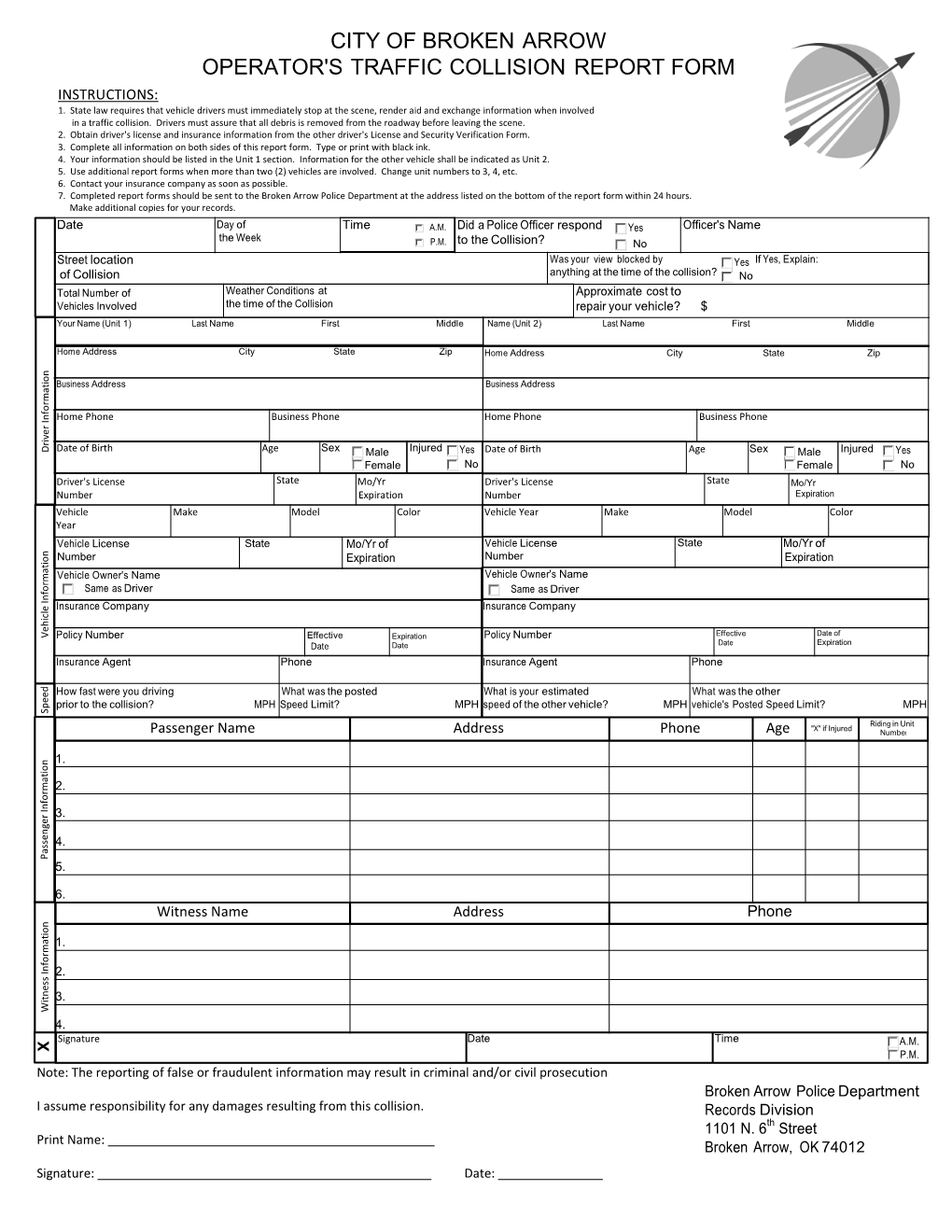
City of Broken Arrow Operator's Traffic
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

Tilde-Arrow-Out (~→O)
Chapter 5: Derivations in Sentential Logic 181 atomic). In the next example, the disjunction is complex (its disjuncts are not atomic). Example 2 (1) (P ´ Q) → (P & Q) Pr (2) •: (P & Q) ∨ (~P & ~Q) ID (3) |~[(P & Q) ∨ (~P & ~Q)] As (4) |•: ¸ DD (5) ||~(P & Q) 3,~∨O (6) ||~(~P & ~Q) 3,~∨O (7) ||~(P ∨ Q) 1,5,→O (8) ||~P 7,~∨O (9) ||~Q 7,~∨O (10) ||~P & ~Q 8,9,&I (11) ||¸ 6,10,¸I The basic strategy is exactly like the previous problem. The only difference is that the formulas are more complex. 13. FURTHER RULES In the previous section, we added the rule ~∨O to our list of inference rules. Although it is not strictly required, it does make a number of derivations much easier. In the present section, for the sake of symmetry, we add corresponding rules for the remaining two-place connectives; specifically, we add ~&O, ~→O, and ~↔O. That way, we have a rule for handling any negated molecular formula. Also, we add one more rule that is sometimes useful, the Rule of Repetition. The additional negation rules are given as follows. Tilde-Ampersand-Out (~&O) ~(d & e) ––––––––– d → ~e Tilde-Arrow-Out (~→O) ~(d → f) –––––––––– d & ~f 182 Hardegree, Symbolic Logic Tilde-Double-Arrow-Out (~±O) ~(d ± e) –––––––––– ~d ± e The reader is urged to verify that these are all valid argument forms of sentential logic. There are other valid forms that could serve equally well as the rules in question. The choice is to a certain arbitrary. The advantage of the particular choice becomes more apparent in a later chapter on predicate logic. -

Proposal to Add U+2B95 Rightwards Black Arrow to Unicode Emoji
Proposal to add U+2B95 Rightwards Black Arrow to Unicode Emoji J. S. Choi, 2015‐12‐12 Abstract In the Unicode Standard 7.0 from 2014, ⮕ U+2B95 was added with the intent to complete the family of black arrows encoded by ⬅⬆⬇ U+2B05–U+2B07. However, due to historical timing, ⮕ U+2B95 was not yet encoded when the Unicode Emoji were frst encoded in 2009–2010, and thus the family of four emoji black arrows were mapped not only to ⬅⬆⬇ U+2B05–U+2B07 but also to ➡ U+27A1—a compatibility character for ITC Zapf Dingbats—instead of ⮕ U+2B95. It is thus proposed that ⮕ U+2B95 be added to the set of Unicode emoji characters and be given emoji‐ and text‐style standardized variants, in order to match the properties of its siblings ⬅⬆⬇ U+2B05–U+2B07, with which it is explicitly unifed. 1 Introduction Tis document primarily discusses fve encoded characters, already in Unicode as of 2015: ⮕ U+2B95 Rightwards Black Arrow: Te main encoded character being discussed. Located in the Miscellaneous Symbols and Arrows block. ⬅⬆⬇ U+2B05–U+2B07 Leftwards, Upwards, and Downwards Black Arrow: Te three black arrows that ⮕ U+2B95 completes. Also located in the Miscellaneous Symbols and Arrows block. ➡ U+27A1 Black Rightwards Arrow: A compatibility character for ITC Zapf Dingbats. Located in the Dingbats block. Tis document proposes the addition of ⮕ U+2B95 to the set of emoji characters as defned by Unicode Technical Report (UTR) #51: “Unicode Emoji”. In other words, it proposes: 1. A property change: ⮕ U+2B95 should be given the Emoji property defned in UTR #51. -

Introducing Sentential Logic (SL) Part I – Syntax
Introducing Sentential Logic (SL) Part I – Syntax 1. As Aristotle noted long ago, some entailments in natural language seem to hold by dint of their “logical” form. Consider, for instance, the example of Aristotle’s being a logician above, as opposed to the “material” entailment considering the relative locations of Las Vegas and Pittsburgh. Such logical entailment provides the basic motivation for formal logic. So-called “formal” or “symbolic” logic is meant in part to provide a (perhaps idealized) model of this phenomenon. In formal logic, we develop an artificial but highly regimented language, with an eye perhaps of understanding natural language devices as approximating various operations within that formal language. 2. We’ll begin with a formal language that is commonly called either Sentential Logic (SL) or, more high- falutinly, “the propositional calculus.” You’re probably already quite familiar with it from an earlier logic course. SL is composed of Roman capital letters (and subscripted capital letters), various operators (or functors), and left and right parentheses. The standard operators for SL include the tilde (~), the ampersand (&), the wedge (v), and the arrow (→). Other operators, such as the double arrow, the stroke and the dagger, can easily be added as the need arises. The Syntax of S.L 3. A syntax for a language specifies how to construct meaningful expressions within that language. For purely formal languages such as SL, we can understand such expressions as well-formed formulas (wffs). The syntax of SL is recursive. That means that we start with basic (or atomic) wffs, and then specify how to build up more complex wffs from them. -

International Language Environments Guide
International Language Environments Guide Sun Microsystems, Inc. 4150 Network Circle Santa Clara, CA 95054 U.S.A. Part No: 806–6642–10 May, 2002 Copyright 2002 Sun Microsystems, Inc. 4150 Network Circle, Santa Clara, CA 95054 U.S.A. All rights reserved. This product or document is protected by copyright and distributed under licenses restricting its use, copying, distribution, and decompilation. No part of this product or document may be reproduced in any form by any means without prior written authorization of Sun and its licensors, if any. Third-party software, including font technology, is copyrighted and licensed from Sun suppliers. Parts of the product may be derived from Berkeley BSD systems, licensed from the University of California. UNIX is a registered trademark in the U.S. and other countries, exclusively licensed through X/Open Company, Ltd. Sun, Sun Microsystems, the Sun logo, docs.sun.com, AnswerBook, AnswerBook2, Java, XView, ToolTalk, Solstice AdminTools, SunVideo and Solaris are trademarks, registered trademarks, or service marks of Sun Microsystems, Inc. in the U.S. and other countries. All SPARC trademarks are used under license and are trademarks or registered trademarks of SPARC International, Inc. in the U.S. and other countries. Products bearing SPARC trademarks are based upon an architecture developed by Sun Microsystems, Inc. SunOS, Solaris, X11, SPARC, UNIX, PostScript, OpenWindows, AnswerBook, SunExpress, SPARCprinter, JumpStart, Xlib The OPEN LOOK and Sun™ Graphical User Interface was developed by Sun Microsystems, Inc. for its users and licensees. Sun acknowledges the pioneering efforts of Xerox in researching and developing the concept of visual or graphical user interfaces for the computer industry. -

MX2 Instruction Manual
RediStart TM Solid State Starter 2 Control RB2, RC2, RX2E Models User Manual 890034-01-02 August 2008 Software Version: 810023-01-08 Hardware Version: 300055-01-05 © 2008 Benshaw Inc. Benshaw retains the right to change specifications and illustrations in text without prior notification. The contents of this document may not be copied without the explicit permission of Benshaw. Important Reader Notice 2 Congratulations on the purchase of your new Benshaw RediStart MX Solid State Starter. This manual contains the information to install and 2 2 program the MX Solid State Starter. The MX is a standard version solid state starter. If you require additional features, please review the 3 expanded feature set of the MX Solid State Starter on page 5. 2 This manual may not cover all of the applications of the RediStart MX . Also, it may not provide information on every possible contingency 2 concerning installation, programming, operation, or maintenance specific to the RediStart MX Series Starters. The content of this manual will not modify any prior agreement, commitment or relationship between the customer and Benshaw. The sales contract contains the entire obligation of Benshaw. The warranty enclosed within the contract between the parties is the only warranty that Benshaw will recognize and any statements contained herein do not create new warranties or modify the existing warranty in any way. Any electrical or mechanical modifications to Benshaw products without prior written consent of Benshaw will void all warranties and may also void cUL listing or other safety certifications, unauthorized modifications may also result in product damage operation malfunctions or personal injury. -
AFT Fathom 11 Quick Start Guide
AFT Fathom™ Quick Start Guide Metric Units AFT Fathom Version 11 Incompressible Pipe Flow Modeling Dynamic solutions for a fluid world ™ CAUTION! AFT Fathom is a sophisticated pipe flow analysis program designed for qualified engineers with experience in pipe flow analysis and should not be used by untrained individuals. AFT Fathom is intended solely as an aide for pipe flow analysis engineers and not as a replacement for other design and analysis methods, including hand calculations and sound engineering judgment. All data generated by AFT Fathom should be independently verified with other engineering methods. AFT Fathom is designed to be used only by persons who possess a level of knowledge consistent with that obtained in an undergraduate engineering course in the analysis of pipe system fluid mechanics and are familiar with standard industry practice in pipe flow analysis. AFT Fathom is intended to be used only within the boundaries of its engineering assumptions. The user should consult the AFT Fathom Help System for a discussion of all engineering assumptions made by AFT Fathom. Information in this document is subject to change without notice. No part of this Quick Start Guide may be reproduced or transmitted in any form or by any means, electronic or mechanical, for any purpose, without the express written permission of Applied Flow Technology. © 2020 Applied Flow Technology Corporation. All rights reserved. Printed in the United States of America. First Printing. “AFT Fathom”, “Applied Flow Technology”, “Dynamic solutions for a fluid world”, and the AFT logo are trademarks of Applied Flow Technology Corporation. Excel and Windows are trademarks of Microsoft Corporation. -

2021 Cadillac XT4 Owner's Manual
21_CAD_XT4_COV_en_US_84533014B_2020OCT27.pdf 1 9/25/2020 1:45:28 PM C M Y CM MY CY CMY K 84533014 B Cadillac XT4 Owner Manual (GMNA-Localizing-U.S./Canada/Mexico- 14584367) - 2021 - CRC - 10/14/20 Introduction model variants, country specifications, Contents features/applications that may not be available in your region, or changes Introduction . 1 subsequent to the printing of this owner’s manual. Keys, Doors, and Windows . 6 Refer to the purchase documentation Seats and Restraints . 36 relating to your specific vehicle to Storage . 84 confirm the features. Instruments and Controls . 90 The names, logos, emblems, slogans, Keep this manual in the vehicle for vehicle model names, and vehicle quick reference. Lighting . 129 body designs appearing in this manual Infotainment System . 136 including, but not limited to, GM, the Canadian Vehicle Owners GM logo, CADILLAC, the CADILLAC Climate Controls . 197 A French language manual can be Emblem, and XT4 are trademarks and/ obtained from your dealer, at Driving and Operating . 203 or service marks of General Motors www.helminc.com, or from: LLC, its subsidiaries, affiliates, Vehicle Care . 281 or licensors. Propriétaires Canadiens Service and Maintenance . 357 For vehicles first sold in Canada, On peut obtenir un exemplaire de ce Technical Data . 370 substitute the name “General Motors guide en français auprès du ” Customer Information . 374 of Canada Company for Cadillac concessionnaire ou à l'adresse Motor Car Division wherever it suivante: Reporting Safety Defects . 384 appears in this manual. Helm, Incorporated OnStar . 387 This manual describes features that Attention: Customer Service Connected Services . 392 may or may not be on the vehicle 47911 Halyard Drive because of optional equipment that Plymouth, MI 48170 Index . -

Unified English Braille (UEB) General Symbols and Indicators
Unified English Braille (UEB) General Symbols and Indicators UEB Rulebook Section 3 Published by International Council on English Braille (ICEB) space (see 3.23) ⠣ opening braille grouping indicator (see 3.4) ⠹ first transcriber‐defined print symbol (see 3.26) ⠫ shape indicator (see 3.22) ⠳ arrow indicator (see 3.2) ⠳⠕ → simple right pointing arrow (east) (see 3.2) ⠳⠩ ↓ simple down pointing arrow (south) (see 3.2) ⠳⠪ ← simple left pointing arrow (west) (see 3.2) ⠳⠬ ↑ simple up pointing arrow (north) (see 3.2) ⠒ ∶ ratio (see 3.17) ⠒⠒ ∷ proportion (see 3.17) ⠢ subscript indicator (see 3.24) ⠶ ′ prime (see 3.11 and 3.15) ⠶⠶ ″ double prime (see 3.11 and 3.15) ⠔ superscript indicator (see 3.24) ⠼⠡ ♮ natural (see 3.18) ⠼⠣ ♭ flat (see 3.18) ⠼⠩ ♯ sharp (see 3.18) ⠼⠹ second transcriber‐defined print symbol (see 3.26) ⠜ closing braille grouping indicator (see 3.4) ⠈⠁ @ commercial at sign (see 3.7) ⠈⠉ ¢ cent sign (see 3.10) ⠈⠑ € euro sign (see 3.10) ⠈⠋ ₣ French franc sign (see 3.10) ⠈⠇ £ pound sign (pound sterling) (see 3.10) ⠈⠝ ₦ naira sign (see 3.10) ⠈⠎ $ dollar sign (see 3.10) ⠈⠽ ¥ yen sign (Yuan sign) (see 3.10) ⠈⠯ & ampersand (see 3.1) ⠈⠣ < less‐than sign (see 3.17) ⠈⠢ ^ caret (3.6) ⠈⠔ ~ tilde (swung dash) (see 3.25) ⠈⠼⠹ third transcriber‐defined print symbol (see 3.26) ⠈⠜ > greater‐than sign (see 3.17) ⠈⠨⠣ opening transcriber’s note indicator (see 3.27) ⠈⠨⠜ closing transcriber’s note indicator (see 3.27) ⠈⠠⠹ † dagger (see 3.3) ⠈⠠⠻ ‡ double dagger (see 3.3) ⠘⠉ © copyright sign (see 3.8) ⠘⠚ ° degree sign (see 3.11) ⠘⠏ ¶ paragraph sign (see 3.20) -

Math Symbol Tables
APPENDIX A Math symbol tables A.1 Hebrew and Greek letters Hebrew letters Type Typeset \aleph ℵ \beth ℶ \daleth ℸ \gimel ℷ © Springer International Publishing AG 2016 481 G. Grätzer, More Math Into LATEX, DOI 10.1007/978-3-319-23796-1 482 Appendix A Math symbol tables Greek letters Lowercase Type Typeset Type Typeset Type Typeset \alpha \iota \sigma \beta \kappa \tau \gamma \lambda \upsilon \delta \mu \phi \epsilon \nu \chi \zeta \xi \psi \eta \pi \omega \theta \rho \varepsilon \varpi \varsigma \vartheta \varrho \varphi \digamma ϝ \varkappa Uppercase Type Typeset Type Typeset Type Typeset \Gamma Γ \Xi Ξ \Phi Φ \Delta Δ \Pi Π \Psi Ψ \Theta Θ \Sigma Σ \Omega Ω \Lambda Λ \Upsilon Υ \varGamma \varXi \varPhi \varDelta \varPi \varPsi \varTheta \varSigma \varOmega \varLambda \varUpsilon A.2 Binary relations 483 A.2 Binary relations Type Typeset Type Typeset < < > > = = : ∶ \in ∈ \ni or \owns ∋ \leq or \le ≤ \geq or \ge ≥ \ll ≪ \gg ≫ \prec ≺ \succ ≻ \preceq ⪯ \succeq ⪰ \sim ∼ \approx ≈ \simeq ≃ \cong ≅ \equiv ≡ \doteq ≐ \subset ⊂ \supset ⊃ \subseteq ⊆ \supseteq ⊇ \sqsubseteq ⊑ \sqsupseteq ⊒ \smile ⌣ \frown ⌢ \perp ⟂ \models ⊧ \mid ∣ \parallel ∥ \vdash ⊢ \dashv ⊣ \propto ∝ \asymp ≍ \bowtie ⋈ \sqsubset ⊏ \sqsupset ⊐ \Join ⨝ Note the \colon command used in ∶ → 2, typed as f \colon x \to x^2 484 Appendix A Math symbol tables More binary relations Type Typeset Type Typeset \leqq ≦ \geqq ≧ \leqslant ⩽ \geqslant ⩾ \eqslantless ⪕ \eqslantgtr ⪖ \lesssim ≲ \gtrsim ≳ \lessapprox ⪅ \gtrapprox ⪆ \approxeq ≊ \lessdot -

View and Use Dingbat Fonts (Windows)
View and Use Dingbat Fonts (Windows) Tip of the Week by Jen White on February 8, 2011 I’m a PC. Always have been. Did you know that Windows comes standard with a Character Map? I didn’t. Do you know what a Character Map is? I didn’t. Well, here’s the low-down on the illusive Character Map... You’re gonna love it! Windows Character Map is a rock solid utility that can be used to copy and paste accented letters, foreign characters, and <tah-dah> dingbats into any Windows application. And the best news of all is... even a dingbat like me can figure it out!! Check it out... Step 1: Open the Map * From the Windows Start Menu, choose: All Programs > Accessories (folder) > System Tools (folder) > Character Map. Can’t find it? No need to panic. Simply open the Start Menu and enter “character map” into the search bar. * If you find the Character Map useful, consider ‘pinning’ it to your Start Menu for easy access. To do that, Right click on Character Map and choose Pin to Start Menu. Step 2: Use the Map * When the Character Map pops up, it will display the last font used. Go ahead and choose a different font - or dingbat as in this case. Tip: If you want to scroll through the fonts just to see what’s available (you’ll be surprised), open the font picker and then close it again. Now use your up and down arrow keys to scroll through your list of installed Page 1 View and Use Dingbat Fonts (Windows), © 2011 Scrapper’s Guide, all rights reserved. -

Unicode Characters in Proofpower Through Lualatex
Unicode Characters in ProofPower through Lualatex Roger Bishop Jones Abstract This document serves to establish what characters render like in utf8 ProofPower documents prepared using lualatex. Created 2019 http://www.rbjones.com/rbjpub/pp/doc/t055.pdf © Roger Bishop Jones; Licenced under Gnu LGPL Contents 1 Prelude 2 2 Changes 2 2.1 Recent Changes .......................................... 2 2.2 Changes Under Consideration ................................... 2 2.3 Issues ............................................... 2 3 Introduction 3 4 Mathematical operators and symbols in Unicode 3 5 Dedicated blocks 3 5.1 Mathematical Operators block .................................. 3 5.2 Supplemental Mathematical Operators block ........................... 4 5.3 Mathematical Alphanumeric Symbols block ........................... 4 5.4 Letterlike Symbols block ..................................... 6 5.5 Miscellaneous Mathematical Symbols-A block .......................... 7 5.6 Miscellaneous Mathematical Symbols-B block .......................... 7 5.7 Miscellaneous Technical block .................................. 7 5.8 Geometric Shapes block ...................................... 8 5.9 Miscellaneous Symbols and Arrows block ............................. 9 5.10 Arrows block ........................................... 9 5.11 Supplemental Arrows-A block .................................. 10 5.12 Supplemental Arrows-B block ................................... 10 5.13 Combining Diacritical Marks for Symbols block ......................... 11 5.14 -

Arrows Range: 2190–21FF
Arrows Range: 2190–21FF This file contains an excerpt from the character code tables and list of character names for The Unicode Standard, Version 14.0 This file may be changed at any time without notice to reflect errata or other updates to the Unicode Standard. See https://www.unicode.org/errata/ for an up-to-date list of errata. See https://www.unicode.org/charts/ for access to a complete list of the latest character code charts. See https://www.unicode.org/charts/PDF/Unicode-14.0/ for charts showing only the characters added in Unicode 14.0. See https://www.unicode.org/Public/14.0.0/charts/ for a complete archived file of character code charts for Unicode 14.0. Disclaimer These charts are provided as the online reference to the character contents of the Unicode Standard, Version 14.0 but do not provide all the information needed to fully support individual scripts using the Unicode Standard. For a complete understanding of the use of the characters contained in this file, please consult the appropriate sections of The Unicode Standard, Version 14.0, online at https://www.unicode.org/versions/Unicode14.0.0/, as well as Unicode Standard Annexes #9, #11, #14, #15, #24, #29, #31, #34, #38, #41, #42, #44, #45, and #50, the other Unicode Technical Reports and Standards, and the Unicode Character Database, which are available online. See https://www.unicode.org/ucd/ and https://www.unicode.org/reports/ A thorough understanding of the information contained in these additional sources is required for a successful implementation.