Emerging Role of SWI/SNF Complex Deficiency As a Target of Immune
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

CDC2 Mediates Progestin Initiated Endometrial Stromal Cell Proliferation: a PR Signaling to Gene Expression Independently of Its Binding to Chromatin
CDC2 Mediates Progestin Initiated Endometrial Stromal Cell Proliferation: A PR Signaling to Gene Expression Independently of Its Binding to Chromatin Griselda Vallejo1, Alejandro D. La Greca1., Inti C. Tarifa-Reischle1., Ana C. Mestre-Citrinovitz1, Cecilia Ballare´ 2, Miguel Beato2,3, Patricia Saragu¨ eta1* 1 Instituto de Biologı´a y Medicina Experimental, IByME-Conicet, Buenos Aires, Argentina, 2 Centre de Regulacio´ Geno`mica, (CRG), Barcelona, Spain, 3 University Pompeu Fabra (UPF), Barcelona, Spain Abstract Although non-genomic steroid receptor pathways have been studied over the past decade, little is known about the direct gene expression changes that take place as a consequence of their activation. Progesterone controls proliferation of rat endometrial stromal cells during the peri-implantation phase of pregnancy. We showed that picomolar concentration of progestin R5020 mimics this control in UIII endometrial stromal cells via ERK1-2 and AKT activation mediated by interaction of Progesterone Receptor (PR) with Estrogen Receptor beta (ERb) and without transcriptional activity of endogenous PR and ER. Here we identify early downstream targets of cytoplasmic PR signaling and their possible role in endometrial stromal cell proliferation. Microarray analysis of global gene expression changes in UIII cells treated for 45 min with progestin identified 97 up- and 341 down-regulated genes. The most over-represented molecular functions were transcription factors and regulatory factors associated with cell proliferation and cell cycle, a large fraction of which were repressors down-regulated by hormone. Further analysis verified that progestins regulate Ccnd1, JunD, Usf1, Gfi1, Cyr61, and Cdkn1b through PR- mediated activation of ligand-free ER, ERK1-2 or AKT, in the absence of genomic PR binding. -

Mir-376C Promotes Carcinogenesis and Serves As a Plasma Marker for Gastric Carcinoma
RESEARCH ARTICLE miR-376c promotes carcinogenesis and serves as a plasma marker for gastric carcinoma Pei-Shih Hung1, Chin-Yau Chen2, Wei-Ting Chen2, Chen-Yu Kuo3, Wen-Liang Fang4,5, Kuo-Hung Huang4,5, Peng-Chih Chiu5, Su-Shun Lo2,6* 1 Department of Education and Medical Research, National Yang-Ming University Hospital, Yilan, Taiwan, 2 Department of Surgery, National Yang-Ming University Hospital, Yilan, Taiwan, 3 Department of Medicine, National Yang-Ming University Hospital, Yilan, Taiwan, 4 Division of General Surgery, Veterans General Hospital±Taipei, Taipei, Taiwan, 5 Department of Dentistry, National Yang-Ming University Hospital, Yilan, Taiwan, 6 School of Medicine, National Yang-Ming University, Taipei, Taiwan a1111111111 [email protected] a1111111111 * a1111111111 a1111111111 a1111111111 Abstract Gastric carcinoma is highly prevalent throughout the world. Understanding the pathogenesis of this disease will benefit diagnosis and resolution. Studies show that miRNAs are involved in the tumorigenesis of gastric carcinoma. An initial screening followed by subsequent vali- OPEN ACCESS dation identified that miR-376c is up-regulated in gastric carcinoma tissue and the plasma Citation: Hung P-S, Chen C-Y, Chen W-T, Kuo C-Y, of patients with the disease. In addition, the urinary level of miR-376c is also significantly Fang W-L, Huang K-H, et al. (2017) miR-376c increased in gastric carcinoma patients. The plasma miR-376c level was validated as a bio- promotes carcinogenesis and serves as a plasma marker for gastric carcinoma. PLoS ONE 12(5): marker for gastric carcinoma, including early stage tumors. The induction of miR-376c was e0177346. -
HCC and Cancer Mutated Genes Summarized in the Literature Gene Symbol Gene Name References*
HCC and cancer mutated genes summarized in the literature Gene symbol Gene name References* A2M Alpha-2-macroglobulin (4) ABL1 c-abl oncogene 1, receptor tyrosine kinase (4,5,22) ACBD7 Acyl-Coenzyme A binding domain containing 7 (23) ACTL6A Actin-like 6A (4,5) ACTL6B Actin-like 6B (4) ACVR1B Activin A receptor, type IB (21,22) ACVR2A Activin A receptor, type IIA (4,21) ADAM10 ADAM metallopeptidase domain 10 (5) ADAMTS9 ADAM metallopeptidase with thrombospondin type 1 motif, 9 (4) ADCY2 Adenylate cyclase 2 (brain) (26) AJUBA Ajuba LIM protein (21) AKAP9 A kinase (PRKA) anchor protein (yotiao) 9 (4) Akt AKT serine/threonine kinase (28) AKT1 v-akt murine thymoma viral oncogene homolog 1 (5,21,22) AKT2 v-akt murine thymoma viral oncogene homolog 2 (4) ALB Albumin (4) ALK Anaplastic lymphoma receptor tyrosine kinase (22) AMPH Amphiphysin (24) ANK3 Ankyrin 3, node of Ranvier (ankyrin G) (4) ANKRD12 Ankyrin repeat domain 12 (4) ANO1 Anoctamin 1, calcium activated chloride channel (4) APC Adenomatous polyposis coli (4,5,21,22,25,28) APOB Apolipoprotein B [including Ag(x) antigen] (4) AR Androgen receptor (5,21-23) ARAP1 ArfGAP with RhoGAP domain, ankyrin repeat and PH domain 1 (4) ARHGAP35 Rho GTPase activating protein 35 (21) ARID1A AT rich interactive domain 1A (SWI-like) (4,5,21,22,24,25,27,28) ARID1B AT rich interactive domain 1B (SWI1-like) (4,5,22) ARID2 AT rich interactive domain 2 (ARID, RFX-like) (4,5,22,24,25,27,28) ARID4A AT rich interactive domain 4A (RBP1-like) (28) ARID5B AT rich interactive domain 5B (MRF1-like) (21) ASPM Asp (abnormal -

Supplementary Table S4. FGA Co-Expressed Gene List in LUAD
Supplementary Table S4. FGA co-expressed gene list in LUAD tumors Symbol R Locus Description FGG 0.919 4q28 fibrinogen gamma chain FGL1 0.635 8p22 fibrinogen-like 1 SLC7A2 0.536 8p22 solute carrier family 7 (cationic amino acid transporter, y+ system), member 2 DUSP4 0.521 8p12-p11 dual specificity phosphatase 4 HAL 0.51 12q22-q24.1histidine ammonia-lyase PDE4D 0.499 5q12 phosphodiesterase 4D, cAMP-specific FURIN 0.497 15q26.1 furin (paired basic amino acid cleaving enzyme) CPS1 0.49 2q35 carbamoyl-phosphate synthase 1, mitochondrial TESC 0.478 12q24.22 tescalcin INHA 0.465 2q35 inhibin, alpha S100P 0.461 4p16 S100 calcium binding protein P VPS37A 0.447 8p22 vacuolar protein sorting 37 homolog A (S. cerevisiae) SLC16A14 0.447 2q36.3 solute carrier family 16, member 14 PPARGC1A 0.443 4p15.1 peroxisome proliferator-activated receptor gamma, coactivator 1 alpha SIK1 0.435 21q22.3 salt-inducible kinase 1 IRS2 0.434 13q34 insulin receptor substrate 2 RND1 0.433 12q12 Rho family GTPase 1 HGD 0.433 3q13.33 homogentisate 1,2-dioxygenase PTP4A1 0.432 6q12 protein tyrosine phosphatase type IVA, member 1 C8orf4 0.428 8p11.2 chromosome 8 open reading frame 4 DDC 0.427 7p12.2 dopa decarboxylase (aromatic L-amino acid decarboxylase) TACC2 0.427 10q26 transforming, acidic coiled-coil containing protein 2 MUC13 0.422 3q21.2 mucin 13, cell surface associated C5 0.412 9q33-q34 complement component 5 NR4A2 0.412 2q22-q23 nuclear receptor subfamily 4, group A, member 2 EYS 0.411 6q12 eyes shut homolog (Drosophila) GPX2 0.406 14q24.1 glutathione peroxidase -

Functional Haplotypes of ARID4A Affect Promoter Activity and Semen
Animal Reproduction Science xxx (xxxx) xxx–xxx Contents lists available at ScienceDirect Animal Reproduction Science journal homepage: www.elsevier.com/locate/anireprosci Functional haplotypes of ARID4A affect promoter activity and semen quality of bulls Chunhong Yanga,1, Jinpeng Wanga,1, Juan Liua,1, Yan Suna, Yijun Guoa,b, Qiang Jianga, Zhihua Jua, Qican Gaoa,b, Xiuge Wanga, Jinming Huanga, ⁎ Changfa Wanga, a Dairy Cattle Research Center, Shandong Academy of Agricultural Sciences, Jinan 250131, PR China b College of Life Science, Shandong Normal University, Jinan, PR China ARTICLE INFO ABSTRACT Keywords: The AT-rich interaction domain 4 A (ARID4A) has an important role in regulating Sertoli cell Bovine function and male fertility. Its molecular mechanisms, however, remain largely unknown. In this ARID4A study, two single nucleotide polymorphisms (SNPs) (g.53 G > T, ss 1966531596, and SNP g.826 G > A, rs 210809648) were identified in the promoter region of ARID4A in 215 Chinese Haplotype Holstein bulls using polymerase chain reaction (PCR)-restriction fragment length polymorphism Semen quality and created restriction site-PCR. Results revealed that bulls with g.53 G > T-GG and g.826 G > A-G G genotype exhibited higher sperm deformity rate than those with g.53 G > T- TT and g.826 G > A-AA genotype (P < 0.01). Furthermore, three haplotypes (H1 (GG), H3 (TG), H4 (TA)) and six haplotype combinations (H1H1, H1H3, H1H4, H3H3, H3H4, H4H4) were obtained. The bulls with H4H4 exhibited lower sperm deformity rate than those with H1H1 and H1H3 (P < 0.05). In addition, results of bioinformatics analysis revealed that ARID4A has two promoters and that two SNPs of ARID4A are located in transcription factor binding sites. -

Core Circadian Clock Transcription Factor BMAL1 Regulates Mammary Epithelial Cell
bioRxiv preprint doi: https://doi.org/10.1101/2021.02.23.432439; this version posted February 23, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY 4.0 International license. 1 Title: Core circadian clock transcription factor BMAL1 regulates mammary epithelial cell 2 growth, differentiation, and milk component synthesis. 3 Authors: Theresa Casey1ǂ, Aridany Suarez-Trujillo1, Shelby Cummings1, Katelyn Huff1, 4 Jennifer Crodian1, Ketaki Bhide2, Clare Aduwari1, Kelsey Teeple1, Avi Shamay3, Sameer J. 5 Mabjeesh4, Phillip San Miguel5, Jyothi Thimmapuram2, and Karen Plaut1 6 Affiliations: 1. Department of Animal Science, Purdue University, West Lafayette, IN, USA; 2. 7 Bioinformatics Core, Purdue University; 3. Animal Science Institute, Agriculture Research 8 Origination, The Volcani Center, Rishon Letsiyon, Israel. 4. Department of Animal Sciences, 9 The Robert H. Smith Faculty of Agriculture, Food, and Environment, The Hebrew University of 10 Jerusalem, Rehovot, Israel. 5. Genomics Core, Purdue University 11 Grant support: Binational Agricultural Research Development (BARD) Research Project US- 12 4715-14; Photoperiod effects on milk production in goats: Are they mediated by the molecular 13 clock in the mammary gland? 14 ǂAddress for correspondence. 15 Theresa M. Casey 16 BCHM Room 326 17 175 South University St. 18 West Lafayette, IN 47907 19 Email: [email protected] 20 Phone: 802-373-1319 21 22 bioRxiv preprint doi: https://doi.org/10.1101/2021.02.23.432439; this version posted February 23, 2021. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. -

Appendix 2. Significantly Differentially Regulated Genes in Term Compared with Second Trimester Amniotic Fluid Supernatant
Appendix 2. Significantly Differentially Regulated Genes in Term Compared With Second Trimester Amniotic Fluid Supernatant Fold Change in term vs second trimester Amniotic Affymetrix Duplicate Fluid Probe ID probes Symbol Entrez Gene Name 1019.9 217059_at D MUC7 mucin 7, secreted 424.5 211735_x_at D SFTPC surfactant protein C 416.2 206835_at STATH statherin 363.4 214387_x_at D SFTPC surfactant protein C 295.5 205982_x_at D SFTPC surfactant protein C 288.7 1553454_at RPTN repetin solute carrier family 34 (sodium 251.3 204124_at SLC34A2 phosphate), member 2 238.9 206786_at HTN3 histatin 3 161.5 220191_at GKN1 gastrokine 1 152.7 223678_s_at D SFTPA2 surfactant protein A2 130.9 207430_s_at D MSMB microseminoprotein, beta- 99.0 214199_at SFTPD surfactant protein D major histocompatibility complex, class II, 96.5 210982_s_at D HLA-DRA DR alpha 96.5 221133_s_at D CLDN18 claudin 18 94.4 238222_at GKN2 gastrokine 2 93.7 1557961_s_at D LOC100127983 uncharacterized LOC100127983 93.1 229584_at LRRK2 leucine-rich repeat kinase 2 HOXD cluster antisense RNA 1 (non- 88.6 242042_s_at D HOXD-AS1 protein coding) 86.0 205569_at LAMP3 lysosomal-associated membrane protein 3 85.4 232698_at BPIFB2 BPI fold containing family B, member 2 84.4 205979_at SCGB2A1 secretoglobin, family 2A, member 1 84.3 230469_at RTKN2 rhotekin 2 82.2 204130_at HSD11B2 hydroxysteroid (11-beta) dehydrogenase 2 81.9 222242_s_at KLK5 kallikrein-related peptidase 5 77.0 237281_at AKAP14 A kinase (PRKA) anchor protein 14 76.7 1553602_at MUCL1 mucin-like 1 76.3 216359_at D MUC7 mucin 7, -

ARID2 Deficiency Promotes Tumor Progression and Is Associated with Higher
bioRxiv preprint doi: https://doi.org/10.1101/2020.01.10.898726; this version posted January 10, 2020. The copyright holder for this preprint (which was not certified by peer review) is the author/funder, who has granted bioRxiv a license to display the preprint in perpetuity. It is made available under aCC-BY-NC-ND 4.0 International license. ARID2 deficiency promotes tumor progression and is associated with higher sensitivity to PARP inhibition in lung cancer. Thaidy Moreno1, Laura González-Silva1, Beatriz Monterde1, Isabel Betancor-Fernández2, Carlos Revilla1, Antonio Agraz-Doblas1, Javier Freire3, Pablo Isidro4, Laura Quevedo1, Santiago Montes-Moreno3, Laura Cereceda3, Aurora Astudillo4, Berta Casar1,6, Piero Crespo1,6, Cristina Morales Torres5, Paola Scaffidi5,7, Javier Gomez-Roman3, Eduardo Salido2, and Ignacio Varela1* 1) Instituto de Biomedicina y Biotecnología de Cantabria. Universidad de Cantabria-CSIC. Santander, Spain. 2) Departamento de Patología, Centro de Investigación Biomédica en Red de Enfermedades Raras by impairing DNA repair. Importantly, our results indicate that ARID2-deficiency could be(CIBERER). Tenerife, Spain. 3) Servicio de Anatomía Patológica y Biobanco Valdecilla. HUMV/IDIVAL. Santander, Spain. 4) Biobanco del Principado de Asturias (BBPA). Hospital Universitario Central de Asturias. Oviedo, Spain. 5) Cancer Epigenetics Laboratory, The Francis Crick Institute. London, UK. 6) Centro de Investigación Biomédica en Red de Cáncer (CIBERONC) 7) UCL Cancer Institute, London, UK. * To whom correspondence should be addressed: Ignacio Varela Instituto de Biomedicina y Biotecnología de Cantabria Universidad de Cantabria Albert Einstein 22, 39011 Santander Spain. Ph. +34 942203931 Email. [email protected] bioRxiv preprint doi: https://doi.org/10.1101/2020.01.10.898726; this version posted January 10, 2020. -

Epigenetic Driver Mutations in ARID1A Shape Cancer Immune Phenotype and Immunotherapy
Epigenetic driver mutations in ARID1A shape cancer immune phenotype and immunotherapy Jing Li, … , Arul M. Chinnaiyan, Weiping Zou J Clin Invest. 2020;130(5):2712-2726. https://doi.org/10.1172/JCI134402. Research Article Immunology Graphical abstract Find the latest version: https://jci.me/134402/pdf RESEARCH ARTICLE The Journal of Clinical Investigation Epigenetic driver mutations in ARID1A shape cancer immune phenotype and immunotherapy Jing Li,1,2 Weichao Wang,1,2 Yajia Zhang,3 Marcin Cieślik,3,4,5 Jipeng Guo,1,2 Mengyao Tan,3 Michael D. Green,1,2,6 Weimin Wang,1,2 Heng Lin,1,2 Wei Li,1,2 Shuang Wei,1,2 Jiajia Zhou,1,2 Gaopeng Li,1,2 Xiaojun Jing,3 Linda Vatan,1,2 Lili Zhao,7 Benjamin Bitler,8 Rugang Zhang,8 Kathleen R. Cho,3,5 Yali Dou,3,5 Ilona Kryczek,1,2 Timothy A. Chan,9 David Huntsman,10,11 Arul M. Chinnaiyan,3,6,12,13,14 and Weiping Zou1,2,3,5,15 1Department of Surgery, University of Michigan School of Medicine, Ann Arbor, Michigan, USA. 2Center of Excellence for Cancer Immunology and Immunotherapy, University of Michigan Rogel Cancer Center, University of Michigan School of Medicine, Ann Arbor, Michigan, USA. 3Department of Pathology, 4Department of Computational Medicine and Bioinformatics, 5University of Michigan Rogel Cancer Center, and 6Department of Radiation Oncology, University of Michigan School of Medicine, Ann Arbor, Michigan, USA. 7Department of Biostatistics, University of Michigan, Ann Arbor, Michigan, USA. 8Gene Expression and Regulation Program, The Wistar Institute, Philadelphia, Pennsylvania, USA. 9Department of Radiation Oncology, Memorial Sloan Kettering Cancer Center, New York, New York, USA. -

Effects of Targeting the Transcription Factors Ikaros and Aiolos on B Cell Activation and Differentiation in Systemic Lupus Erythematosus
Immunology and inflammation Lupus Sci Med: first published as 10.1136/lupus-2020-000445 on 16 March 2021. Downloaded from Effects of targeting the transcription factors Ikaros and Aiolos on B cell activation and differentiation in systemic lupus erythematosus Felice Rivellese ,1 Sotiria Manou- Stathopoulou,1 Daniele Mauro,1 Katriona Goldmann,1 Debasish Pyne,2 Ravindra Rajakariar,3 Patrick Gordon,4 Peter Schafer,5 Michele Bombardieri,1 Costantino Pitzalis,1 Myles J Lewis 1 To cite: Rivellese F, ABSTRACT Manou- Stathopoulou S, Objective To evaluate the effects of targeting Ikaros and Key messages Mauro D, et al. Effects of Aiolos by cereblon modulator iberdomide on the activation What is already known about this subject? targeting the transcription and differentiation of B- cells from patients with systemic factors Ikaros and Aiolos The transcription factors Ikaros and Aiolos, which lupus erythematosus (SLE). ► on B cell activation and are critical for B cell differentiation, are implicated in Methods CD19+ B- cells isolated from the peripheral differentiation in systemic systemic lupus erythematosus (SLE) pathogenesis. blood of patients with SLE (n=41) were cultured with lupus erythematosus. Targeting Ikaros and Aiolos using the cereblon mod- TLR7 ligand resiquimod ±IFNα together with iberdomide ► Lupus Science & Medicine ulator iberdomide has been proposed as a promising 2021;8:e000445. doi:10.1136/ or control from day 0 (n=16). Additionally, in vitro B- cell therapeutic agent. lupus-2020-000445 differentiation was induced by stimulation with IL-2/IL-10/ IL-15/CD40L/resiquimod with iberdomide or control, given What does this study add? at day 0 or at day 4. -
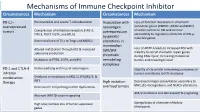
Mechanisms of Immune Checkpoint Inhibitor Circumstances Mechanism Circumstances Mechanism
Mechanisms of Immune Checkpoint Inhibitor Circumstances Mechanism Circumstances Mechanism PD-L1– Nonreversible and severe T-cell exhaustion Association with Loss-of-function mutations in chromatin overexpressed neoantigen remodeler genes (PBRM1, ARID2 and BRD7) tumors Coexpression of inhibitory receptors (LAG-3, overexpression sensitize tumors to ICB and increase TIM-3, TIGIT, VISTA, and BTLA) accessibility to regulatory elements of IFN-γ– by genetic inducible genes. Decreased ratio of TILs to Tregs and MDSCs alterations in mammalian Loss of ARID1A leads to increased MSI with Altered metabolism through IDO & increased SWI/SNF adenosine production inability to recruit mismatch repair genes chromatin during DNA repair, increasing mutational Mutations in PTEN, EGFR, and MYC remodeling burden and neoantigen load. complexes PD-1 and CTLA-4 Immunoediting with loss of neoantigens Stability of chromatin remodeling complexes in inhibitor tumors contributes to ICB resistance combination Deletions or mutations in JAK1/2, IFNGR1/2, & therapy IRF1 High mutation Decreased antigen presentation secondary to MHC, β2-microglobulin, and NLRC5 alterations Decreased T-cell priming and DC dysfunction overload tumors AK1/2 mutations and decreased IFN-γ signaling Aberrant WNT/β-catenin signaling High copy number loss of tumor suppressor Upregulation of alternate inhibitory genes checkpoints Mechanism of Drug Resistance ctDNA for MRD in Colon Cancer ctDNA for MRD in Colon Cancer Factors associated with TTR From Cancer Stem Cell to See the Future Research in Colorectal Cancer Colon Cancer has the Characteristics and Advantages of both Stemness of Cancer Cell and Intestinal System CSC + ISC CCSC Cancer Stem Cell • Possess special biological properties • Very Important to understand the cellular • Long-term self-renewal capacity survival mechanisms • Multi-lineage differentiation • To eradicate cancer stem cells and • Resistance to conventional preventing chemotherapy and radiotherapy chemotherapy and radiotherapy resistance. -
RESEARCH ARTICLE Analysis of ARID2 Gene Mutation in Oral
DOI:10.22034/APJCP.2017.18.10.2679 ARID2 in Oral Squamous Cell Carcinoma RESEARCH ARTICLE Analysis of ARID2 Gene Mutation in Oral Squamous Cell Carcinoma Lakshmi Prabha Das1*, Raghuram Hari Pitty1, Kannan Asokan1, Krithika C-L1, Anandi M-S1, Arvind Ramanathan2 Abstract Background: The ARID2 gene, encoding a sub unit of the chromatin remodelling complex, has a possible tumour suppressor function and has been found to be frequently mutated in various tumours, including gingivo buccal oral squamous cell carcinomas. The present study was designed to analyse the presence of ARID2 gene mutations in the distinct genetic South Indian (Dravidian) population. Materials and Methods: Genomic DNA from thirty biopsy tissue samples of histopathologically confirmed cases of oral squamous cell carcinoma (OSCC) were subjected to PCR amplification with intronic primers encompassing exons 19 and 20 of ARID2. Subsequently, the PCR amplicons were purified and subjected to Sanger sequencing using forward primers for analysis of mutational status. Results: Our study yielded a 6% occurrence of mutations in the ARID2 gene among the thirty OSCC samples. Two samples showed a C(5174)A nonsense mutation whereby the “C” nucleotide was substituted with an “A” nucleotide at position 5174, resulting in the conversion of serine amino acid at codon 1725 to a premature STOP codon. Conclusion: Identification of ARID2 gene mutations in OSCCs in this distinct ethnic population reaffirms that aberrations in the chromatin remodelling complex could indeed also contribute to tumorigenesis, thus providing new insights for future research. Keywords: Oral squamous cell carcinoma- ARID2- chromatin remodelling complex- PBAF- mutation Asian Pac J Cancer Prev, 18 (10), 2679-2681 Introduction therapies and also predict responses to various treatment modalities (Bhatt et al., 2010).