • 47,112 people died from Nephritis, Nephrotic Syndrome, and Nephrosis in 2013 (14.9 per 100,000 population). This was the 9th leading cause of death6. WHO IS AT RISK1? • Diabetes is the most common cause of kidney failure. Approximately 1 out of 3 adults with diabetes has CKD.