High B1a0d Pressure and Its Treatment in General
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

DISEASES of ARTERIES ARTERIOSCLEROSIS (“Hardening of the Arteries”): General Term Reflecting Arterial Wall Thickening and Loss of Elasticity
DISEASES OF ARTERIES ARTERIOSCLEROSIS (“hardening of the arteries”): general term reflecting arterial wall thickening and loss of elasticity 3 patterns •Atherosclerosis: involves the the aorta and the large arteries •Mönckeberg sclerosis: calcific deposits in the media of middle-sized arteries in persons >age 50 •Arteriolosclerosis: involves the small arteries and arterioles in association with hypertension or diabetes ATHEROSCLEROSIS Multifactorial, slowly progressive chronic degenerative-inflammatory disease of the aorta and the large arteries, such as • coronary arteries • circle of Willis • popliteal and tibial arteries Significance: > 50% of all death is attributed to atherosclerosis in well-developed countries Morphology Gross • Atheromatous plaque (pathognomic) - raised white-yellow lesion in the intima, protruding into the lumen • Large plaques in the aorta (> 2 cm) contain a yellow, grumous debris (”atheroma” - Greek word for gruel) Atheromatous plaque in the middle cerebral artery: raised white-yellow lesion in the intima, protruding into the lumen (formol-fixed brain) Aorta: the plaques contain a yellow, grumous debris (arrow) Structure of atheroma on LM • Intimal lesion • Central lipid core • Fibrous ”cap” subendothelially Central lipid core composed of lipids, cholesterol clefts, necrotic debris + calcium-salts, surrounded by foamy macrophages, T-lymphocytes, fibroblasts, small capillaries, and collagens and proteoglycans Types of plaques • Vulnerable plaques have large atheromatous cores, increased inflammatory cell content and thin fibrous caps high risk of rupture thrombosis • Stable plaques have minimal atheromatous cores and inflammation and thick fibrous caps 70% stenosis (critical stenosis) chronic ischemia distally Vulnerable plaque in the coronary artery Inflammatory infiltrates and capillaries around the lipid core. Lumen Intima Media Pathogenesis Response to chronic endocardial injury hypothesis • Cholesterol can’t dissolve in the blood. -

441.2.Full.Pdf
Ann Rheum Dis: first published as 10.1136/annrheumdis-2018-eular.4790 on 12 June 2018. Downloaded from Scientific Abstracts Thursday, 14 June 2018 441 All GCA TAK p (n 23) (n 13) (n 8) Female, n (%) 19 (82.6) 12 (92.3) 6 (75) ns Age at diagnosis 63 (51–68) 68 (63–73) 43.5 (30.5–57) 0.003 Diagnostic latency (months) 4.5 (2–12) 3 (2–10) 8 (3.5–12) ns ESR at disease onset (mm/h) 49 (38–68) 52.5 (45.5– 42 (40–61.5) ns 59.7) CRP at disease onset (mg/L) 61.8 (13– 89 (32.5–106) 60.5 (9.3–132.5) ns 132.5) Disease duration at PET/MR 27 (18–36) 24 (13–29.5) 36.5 (14.75– ns (months) 129.3) ESR at examination (mm/h) 18 (9–35) 16 (7–31) 20.5 (11–44.5) ns CRP at examination (mg/L) 4.5 (2.55–8.9) 3.9 (3.48–4.72) 4.55 (2.05–10.4) ns Results: 23 LVV patients were included, 56.5% GCA, 34.8% TAK and 8.7% iso- Results: Among 602 patients with TA during this period, 119 (19.8%) were jTA, lated aortitis, all Caucasian, mostly females (82%). We considered 55 PET scans, while 483 were aTA. Female predominance was less striking in jTA (71.4%) than 32/55 in LVV group (from min. 1 to max. 3 scans/patient) mainly during follow-up aTA (79%), p=0.047. Patients with jTA had presented more commonly with fever (29/32 scans), and 23/55 in control group. -
DSM III and ICD 9 Codes 11-2004
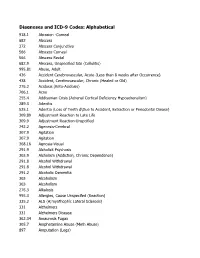
Diagnoses and ICD-9 Codes: Alphabetical 918.1 Abrasion -Corneal 682 Abscess 372 Abscess Conjunctiva 566 Abscess Corneal 566 Abscess Rectal 682.9 Abscess, Unspecified Site (Cellulitis) 995.81 Abuse, Adult 436 Accident Cerebrovascular, Acute (Less than 8 weeks after Occurrence) 438 Accident, Cerebrovascular, Chronic (Healed or Old) 276.2 Acidosis (Keto-Acidosis) 706.1 Acne 255.4 Addisonian Crisis (Adrenal Cortical Deficiency Hypoadrenalism) 289.3 Adenitis 525.1 Adentia (Loss of Teeth d\Due to Accident, Extraction or Periodontal Diease) 309.89 Adjustment Reaction to Late Life 309.9 Adjustment Reaction-Unspcified 742.2 Agenesis-Cerebral 307.9 Agitation 307.9 Agitation 368.16 Agnosia-Visual 291.9 Alcholick Psychosis 303.9 Alcholism (Addiction, Chronic Dependence) 291.8 Alcohol Withdrawal 291.8 Alcohol Withdrawal 291.2 Alcoholic Dementia 303 Alcoholism 303 Alcoholism 276.3 Alkalosis 995.3 Allergies, Cause Unspecifed (Reaction) 335.2 ALS (A;myothophic Lateral Sclerosis) 331 Alzheimers 331 Alzheimers Disease 362.34 Amaurosis Fugax 305.7 Amphetamine Abuse (Meth Abuse) 897 Amputation (Legs) 736.89 Amputation, Leg, Status Post (Above Knee, Below Knee) 736.9 Amputee, Site Unspecified (Acquired Deformity) 285.9 Anemia 284.9 Anemia Aplastic (Hypoplastic Bone Morrow) 280 Anemia Due to loss of Blood 281 Anemia Pernicious 280.9 Anemia, Iron Deficiency, Unspecified 285.9 Anemia, Unspecified (Normocytic, Not due to blood loss) 281.9 Anemia, Unspecified Deficiency (Macrocytic, Nutritional 441.5 Aneurysm Aortic, Ruptured 441.1 Aneurysm, Abdominal 441.3 Aneurysm, -

Echocardiography in Pediatric Pulmonary Hypertension
REVIEW ARTICLE published: 12 November 2014 PEDIATRICS doi: 10.3389/fped.2014.00124 Echocardiography in pediatric pulmonary hypertension Pei-Ni Jone* and D. Dunbar Ivy Pediatric Cardiology, Children’s Hospital Colorado, University of Colorado School of Medicine, Aurora, CO, USA Edited by: Pulmonary hypertension (PH) can be a rapidly progressive and fatal disease. Although Antonio Francesco Corno, Universiti right heart catheterization remains the gold standard in evaluation of PH, echocardiogra- Sains Malaysia, Malaysia phy remains an important tool in screening, diagnosing, evaluating, and following these Reviewed by: Jeffrey Feinstein, Stanford University, patients. In this article, we will review the important echocardiographic parameters of the USA right heart in evaluating its anatomy, hemodynamic assessment, systolic, and diastolic Cecile Tissot, The University function in children with PH. Children’s Hospital, Switzerland Tilman Humpl, SickKids Hospital, Keywords: pediatric pulmonary hypertension, echocardiography, right heart, right ventricular function Canada *Correspondence: Pei-Ni Jone, Pediatric Cardiology, Children’s Hospital Colorado, University of Colorado School of Medicine, 13123 East 16th Avenue, B100, Aurora, CO 80045, USA e-mail: pei-ni.jone@ childrenscolorado.org INTRODUCTION of the RA area in end-systole is performed to evaluate for RA dila- Pulmonary hypertension (PH) is a progressive disease that carries tion (Figure 1)(3). Indexed RA area to body surface area in adult high morbidity and mortality. Although cardiac catheterization is patients with idiopathic PH has been a predictor of mortality and used to define PH, echocardiography is the most important non- has been shown to be a prognostic marker for follow up of PH invasive tool that is used to detect PH (1). -

Effects of Immediate Versus Delayed Antihypertensive Therapy on Outcome in the Systolic Hypertension in Europe Trial Jan A
Original article 847 Effects of immediate versus delayed antihypertensive therapy on outcome in the Systolic Hypertension in Europe Trial Jan A. Staessena, Lutgarde Thijsa, Robert Fagarda, Hilde Celisa, Willem H. Birkenha¨gerb, Christopher J. Bulpittc, Peter W. de Leeuwd, Astrid E. Fletchere, Franc¸oise Forettef, Gastone Leonettig, Patricia McCormackh, Choudomir Nachevi, Eoin O’Brienh, Jose´ L. Rodicioj, Joseph Rosenfeldk, Cinzia Sartil, Jaakko Tuomilehtol, John Websterm, Yair Yodfatn and Alberto Zanchettig, for the Systolic Hypertension in Europe (Syst-Eur) Trial Investigators Background To assess the impact of immediate versus systolic hypertension. Immediate compared with delayed delayed antihypertensive treatment on the outcome of treatment prevented 17 strokes or 25 major cardiovascular older patients with isolated systolic hypertension, we events per 1000 patients followed up for 6 years. These extended the double-blind placebo-controlled Systolic findings underscore the necessity of early treatment of Hypertension in Europe (Syst-Eur) trial by an open-label isolated systolic hypertension. J Hypertens 22:847–857 & follow-up study lasting 4 years. 2004 Lippincott Williams & Wilkins. Methods The Syst-Eur trial included 4695 randomized Journal of Hypertension 2004, 22:847–857 patients with minimum age of 60 years and an untreated Keywords: calcium-channel blocker, clinical trial, isolated systolic blood pressure of 160–219 mmHg systolic and below hypertension, outcome, myocardial infarction, stroke 95 mmHg diastolic. The double-blind -

HYPERTENSION-I by ROBERT PLATE, M.D., M.Sc., F.R.C.P
BRITISH APRIL 22, 1950 HYPERTENSION MEDICAL JOURNAL 951 REFRESHER COURSE FOR GENERAL PRACTITIONERS HYPERTENSION-I BY ROBERT PLATE, M.D., M.Sc., F.R.C.P. Professor of Medicine, University of Manchester Hypertension is a syndrome and not a disease. A large tension in that they developed arteriolar necrosis in various number of cases with high blood pressure fall into the organs, though not, however, in the kidneys, because by the group which is known as primary or essential hypertension. very nature of the experiment the renal arterioles were This means that no pre-existing disease which might have protected from the effects of the high blood pressure. If caused the hypertension can be discovered. In other words, the renal artery of only one kidney was constricted, as Wakerlin (1949) has said, "'Essential hypertension' is hypertension was usually more transient and less severe, a designation born of ignorance and is equivalent to 'fever and if the affected kidney was removed the blood pressure of unknown cause."' Although we are ignorant of the returned to normal. cause of esgential hypertension I believe that it is much Wilson and Byrom (1939) found that severe hypertensiorn more than a merely negative diagnosis, and that it will of the malignant type could be produced in rats by con- turn out to be a definite entity with a recognizable patho- striction of only one renal artery, in which case the patho- genesis. A family history of hypertensive disease is present logical changes of malignant hypertension, with their in a high proportion of cases of essential hypertension. -

Hypertension and the Prothrombotic State
Journal of Human Hypertension (2000) 14, 687–690 2000 Macmillan Publishers Ltd All rights reserved 0950-9240/00 $15.00 www.nature.com/jhh REVIEW ARTICLE Hypertension and the prothrombotic state GYH Lip Haemostasis Thrombosis and Vascular Biology Unit, University Department of Medicine, City Hospital, Birmingham, UK The basic underlying pathophysiological processes related to conventional risk factors, target organ dam- underlying the major complications of hypertension age, complications and long-term prognosis, as well as (that is, heart attacks and strokes) are thrombogenesis different antihypertensive treatments. Further work is and atherogenesis. Indeed, despite the blood vessels needed to examine the mechanisms leading to this being exposed to high pressures in hypertension, the phenomenon, the potential prognostic and treatment complications of hypertension are paradoxically throm- implications, and the possible value of measuring these botic in nature rather than haemorrhagic. The evidence parameters in routine clinical practice. suggests that hypertension appears to confer a Journal of Human Hypertension (2000) 14, 687–690 prothrombotic or hypercoagulable state, which can be Keywords: hypercoagulable; prothrombotic; coagulation; haemorheology; prognosis Introduction Indeed, patients with hypertension are well-recog- nised to demonstrate abnormalities of each of these Hypertension is well-recognised to be an important 1 components of Virchow’s triad, leading to a contributor to heart attacks and stroke. Further- prothrombotic or hypercoagulable state.4 Further- more, effective antihypertensive therapy reduces more, the processes of thrombogenesis and athero- strokes by 30–40%, and coronary artery disease by 2 genesis are intimately related, and many of the basic approximately 25%. Nevertheless the basic under- concepts thrombogenesis can be applied to athero- lying pathophysiological processes underlying both genesis. -
Dissecting Aneurysm of the Aorta
Cleveland Clinic Quarterly Volume 23 OCTOBER 1956 No. 4 DISSECTING ANEURYSM OF THE AORTA A Review ARTHUR L. SCHERBEL, M.D., Division of Medicine JOHN B. HAZARD, M.D., Department of Pathology and VICTOR G. DEWOLFE, M.D. Department of Cardiovascular Disease ISSECTING ANEURYSM OF THE AORTA is an intramural separation D of the aortic wall by circulating blood that has penetrated and extended into the media. The process may arrest at this stage and heal, progress im- mediately, or extend at some later date. As the dissecting aneurysm progresses, it may rupture through the adventitia into the pericardial, pleural, or abdominal cavities and may obstruct arteries arising from the aorta. It may rupture back into the lumen and form a double-barreled aorta, which may persist, or the aneurysm may be filled with clot and subsequently heal, obliterating the secondary channel. Etiology Although the specific cause of the disease is not known, the lesion that generally is accepted as being precedent to dissecting aneurysm of the aorta is 231 Downloaded from www.ccjm.org on September 26, 2021. For personal use only. All other uses require permission. SCHERBEL, HAZARD, AND DEWOLFE A Fig. 1. Changes in the media. (A) Medial degeneration (mucinous); hematoxylin, eosin and methylene blue stain, X80. (B) Marked loss of elastic tissue in a corresponding area; Verhoeff's stain, X80. 232 Cleveland Clinic Quarterly Downloaded from www.ccjm.org on September 26, 2021. For personal use only. All other uses require permission. DISSECTING ANEURYSM OF THE AORTA medial degeneration. This most often consists of mucoid changes in the media and focal loss of elastic tissue (Fig. -

The Clinical Significance of Systolic Hypertension
AJH 1998;11:182S–185S The Clinical Significance of Systolic Hypertension William C. Cushman Downloaded from https://academic.oup.com/ajh/article/11/S8/182S/151642 by guest on 28 September 2021 Large-scale epidemiologic studies and clinical trials Blood Pressure (JNC VI) recommends drug therapy have contributed to an increased recognition of the for all patients with stage 1 (140 to 159 mm Hg) or importance of systolic hypertension. Data from stage 2–3 (> 160 mm Hg) systolic hypertension, landmark epidemiologic studies such as the whether it occurs in isolation or in conjunction Multiple Risk Factor Intervention Trial screenee with diastolic hypertension. The sixth JNC report follow-up and the Framingham Heart Study have identified diuretics as the initial therapy of choice, demonstrated that elevated systolic blood pressure with a long-acting dihydropyridine calcium dramatically increases the risk of cardiovascular channel blocker as an alternative if diuretics are events. Of particular concern is the extremely high ineffective or not well tolerated. More research is risk associated with isolated systolic hypertension needed to evaluate other classes of drugs in this (ISH), which is much more common in the elderly setting. Regardless of the choice of therapy, than in young adults. Clinical trials have identified patients should be encouraged to adopt lifestyle significant risk reductions after treatment with modifications such as weight loss, exercise, sodium diuretics or the dihydropyridine calcium antagonist restriction, and reduced alcohol consumption. nitrendipine in older individuals with ISH. Beta Am J Hypertens 1998;11:182S–185S blockers have not been associated with such benefits. The recently released sixth report of the Joint National Committee on Prevention, KEY WORDS: Cardiovascular risk, systolic Detection, Evaluation, and Treatment of High hypertension. -

Hypertension and the Kidney
8.10 Hypertension and the Kidney SPECTRUM OF CLINICAL RENAL INVOLVEMENT IN MALIGNANT HYPERTENSION Progressive subacute deterioration of renal function to end-stage renal disease Transient deterioration of renal function with initial blood pressure control Oliguric acute renal failure Established renal failure FIGURE 8-17 Malignant hypertension is a progressive systemic vasculopathy in which renal involvement is a relatively late finding. In this regard, patients with malignant hypertension can present with a spectrum of renal involvement ranging from normal renal function with minimal FIGURE 8-16 (see Color Plate) albuminuria to end-stage renal disease (ESRD) indistinguishable Micrograph of proliferative endarteritis in malignant hypertension from that seen in primary renal parenchymal disease. In patients (musculomucoid intimal hyperplasia). In malignant nephrosclerosis, initially exhibiting preserved renal function, in the absence of adequate the interlobular (cortical radial) arteries reveal characteristic lesions. blood pressure control, it is common to observe subacute deterio- These lesions are variously referred to as proliferative endarteritis, ration of renal function to ESRD over a period of weeks to months. endarteritis fibrosa, musculomucoid intimal hyperplasia, or the Transient deterioration of renal function with initial control of onionskin lesion. The typical finding is marked thickening of the blood pressure is a well-documented entity in patients initially intima that obstructs the vessel lumen. In severely affected vessels exhibiting mild to moderate renal impairment. Occasionally, the luminal diameter may be reduced to the caliber of a single ery- patients with malignant hypertension initially exhibit oliguric acute throcyte. Occasionally, complete obliteration of the lumen by a renal failure, necessitating initiation of dialysis within a few days of superimposed fibrin thrombus occurs. -

The Burden of Pulmonary Hypertension in Resource-Limited Settings Suman Gidwani*, Ajith Nairy Durham, NC, USA; and New York, NY, USA
j STATE-OF-THE-ART REVIEW gREVIEW The Burden of Pulmonary Hypertension in Resource-Limited Settings Suman Gidwani*, Ajith Nairy Durham, NC, USA; and New York, NY, USA ABSTRACT Pulmonary vascular disease (PVD) is a significant global health problem and accounts for a substantial portion of cardiovascular disease in the developing world. Although there have been considerable advances in therapeutics for pulmonary arterial hypertension, over 97% of the disease burden lies within the developing world where there is limited access to health care and pharmaceuticals. The causes of pulmonary arterial hypertension differ between industrialized and developing nations. Infectious diseases—including schistosomiasis human immunodeficiency virus, and rheumatic fever—are common causes of PVD, as are hemoglobinopathies, and untreated congenital heart disease. High altitude and exposure to household air pollutants also contribute to a significant portion of PVD cases. Although diagnosis of pulmonary arterial hypertension requires the use of imaging and invasive hemodynamics, access to equipment may be limited. PVD therapies may be prohibitively expensive and limited to a select few. Prevention is therefore important in limiting the global PVD burden. Cardiovascular disease accounts for roughly 30% of 2); PH secondary to pulmonary disease (group 3); chronic deaths worldwide and is the leading cause of death globally thromboembolic PH (group 4); and PH from multifactorial [1]. Pulmonary vascular disease (PVD) accounts for a sub- etiologies (group 5) [5] (Table 1). PAH represents a subset stantial burden of cardiovascular disease in resource-limited of PVD that is characterized by pre-capillary PVD. The settings. PVD broadly refers to any disorder that may affect hemodynamic definition of PAH is a mean PA pressure the pulmonary blood circulation. -

The Study of Aortic Stiffness in Different Hypertension Subtypes in Dialysis Patients
593 Hypertens Res Vol.31 (2008) No.4 p.593-599 Original Article The Study of Aortic Stiffness in Different Hypertension Subtypes in Dialysis Patients Li-Tao CHENG1),2), Hui-Min CHEN1),3), Li-Jun TANG1),4), Wen TANG1), Hai-Yan HUANG2), Yue GU1), and Tao WANG1),2) The aim of this study was to validate whether differences in aortic stiffness are responsible for the differ- ences in cardiovascular mortality among hypertension subtypes. Twenty hundred and fifty continuous ambulatory peritoneal dialysis patients were included in the present study. They were classified into four groups: normotensives (n=92) with systolic blood pressure (SBP) <140 mmHg and diastolic blood pressure (DBP) <90 mmHg; isolated systolic hypertensives (ISH, n=84) with SBP ≥140 mmHg and DBP <90 mmHg; isolated diastolic hypertensives (IDH, n=21) with SBP <140 mmHg and DBP ≥90 mmHg; and systolic-dias- tolic hypertensives (SDH, n=53) with SBP ≥140 mmHg and DBP ≥90 mmHg. Aortic stiffness was assessed by pulse pressure, central pressure parameters and pulse wave velocity. The IDH group had more male patients and a lower mean age than the other groups. The percentage of diabetes in the ISH group was higher than that in the other groups. The comparisons of aortic stiffness showed that the ISH and SDH groups had higher aortic stiffness than the normotension and IDH groups. The aortic stiffness in the ISH group was also higher than that in the SDH group, but there was no significant difference in aortic stiffness between the normotension and IDH groups. In conclusion, this study showed that aortic stiffness was sig- nificantly different among different hypertension subtypes, which might be an underlying cause of the dif- ferences in cardiovascular mortality among the hypertension subtypes.