Anterior Fontanelle Pressure Monitoring in Infants
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Unclaimed Capital Credits 121919.Xlsx
Name City State (MORGAN)VANPELT LORI A LAUREL DE 1600 LIMITED PARTNERSHI LEWES DE 1ST HORIZON HOME LOANS IRVING TX 1ST STATE CIGARRETT OUT LEWES DE HARBESO 1ST STATE HOMES INC DE N GEORGET 1ST STATE TECHNOLOGIES DE OWN MILLSBOR 310 A BUILDERS DE O 72 DEVELOPMENT PARTNERS FELTON DE SELBYVILL A & A AIR SERVICES INC DE E A & A FARMS SEAFORDDE A C C BUILDERS INC SMYRNA DE GREENVIL A G B INC DE LE SELBYVILL A GOOD SIGN LLC DE E A K M GROUP LLC NEWARK DE CAMDEN A M T WYOMIN DE G GREENWO A P RENTALS LLC DE OD A TO Z BUILDERS LEWES DE A TO Z MOBILE HOME PARK DOVER DE A+ AUTO BROKERS FELTON DE HARBESO A-1 FIBERGLASS DE N AADLAND DIANE L DOVER DE AAHKEEL BENJAMIN A SMYRNA DE ROCKFOR AARON GARY S TN D WASHING AARONSON NANCY S DC TON AASEBO ARNVID MILTON DE REHOBOT AASEBO ARNVID DE H BCH QUEENST ABA ASSOCIATE MD OWN ABACHNOU SABAH LEWES DE MAGNOLI ABAT EDRIS A DE A ABATE SAMUEL MILTON DE ABBATE JOSEPH DOVER DE ABBATE JOSEPH HARTLY DE ABBATE ANGELO MILFORDDE ARLINGTO ABBENANTE THOMAS VA N ABBEY DEBORAH A CLAYTON DE GEORGET ABBOTT ALEXANDER K DE OWN ABBOTT ANN R SEAFORD DE MILLSBOR ABBOTT BARBARA R DE O ABBOTT BRADY M DOVER DE ELLENDAL ABBOTT CLARK DE E NEW ABBOTT CORDELL A DE CASTLE REHOBOT ABBOTT FRANK H DE H BEACH ABBOTT FRED A EVERETT PA GEORGET ABBOTT GERALD L DE OWN ALTAMON ABBOTT GREGREY A TE FL SPRINGS WILMING ABBOTT HELEN DE TON HOBGOO ABBOTT HELEN G NC D ABBOTT HOWARD NJR DOVER DE ABBOTT JAMES EJR MILFORD DE ABBOTT JANET L SEAFORD DE ABBOTT JOHN L LEWES DE ABBOTT JOSEPH W LAUREL DE NEW ABBOTT KENNETH R DE CASTLE ABBOTT MARGARET HARTLY DE -

IAIS Abstracts Melbourne 2005
Book of Abstracts List of Committees Organising Committee Steering Committee Chairs Ian Adcock, UK John Hamilton, Australia Ian Ahnfelt-Ronne, Denmark Eric Morand, Australia Gareth Bowen, UK Michel Chignard, France Gary Anderson, Australia John Hamilton, Australia Gareth Bowen, UK Gordon Letts, USA Andrew Cook, Australia Lisa Marshall, USA Michael Hickey, Australia Tineke Meijers, Canada Gordon Letts, USA Tatsutoshi Nakahata, Japan Alan Lewis, USA Wim van den Berg, The Netherlands Lisa Marshall, USA Kouji Matsushima, Japan Amy Roshak, USA Glen Scholz, Australia Ross Vlahos, Australia Young Investigator Award Committee Program Committee Chair: Chair: Glen Scholz, Australia Michael Hickey, Australia Laurent Audoly, Canada Andrew Cook, Australia Susan Brain, UK John Hamilton, Australia John Schrader, Canada Lisa Marshall, USA Vincent Lagente, France Eric Morand, Australia Kouji Matsushima, Japan Glen Scholz, Australia Ross Vlahos, Australia For enquiries after the Congress please contact the Congress Secretariat: ICMS Pty Ltd Attention: 7th World Congress on Infl ammation 2005 84 Queensbridge Street Southbank Vic 3006 Australia P: +61 3 9682 0244 F: +61 3 9682 0288 E: infl [email protected] W: www.infl ammation2005.com Contents Sunday 21 August 2005 Abstract No. Page Title Morning 1001 — Plenary 1: Peter Doherty 1002 -1004 — Symposium 1: Chronic Obstructive Pulmonary Disease 1005 - 1008 S 85 Symposium 2: Arthritis Afternoon 1010 - 1013 S 85 Focus Group 1: Understanding Infl ammation through Genetics, Genomics and Proteomics 1014 - 1018 S 86 Focus Group 2: Asthma 1019 - 1022 S 88 Focus Group 3: The Immunoregulatory Response 1023 -1027 S 89 Focus Group 4; Structure-Based Drug Design 1028 - 1032 S 90 Focus Group 5: Chronic Obstructive Pulmonary Disease 1033 - 1037 S 90 Focus Group 6: Rheumatic Diseases Monday 22 August 2005 Abstract No. -

Rev. Richard R. Hanner Training
.... '. College Band To .G.ive ,. Lenny Chappell Scores ·First Fo~;ll c~ncert · ·t·~·~.·.' 38 Points As Deacons -u Defeat ·Duke, 103-89 Of Season -~(Thursday- lnrk Page, Three . Page Seven * * Wake Forest College, Wiliston-Salem, North Ca~lina, Monday, February 20, 19. * * NUIUBER 17 ~------------~----- lr .· 1Wake. 'Forest faculty; App;rove~: Resolution ' ' Whi~h Mtiy Direc~ Immediate Desegregation f ' ·Action Is Focused Claims Roebuck ' ' Death On Young .African By GEORGE WILLIAMSON OGBcB COLUMNIST • In a historic meeting last Monday, the Wak~ Forest faculty passed a resolution that may lead to the immediate- desegregation of the College. · . · The vote was prompted by the report of a faculty com-' mittee that had been investigating the possibilities of inte gration, and •by the efforts of several students to have an African prep school graduate enrolled. -----=-------:-.---- The final decision on College phlicy must come from the board of: trustees, which does not meet WF Station again until April.. And tb:e final decision on the ap Receives plication of the Mrican'student will be in the hands of the Admissions Transmitter A Saturday morning check with Bilf Starlfug, director ·of admis Long-awaited delivery of a trans sions at the College, revealed that mitter to WFDD last week has Reynolds' application is being made it :pOssible for the College kept on file and will not undergo radio start:ion to spe€d up plans in . ',• further processing until after the making a changeover to FM broad faculty resolution has been con IT WASN'T PLANNED THIS WAY BUT.....;.Ughts bumed late and long in 'the Old GOld and office Sun casting. -
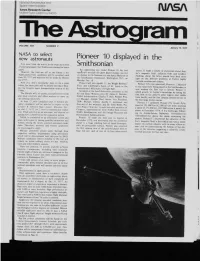
Pioneer 10 Displayed in the Smithsonian
NallOJ1~tlAeroJ I~]tlh(]s and St)riceAdnllrllstrailon Ames ResearchCenter blofletlF lelCl Calitomla 94(.)55 VOLUME XIX NUMBER 7 January13,1977 NASA to select new astronauts Pioneer10 displayedin the Smithsonian An e~:gineering:est mode} Pioneer ]0, die fir~: moons It made a variet~ of discoveriesabout Jupi- ,,pa¢~’craftto reach the giant p]anel Jupiter. ",,,’as I’,Ul ter’s magnetic field, radiationbelts and weather. on displa.,,m the NalionalAir and Space Museum el Findings about the latter >hould help shed more the Smithsonian Institution, Washington. D.( . on lighl on the d{fficuh problems of Earth"s highly Monday. Jan l0 unstable’,~eather and climate. Pioneerwill .ioiii ApolloI I. the Wright Brothers Pioneer10% twin spacecralt.Pioneer I I. iden:i,¢al [:lyer and Lindbergh’s Spirit of St LoLds in the tn the spacecral!being p~aced m the Smiihsonian.is Smilhsonian’~Mi]¢shmes of ::]ighlHall. now making the first trip Io Saitlrn. Pioneer 11 Speaker>aa the, brief dedicationceremonl, at the added greatly Io Jupiter’_*knowledge b3 taking the Air and Space MtlSei.lll:were Dr Jail:asC. Flelcher. first look at ~.he planet’spolar regions{not visible NASA A,dniinis{rat{~r:Charles F tlal}.Pioneer Pr(n- ~rom Eaethi.and the l’/rs{closenp pictures of two of e~l Manager; Adolph Thic] Senior Vice Prc~idenl. the four large Jovian me<ms TRla Michael f’ollms. Apollo If As{ronaul and Pioneer II surpassed Pioneer 10"s record flyb) Director of the m:lxeum: and l)r John Wolle. Pio- speed of" 131.000km (82.000rail per hour. -

Deadly Flavor Technical Repor
Written by: Ashley Grant, MPH Caitlin Weiger, MHS Mark Spires, MPH Joanna Cohen, PhD Produced June 2017 by: Institute for Global Tobacco Control Johns Hopkins Bloomberg School of Public Health 2213 McElderry St., Fourth Floor Baltimore, MD 21205 USA www.jhsph.edu/igtc www.globaltobaccocontrol.org Acknowledgements The Institute for Global Tobacco Control (IGTC) at the Johns Hopkins Bloomberg School of Public Health (JHSPH) wishes to acknowledge Aliança de Promoçao da Sáude, Comisión Nacional Permanente de Lucha Antitabáquica, Educación Popular en Salud, Fundación InterAmericana del CoraZón Argentina, and the Fundación InterAmericana del CoraZón Bolivia for their assistance with data collection, and the Campaign for Tobacco-Free Kids for facilitating work between IGTC and the organiZations listed above and for providing background information. IGTC also thanks Teresa DeAtley for leading the training in Chile and Joanna LopeZ for leading the trainings in Bolivia and Peru. This work was supported with funding from Bloomberg Philanthropies’ Bloomberg Initiative to Reduce Tobacco Use (www.bloomberg.org). Copyright 2017 Institute for Global Tobacco Control Suggested Citation: Institute for Global Tobacco Control. Technical Report on Flavored Cigarettes at the Point-of-Sale in Latin America: Availability and Marketing around Primary and Secondary Schools in Five Countries. Baltimore, MD: Johns Hopkins Bloomberg School of Public Health; June 2017. For more information, please contact: [email protected] Flavored Cigarettes at the POS in Latin America -

304Th MEETING of the BOARD of DIRECTORS
304th MEETING OF THE BOARD OF DIRECTORS 18th OCTOBER 2019 Please note that John Phillips and Michael Flanigan of auditors CW Stirling will attend the Board meeting at 8.00am 10th October 2019 To: N. Horton J. Gole D. Coombes B. Lipmann R. Rosewarne G. Mansour C. Pearce I. Davidoff I. Winter S. Phillips C.C.: M. Deschepper H. Small NOTICE OF THE THREE HUNDRED AND FOURTH MEETING OF THE BOARD OF WINTRINGHAM TO BE HELD AT 136 MT ALEXANDER RD, FLEMINGTON ON WEDNESDAY 7TH AUGUST, 7.30am to 9.00am Enclosed: 1. Agenda for Meeting No. 304 2. Draft Minutes of Wintringham Board Meeting No. 303 3. Board Action Item schedule 4. 2019 Calendar of events 5. Chief Executive Officer’s Report 6. Operational Risk Report 7. Finance Report 8. Selected Correspondence and Attachments Wintringham Activities/Projects List of Acronyms and Definitions 1 WINTRINGHAM BOARD OF DIRECTORS’ MEETING No. 304 TO BE HELD ON FRIDAY 18TH OCTOBER 2019 Item Agenda item Attach Time 1 Present 7.30 2 Apologies 3 Approval of Minutes of Meeting 303 Yes 4 Board Action Item schedule Yes 5 2019 Board Calendar Yes 6 Company secretarial matters 6.1 Declarations of interest 6.2 Director’s attendance (annual declaration) Yes 6.3 Christmas hamper presentations – board attendance Yes 7 Significant items of business 7.1 Financial Statements Yes and (to be considered jointly with Wintringham Housing Limited) separate PDF (includes minutes of the Finance & Risk Committee meeting to review the financial statements) Yes 7.2 CEO/DCEO declaration in relation to the financial statements Yes 7.3 Management representation letter Yes 7.4 Resolutions for 2018/2019 financial statements 8 Chief Executive Officer’s Report Yes Royal Commission submission Separate PDF 9 Operational Risk Report Yes 10 Contemporary topic for Board discussion None this month 11 Finance Report Yes Finance and Risk Committee meeting minutes – refer 7.1 12 Other Business 12.1 Review of Auditor engagement Yes 12.2 Residential funding model overview Yes 12.3 Board policy review separate PDF 13 Meeting close 9.00 2 MEETING Wintringham Board Meeting No. -

OTP Wholesalers
OTP Wholesalers November 07, 2017 Owner Information Business Information Permit Number 4700114 A & E WHOLESALE OF NORTH FLORIDA, LLC A & E WHOLESALE OF NORTH FLORIDA, LLC POST OFFICE BOX 21 1023 CAPITAL CIRCLE NW TALLAHASSEE, FL 32302 TALLAHASSEE, FL 32304 Permit Number 6200236 A & J DISTRIBUTING CORP A & J DISTRIBUTING CORP 3880 69TH AVE 3880 69TH AVE PINELLAS PARK, FL 33781 PINELLAS PARK, FL 33781 Permit Number 5800250 ABC LIQUORS INC ABC LIQUORS INC PO BOX 593688 8989 SOUTH ORANGE AVENUE ORLANDO, FL 32859-3688 ORLANDO, FL 32824 Permit Number 2600353 ADEL WHOLESALE ADEL WHOLESALE 2500 CHARLEVOIX ST 2500 CHARLEVOIX ST JACKSONVILLE, FL 32206 JACKSONVILLE, FL 32206 Permit Number 3900610 ALFA DISTRIBUTING INC ALFA DISTRIBUTING INC 18103 REGENTS SQ DRIVE 18103 REGENTS SQ DRIVE TAMPA, FL 33647 TAMPA, FL 33647 Permit Number 3900605 ALKEIF COFFEE & SMOKE SHOP ALKEIF COFFEE & SMOKE SHOP 4815 E. BUSCH BLVD. 110 BUTLER RD SUITE 103 BRANDON, FL 33511 TAMPA, FL 33617 Permit Number 7900040 ALTADIS U.S.A., INC. ALTADIS U.S.A., INC. 5900 N ANDREWS AVE 600 PERDUE AVENUE FORT LAUDERDALE, FL 33309 RICHMOND, VA 23224 Permit Number 3900405 ALTADIS USA INC ALTADIS USA INC 5900 N ANDREWS AVE 2601 H. TAMPA EAST BLVD FORT LAUDERDALE, FL 33309 TAMPA, FL 33619 Permit Number 3900598 AMERICAN COMMERCIAL GROUP LLC AMERICAN COMMERCIAL GROUP LLC 12634 NICOLE LN 5705 HANNA AVE TAMPA, FL 33625 TAMPA, FL 33610 Page 1 of 24 OTP Wholesalers November 07, 2017 Owner Information Business Information Permit Number 7900073 ANDALUSIA DISTRIBUTING CO INC ANDALUSIA DISTRIBUTING CO INC P O BOX 51 115 ALLEN AVE ANDALUSIA, AL 36420 ANDALUSIA, AL 36420 Permit Number 1614252 ASSOCIATED GROCERS OF FLORIDA INC ASSOCIATED GROCERS OF FLORIDA INC 1141 SW 12TH AVE 1141 SW 12TH AVE POMPANO BEACH, FL 33069 POMPANO BEACH, FL 33069 Permit Number 7900030 ATLANTIC DOMINION DISTRIBUTORS ATLANTIC DOMINION DISTRIBUTORS P.O. -

Tobaccocompaniesbybrand2017 (1)
Geography Category Brand Name (GBO) Company Name (NBO) Data Type 2016 Azerbaijan Cigarettes Viceroy (British American Tobacco Plc) British American Tobacco Azerbaijan MMC Retail Volume 13.0 Azerbaijan Cigarettes Imperial Classic Black (Imperial Brands Plc) Imperial Tobacco MMC Retail Volume 13.0 Azerbaijan Cigarettes LD (Japan Tobacco Inc) JTI Caucasus LLC Retail Volume 8.7 Azerbaijan Cigarettes Winchester (Japan Tobacco Inc) JTI Caucasus LLC Retail Volume 8.6 Azerbaijan Cigarettes Kent (British American Tobacco Plc) British American Tobacco Azerbaijan MMC Retail Volume 7.9 Azerbaijan Cigarettes More (Japan Tobacco Inc) JTI Caucasus LLC Retail Volume 7.5 Azerbaijan Cigarettes Viceroy Lights Blue (British American Tobacco Plc) British American Tobacco Azerbaijan MMC Retail Volume 5.0 Azerbaijan Cigarettes Prima Deluxe (Imperial Brands Plc) Imperial Tobacco MMC Retail Volume 4.4 Azerbaijan Cigarettes West Lights (Imperial Brands Plc) Imperial Tobacco MMC Retail Volume 2.9 Azerbaijan Cigarettes Imperial Classic White (Imperial Brands Plc) Imperial Tobacco MMC Retail Volume 2.4 Azerbaijan Cigarettes Winston (Japan Tobacco Inc) JTI Caucasus LLC Retail Volume 2.0 Azerbaijan Cigarettes Winston Classic (Japan Tobacco Inc) JTI Caucasus LLC Retail Volume 1.7 Azerbaijan Cigarettes Kent Convertibles (British American Tobacco Plc) British American Tobacco Azerbaijan MMC Retail Volume 1.1 Azerbaijan Cigarettes Vogue Superslims Menthe (British American Tobacco Plc) British American Tobacco Azerbaijan MMC Retail Volume 0.9 Azerbaijan Cigarettes Winston -
A U S T R a L I a N B R O a D C a S T I N G a U T H O R I TY Annual Report
Introduction A U S T R A L I A N B R O A D C A S T I N G A U T H O R I TY annual report Sydney 1997 1 Annual Report 1996-97 © Commonwealth of Australia, 1997 ISSN 1320-2863 Design by Media and Public Relations Australian Broadcasting Authority Printed in Australia by Printing Headquarters, Broadway, NSW 2008 For inquiries about this report, contact: Publications Officer Australian Broadcasting Authority at address below For inquiries about information to be made available to Members of Parliament and Senators on request, contact: Director Corporate Services Branch Australian Broadcasting Authority at address below For inquiries relating to Freedom of Information, contact: FOI Officer Australian Broadcasting Authority Level 15, 201 Sussex Street Sydney NSW 2000 Ph. (02) 9334 7700 Fax: (02) 9334 7799 Postal address: PO Box Q500 Queen Victoria Building NSW 1230 E-mail: [email protected] Web site: http://www.dca.gov.au/aba/hpcov.htm 2 Introduction Reserved for letter of transmission 3 Annual Report 1996-97 4 Introduction Table of contents Page no. Letter of transmission 3 Introduction to the report 7 The year in review 8 Corporate overview 16 Performance reporting: Objective 1 — Expert advice 23 International liaison 24 Advice to the government 30 Digital terrestrial television broadcasting 30 Digital radio broadcasting 31 The sixth television channel 32 External liaison 34 Objective 2 — Planning the spectrum 45 Final licence area plans – radio 46 Final licence area plans – television 53 Objective 3 — Licence allocations 56 Allocation of commercial -

Hello, I Have Come Across a Letter Sent from the Office Florida Chief
From: Megan Reeves To: Open Government; Vendor Relations Subject: request for information - Vendor Ownership Survey Date: Thursday, June 25, 2020 12:19:10 PM Hello, I have come across a letter sent from the office Florida Chief Financial Officer Jimmy Patronis. It was addressed to "State of Florida Vendor" and requested responses to a "Vendor Ownership Survey" be sent to the state's vendor relations email address, [email protected]. I am requesting a list of businesses and/or individuals this letter was sent to, as well as the date it was sent and copies of any responses the state has received via email or otherwise. I also am hoping to get an explanation of who ordered the survey and why. Please let me know if you have any questions. Thank you. Megan Megan Reeves Staff writer, health and medicine Tampa Bay Times o: 352-754-6116 | c: 904-298-5213 | f: 352-754-6133 Website: tampabay.com Twitter: @mareevs Facebook: Gradebook by the Tampa Bay Times VENDOR_NM1 SNEADS FFA ALUMNI TREASURY BANK & INVESTMENT UNITED STATES POSTAL SERVICE PAN FOOD STORES HOLIDAY INN EXPRESS SEBRING BECK CHRYSLER DODGE JEEP OF STA 7‐ELEVEN LL BEAN TD BANK NA WALDO COUNTY GENERAL HOSPITAL SOUTHERN MAINE HEALTH CARE THE IRIS NETWORK MAINE COAST REGIONAL HEALTH COMMUNITY HEALTH & COUNSELING EASTERN MAINE HEALTHCARE MERCY HOSPITAL ST MARYS REGIONAL MEDICAL CENTE CALAIS REGIONAL HOSPITAL MOUNT DESERT ISLAND HOSPITAL SWEETSER ST JOSEPH HOSPITAL EASTERN MAINE HEALTHCARE SYSTEM THE BAKER COMPANY, INC BLUE HILL MEMORIAL HOSPITAL INC NORTHEAST HEARING & SPEECH -
Confronting Illicit Tobacco Trade: a Global Review of Country Experiences
: Public Disclosure Authorized Public Disclosure Authorized TRADE Public Disclosure Authorized A GLOBAL REVIEW OF COUNTRY EXPERIENCES Public Disclosure Authorized TECHNICAL REPORT OF THE WORLD BANK GROUP GLOBAL TOBACCO CONTROL PROGRAM. CONFRONTING EDITOR: SHEILA DUTTAA A ILLICIT TOBACCO CONFRONTING ILLICIT TOBACCO TRADE A GLOBAL REVIEW OF COUNTRY EXPERIENCES CONTENTS ACKNOWLEDGMENTS VII EXECUTIVE SUMMARY XI INTRODUCTION XXV THE PROTOCOL TO ELIMINATE ILLICIT TRADE IN TOBACCO PRODUCTS A Global Solution to a Global Problem 1 AUSTRALIA, CANADA, & EUROPE AUSTRALIA Addressing the Illicit Flow of Tobacco Products in Australia 14 CANADA Controlling Illicit Tobacco Trade 50 EUROPEAN UNION Confronting Illicit Tobacco Trade: An Update on EU Policies 72 GEORGIA Controlling Illicit Cigarette Trade 92 IRELAND Addressing the Illicit Flow of Tobacco Products 118 UNITED KINGDOM Tackling Illicit Tobacco 162 III III Confronting Illicit Tobacco Trade: A Global Review of Country Experiences LATIN AMERICA & THE CARIBBEAN ORGANIZATION OF EASTERN CARIBBEAN STATES (OECS) AND TRINIDAD AND TOBAGO Regional Reports on Illicit Tobacco Trade 226 CHILE Tackling the Illicit Tobacco Trade 254 COLOMBIA Illicit Cigarette Trade 292 ECUADOR Addressing Illicit Tobacco Trade 322 MEXICO Controlling the Illicit Cigarette Trade 344 URUGUAY Tackling Illicit Tobacco Trade 364 SOUTH ASIA & EAST ASIA BANGLADESH Illicit Tobacco Trade 406 IV // Contents INDONESIA Tackling Illicit Cigarettes 438 MALAYSIA Addressing the Illicit Flow of Tobacco Products 468 PHILIPPINES Addressing the Illicit -

LE MONDE/PAGES<UNE>
www.lemonde.fr 58 ANNÉE – Nº 17814 – 1,20 ¤ – FRANCE MÉTROPOLITAINE --- DIMANCHE 5 - LUNDI 6 MAI 2002 FONDATEUR : HUBERT BEUVE-MÉRY – DIRECTEUR : JEAN-MARIE COLOMBANI 0123 ARGENT Comment Le retour de Chirac, l’adieu de Jospin compléter Au lendemain du vote du 5 mai, la passation de pouvoirs ira très vite. Notre récit de l’échec du premier ministre ses revenus Le second tour. Le score de l’extrê- f Le score JUSTICE me droite est le principal enjeu du scrutin du 5 mai. Jacques Chirac à de l’extrême droite Châlons avec des jeunes. Jean-Marie est l’enjeu principal Ibrahim Rugova, Le Pen contre la « fraude électora- président du Kosovo, le ». L’ancien président Valéry Gis- du second tour dépose card d’Estaing appelle à voter Chi- rac. Quatre reportages dans quatre f contre Milosevic p. 11 villes, quatre cas d’école pour Qui sont les ENTREPRISES décrypter le vote. p. 2 et 3 électeurs de Chirac et Passation de pouvoirs. Lionel Jos- de Le Pen ? L’agence financière pin doit présenter sa démission lun- Moody’s a dégradé di matin. « Je pars dans la sérénité », f Les équipes qui ont la note de confie le premier ministre. Notre récit inédit du combat manqué de fait les campagnes Vivendi Universal p. 25 Lionel Jospin, victime d’un « acci- dent » politique et du péché d’or- des deux candidats ENCHÈRES gueil. Jacques Chirac entretient l’in- certitude sur le choix de son pre- f Les hypothèses sur Douze monoplaces mier ministre. L’hypothèse Sarkozy et les restes de l’écurie est peu probable.