Incidence, Morbidity and Mortality of Patients with Achalasia in England: Findings from a Nationwide Hospital Database and 4 Million Population Based Data
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

High B1a0d Pressure and Its Treatment in General
HIGH B1A0D PRESSURE AND ITS TREATMENT IN GENERAL PRACTICE WITH PARTICULAR REFERENCE TO A SERIES OF 100 CASES TREATED BY THE AUTHOR By HAROLD WILSON B01YBR IB.ffh.B. ProQuest Number: 13849841 All rights reserved INFORMATION TO ALL USERS The quality of this reproduction is dependent upon the quality of the copy submitted. In the unlikely event that the author did not send a com plete manuscript and there are missing pages, these will be noted. Also, if material had to be removed, a note will indicate the deletion. uest ProQuest 13849841 Published by ProQuest LLC(2019). Copyright of the Dissertation is held by the Author. All rights reserved. This work is protected against unauthorized copying under Title 17, United States C ode Microform Edition © ProQuest LLC. ProQuest LLC. 789 East Eisenhower Parkway P.O. Box 1346 Ann Arbor, Ml 48106- 1346 -CONTENTS SECTION 1. Introduction. SECTION 2. General Remarks. Definitions of General Interest. Present Views on Etiology. Pathology and Morbid Anatomy. Brief Historical Survey. SECTION 3. The Present Position. Prevalence. Clinical Manifestations. Prognosis. SECTION 4. Prevalence in Bolton. Summary of Cases. Symptomatology and Case Histories Prognosis. Treatment. SECTION 5. Conclusions. Bibliography. SECTION 1. INTRODUCTION. I think it can truthfully be said that the most interest ing problems in Medioine are those that are most baffling. Some years ago Ralph M a j o r ^ wrote these words, ”If our knowledge of the etiology of arterial hypertension is shrouded in a oertain haze, our knowledge of an effective therapy in this disease is enveloped in a dense fog.n A study of some of the vast literature on this subject does not greatly clarify the obscurity. -

DISEASES of ARTERIES ARTERIOSCLEROSIS (“Hardening of the Arteries”): General Term Reflecting Arterial Wall Thickening and Loss of Elasticity
DISEASES OF ARTERIES ARTERIOSCLEROSIS (“hardening of the arteries”): general term reflecting arterial wall thickening and loss of elasticity 3 patterns •Atherosclerosis: involves the the aorta and the large arteries •Mönckeberg sclerosis: calcific deposits in the media of middle-sized arteries in persons >age 50 •Arteriolosclerosis: involves the small arteries and arterioles in association with hypertension or diabetes ATHEROSCLEROSIS Multifactorial, slowly progressive chronic degenerative-inflammatory disease of the aorta and the large arteries, such as • coronary arteries • circle of Willis • popliteal and tibial arteries Significance: > 50% of all death is attributed to atherosclerosis in well-developed countries Morphology Gross • Atheromatous plaque (pathognomic) - raised white-yellow lesion in the intima, protruding into the lumen • Large plaques in the aorta (> 2 cm) contain a yellow, grumous debris (”atheroma” - Greek word for gruel) Atheromatous plaque in the middle cerebral artery: raised white-yellow lesion in the intima, protruding into the lumen (formol-fixed brain) Aorta: the plaques contain a yellow, grumous debris (arrow) Structure of atheroma on LM • Intimal lesion • Central lipid core • Fibrous ”cap” subendothelially Central lipid core composed of lipids, cholesterol clefts, necrotic debris + calcium-salts, surrounded by foamy macrophages, T-lymphocytes, fibroblasts, small capillaries, and collagens and proteoglycans Types of plaques • Vulnerable plaques have large atheromatous cores, increased inflammatory cell content and thin fibrous caps high risk of rupture thrombosis • Stable plaques have minimal atheromatous cores and inflammation and thick fibrous caps 70% stenosis (critical stenosis) chronic ischemia distally Vulnerable plaque in the coronary artery Inflammatory infiltrates and capillaries around the lipid core. Lumen Intima Media Pathogenesis Response to chronic endocardial injury hypothesis • Cholesterol can’t dissolve in the blood. -
DSM III and ICD 9 Codes 11-2004
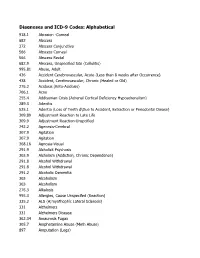
Diagnoses and ICD-9 Codes: Alphabetical 918.1 Abrasion -Corneal 682 Abscess 372 Abscess Conjunctiva 566 Abscess Corneal 566 Abscess Rectal 682.9 Abscess, Unspecified Site (Cellulitis) 995.81 Abuse, Adult 436 Accident Cerebrovascular, Acute (Less than 8 weeks after Occurrence) 438 Accident, Cerebrovascular, Chronic (Healed or Old) 276.2 Acidosis (Keto-Acidosis) 706.1 Acne 255.4 Addisonian Crisis (Adrenal Cortical Deficiency Hypoadrenalism) 289.3 Adenitis 525.1 Adentia (Loss of Teeth d\Due to Accident, Extraction or Periodontal Diease) 309.89 Adjustment Reaction to Late Life 309.9 Adjustment Reaction-Unspcified 742.2 Agenesis-Cerebral 307.9 Agitation 307.9 Agitation 368.16 Agnosia-Visual 291.9 Alcholick Psychosis 303.9 Alcholism (Addiction, Chronic Dependence) 291.8 Alcohol Withdrawal 291.8 Alcohol Withdrawal 291.2 Alcoholic Dementia 303 Alcoholism 303 Alcoholism 276.3 Alkalosis 995.3 Allergies, Cause Unspecifed (Reaction) 335.2 ALS (A;myothophic Lateral Sclerosis) 331 Alzheimers 331 Alzheimers Disease 362.34 Amaurosis Fugax 305.7 Amphetamine Abuse (Meth Abuse) 897 Amputation (Legs) 736.89 Amputation, Leg, Status Post (Above Knee, Below Knee) 736.9 Amputee, Site Unspecified (Acquired Deformity) 285.9 Anemia 284.9 Anemia Aplastic (Hypoplastic Bone Morrow) 280 Anemia Due to loss of Blood 281 Anemia Pernicious 280.9 Anemia, Iron Deficiency, Unspecified 285.9 Anemia, Unspecified (Normocytic, Not due to blood loss) 281.9 Anemia, Unspecified Deficiency (Macrocytic, Nutritional 441.5 Aneurysm Aortic, Ruptured 441.1 Aneurysm, Abdominal 441.3 Aneurysm, -

Human Anatomy As Related to Tumor Formation Book Four
SEER Program Self Instructional Manual for Cancer Registrars Human Anatomy as Related to Tumor Formation Book Four Second Edition U.S. DEPARTMENT OF HEALTH AND HUMAN SERVICES Public Health Service National Institutesof Health SEER PROGRAM SELF-INSTRUCTIONAL MANUAL FOR CANCER REGISTRARS Book 4 - Human Anatomy as Related to Tumor Formation Second Edition Prepared by: SEER Program Cancer Statistics Branch National Cancer Institute Editor in Chief: Evelyn M. Shambaugh, M.A., CTR Cancer Statistics Branch National Cancer Institute Assisted by Self-Instructional Manual Committee: Dr. Robert F. Ryan, Emeritus Professor of Surgery Tulane University School of Medicine New Orleans, Louisiana Mildred A. Weiss Los Angeles, California Mary A. Kruse Bethesda, Maryland Jean Cicero, ART, CTR Health Data Systems Professional Services Riverdale, Maryland Pat Kenny Medical Illustrator for Division of Research Services National Institutes of Health CONTENTS BOOK 4: HUMAN ANATOMY AS RELATED TO TUMOR FORMATION Page Section A--Objectives and Content of Book 4 ............................... 1 Section B--Terms Used to Indicate Body Location and Position .................. 5 Section C--The Integumentary System ..................................... 19 Section D--The Lymphatic System ....................................... 51 Section E--The Cardiovascular System ..................................... 97 Section F--The Respiratory System ....................................... 129 Section G--The Digestive System ......................................... 163 Section -

Guidance for the Format and Content of the Protocol of Non-Interventional
PASS information Title Metformin use in renal impairment Protocol version identifier Version 2 Date of last version of 30 October 2013 protocol EU PAS register number Study not registered Active substance A10BA02 metformin Medicinal product Metformin Product reference N/A Procedure number N/A Marketing authorisation 1A Farma, Actavis, Aurobindo, Biochemie, Bluefish, holder(s) Hexal, Mylan, Orifarm, Pfizer, Sandoz, Stada, Teva Joint PASS No Research question and To assess the use and safety of metformin in patients objectives with and without renal insufficiency in current clinical practice in at least two EU Member States. Country(-ies) of study Denmark, United Kingdom Author Christian Fynbo Christiansen, MD, PhD Page 1/214 Marketing authorisation holder(s) Marketing authorisation N/A holder(s) MAH contact person N/A Page 2/214 1. Table of Contents PASS information .......................................................................................................... 1 Marketing authorisation holder(s) .................................................................................... 2 1. Table of Contents ...................................................................................................... 3 2. List of abbreviations ................................................................................................... 4 3. Responsible parties .................................................................................................... 5 4. Abstract .................................................................................................................. -

IQI 17 Acute Stroke Mortality Rate
AHRQ Quality Indicators™ (AHRQ QI™) ICD-10-CM/PCS Specification v2021 Inpatient Quality Indicator 17 (IQI 17) Acute Stroke Mortality Rate July 2021 Hospital-Level Indicator Type of Score: Rate Prepared by: Agency for Healthcare Research and Quality U.S. Department of Health and Human Services www.qualityindicators.ahrq.gov DESCRIPTION In-hospital deaths per 1,000 hospital discharges with a principal diagnosis of acute stroke for patients ages 18 years and older. Includes metrics for discharges grouped by type of stroke. Excludes transfers to another hospital, cases admitted from a hospice facility, and obstetric discharges. [NOTE: The software provides the rate per hospital discharge. However, common practice reports the measure as per 1,000 discharges. The user must multiply the rate obtained from the software by 1,000 to report in-hospital deaths per 1,000 hospital discharges.] Stratification of Indicator The indicator is stratified into three groups by the type of stroke: Cases are assigned to strata according to a hierarchy based on risk of mortality, with cases being assigned to the stratum with the highest mortality for which the case qualifies. In the case of Stroke Mortality the current hierarchy is as follows: Strata hierarchy (listed from highest mortality to lowest mortality): 1) Intracerebral hemorrhage 2) Subarachnoid hemorrhage 3) Ischemic stroke Strata are mutually exclusive. If a discharge qualifies for more than one stratum, it will be assigned to the stratum with the highest risk of mortality (Intracerebral hemorrhage, Subarachnoid hemorrhage, Ischemic stroke). July 2021 1 of 7 AHRQ QI™ ICD-10-CM/PCS Specification v2021 IQI 17 Acute Stroke Mortality Rate www.qualityindicators.ahrq.gov NUMERATOR Overall Number of deaths (DISP=20) among cases meeting the inclusion and exclusion rules for the denominator. -

Technical Guidelines for Head and Neck Cancer IMRT on Behalf of the Italian Association of Radiation Oncology
Merlotti et al. Radiation Oncology (2014) 9:264 DOI 10.1186/s13014-014-0264-9 REVIEW Open Access Technical guidelines for head and neck cancer IMRT on behalf of the Italian association of radiation oncology - head and neck working group Anna Merlotti1†, Daniela Alterio2†, Riccardo Vigna-Taglianti3†, Alessandro Muraglia4†, Luciana Lastrucci5†, Roberto Manzo6†, Giuseppina Gambaro7†, Orietta Caspiani8†, Francesco Miccichè9†, Francesco Deodato10†, Stefano Pergolizzi11†, Pierfrancesco Franco12†, Renzo Corvò13†, Elvio G Russi3*† and Giuseppe Sanguineti14† Abstract Performing intensity-modulated radiotherapy (IMRT) on head and neck cancer patients (HNCPs) requires robust training and experience. Thus, in 2011, the Head and Neck Cancer Working Group (HNCWG) of the Italian Association of Radiation Oncology (AIRO) organized a study group with the aim to run a literature review to outline clinical practice recommendations, to suggest technical solutions and to advise target volumes and doses selection for head and neck cancer IMRT. The main purpose was therefore to standardize the technical approach of radiation oncologists in this context. The following paper describes the results of this working group. Volumes, techniques/strategies and dosage were summarized for each head-and-neck site and subsite according to international guidelines or after reaching a consensus in case of weak literature evidence. Introduction Material and methods Performing intensity-modulated radiotherapy (IMRT) The first participants (AM, DA, AM, LL, RM, GG, OC, in head and neck cancer patients (HNCPs) requires FM, FD and RC) were chosen on a voluntary basis training [1] and experience. For example, in the 02–02 among the HNCWG members. The group was coordi- Trans Tasman Radiation Oncology Group (TROG) nated by an expert head and neck radiation oncologist trial, comparing cisplatin (P) and radiotherapy (RT) (RC). -

ANATOMIC and PATHOLOGIC ASSESSMENT of FELINE LYMPH NODES USING COMPUTED TOMOGRAPHY and ULTRASONOGRAPHY Mauricio Tobón Restrepo
ADVERTIMENT. Lʼaccés als continguts dʼaquesta tesi queda condicionat a lʼacceptació de les condicions dʼús establertes per la següent llicència Creative Commons: http://cat.creativecommons.org/?page_id=184 ADVERTENCIA. El acceso a los contenidos de esta tesis queda condicionado a la aceptación de las condiciones de uso establecidas por la siguiente licencia Creative Commons: http://es.creativecommons.org/blog/licencias/ WARNING. The access to the contents of this doctoral thesis it is limited to the acceptance of the use conditions set by the following Creative Commons license: https://creativecommons.org/licenses/?lang=en Doctorand: Mauricio Tobón Restrepo Directores: Yvonne Espada Gerlach & Rosa Novellas Torroja Tesi Doctoral Barcelona, 29 de juliol de 2016 This thesis has received financial support from the Colombian government through the “Francisco José de Caldas” scholarship program of COLCIENCIAS and from the Corporación Universitaria Lasallista. DEDICATED TO A los que son la razón y la misión de esta tesis… LOS GATOS. A mis padres y hermanos. A Ismael. Vor mijn poffertje. ACKNOWLEDGMENTS Tal vez es la parte que se pensaría más fácil de escribir, pero sin duda se juntan muchos sentimientos al momento de mirar atrás y ver todo lo que has aprendido y todas las personas que han estado a tu lado dándote una palabra de aliento… y es ahí cuando se asoma la lágrima… Sin duda alguna, comienzo agradeciendo a los propietarios de todos los gatos incluidos en este estudio, sin ellos esto no habría sido posible. A continuación agradezco a mis directoras de tesis, la Dra. Rosa Novellas y la Dra. Yvonne Espada. Muchas gracias por creer en mí, por apoyarme y por tenerme tanta paciencia. -

M. H. RATZLAFF: the Superficial Lymphatic System of the Cat 151
M. H. RATZLAFF: The Superficial Lymphatic System of the Cat 151 Summary Four examples of severe chylous lymph effusions into serous cavities are reported. In each case there was an associated lymphocytopenia. This resembled and confirmed the findings noted in experimental lymph drainage from cannulated thoracic ducts in which the subject invariably devdops lymphocytopenia as the lymph is permitted to drain. Each of these patients had com munications between the lymph structures and the serous cavities. In two instances actual leakage of the lymphography contrrult material was demonstrated. The performance of repeated thoracenteses and paracenteses in the presenc~ of communications between the lymph structures and serous cavities added to the effect of converting the. situation to one similar to thoracic duct drainage .The progressive immaturity of the lymphocytes which was noted in two patients lead to the problem of differentiating them from malignant cells. The explanation lay in the known progressive immaturity of lymphocytes which appear when lymph drainage persists. Thankful acknowledgement is made for permission to study patients from the services of Drs. H. J. Carroll, ]. Croco, and H. Sporn. The graphs were prepared in the Department of Medical Illustration and Photography, Dowristate Medical Center, Mr. Saturnino Viloapaz, illustrator. References I Beebe, D. S., C. A. Hubay, L. Persky: Thoracic duct 4 Iverson, ]. G.: Phytohemagglutinin rcspon•e of re urctcral shunt: A method for dccrcasingi circulating circulating and nonrecirculating rat lymphocytes. Exp. lymphocytes. Surg. Forum 18 (1967), 541-543 Cell Res. 56 (1969), 219-223 2 Gesner, B. M., J. L. Gowans: The output of lympho 5 Tilney, N. -

Collaborative Stage Manual Part II
SEER Program Coding and Staging Manual 2004, Revision 1 Collaborative Staging Codes Nasal Cavity C30.0 C30.0 Nasal cavity (excludes nose, NOS C76.0) Note: Laterality must be coded for this site, except subsites Nasal cartilage and Nasal septum, for which laterality is coded 0. CS Tumor Size CS Site-Specific Factor 1 - Size of The following tables are available CS Extension Lymph Nodes at the collaborative staging CS TS/Ext-Eval CS Site-Specific Factor 2 - website: CS Lymph Nodes Extracapsular Extension, Lymph Nodes Histology Exclusion Table CS Reg Nodes Eval for Head and Neck AJCC Stage Reg LN Pos CS Site-Specific Factor 3 - Levels I- Lymph Nodes Size Table Reg LN Exam III, Lymph Nodes for Head and Neck CS Mets at DX CS Site-Specific Factor 4 - Levels IV- CS Mets Eval V and Retropharyngeal Lymph Nodes for Head and Neck CS Site-Specific Factor 5 - Levels VI- VII and Facial Lymph Nodes for Head and Neck CS Site-Specific Factor 6 - Parapharyngeal, Parotid, Preauricular, and Sub-Occipital Lymph Nodes, Lymph Nodes for Head and Neck Nasal Cavity CS Tumor Size SEE STANDARD TABLE Nasal Cavity CS Extension Code Description TNM SS77 SS2000 00 In situ; non-invasive Tis IS IS 10 Invasive tumor confined to site of origin T1 L L Meatus (superior, middle, inferior) Nasal chonchae (superior, middle, inferior) Septum Tympanic membrane 30 Localized, NOS T1 L L 40 Extending to adjacent connective tissue within the nasoethomoidal T2 RE RE complex Nasolacrimal duct 60 Adjacent organs/structures including: T3 RE RE Bone of skull Choana Frontal sinus Hard palate -

Tests Spring 2012
Tests spring 2013 Test 1 Oral cavity 1. Vestibulum oris does not communicate with proper oral cavity through: :r1 oral part of pharynx :r2 tremata :r3 space behind last molar :r4 space when tooth is missing :r5 communicates through all mentioned ways -- 2. Into vestibule of oral cavity opens out: :r1 caruncula sublingualis :r2 papilla parotidea :r3 ductus nasolacrimalis :r4 plica sublingualis :r5 none of mentioned answers is correct -- 3. The underlay of lips is: :r1 m. labialis :r2 m. orbicularis oculi :r3 m. orbicularis oris :r4 m. buccalis :r5 none of mentioned answers is correct -- 4. The upper lip is partially connected with alveolar process using: :r1 lig. labii superioris :r2 m. platysma :r3 frenulum labii superioris :r4 plica labii superioris :r5 none of mentioned answers is correct -- 5. Cheek is not made up of: :r1 skin :r2 adipose body :r3 muscular layer :r4 adventitia :r5 none of mentioned answers is correct -- 6. Parotid duct passes through: :r1 m. masseter :r2 m. buccinator :r3 m. orbicularis oris :r4 m. pterygoideus lateralis :r5 none of mentioned answers is correct -- 7. The underlay of hard palate is not: :r1 praemaxilla :r2 vomer :r3 processus palatinus maxillae :r4 lamina horizontalis ossis palatini :r5 all mentioned bones form the underlay of hard palate -- 8. Which statement describing mucosa of hard palate is not correct: :r1 it contains big amount of submucosal connective tissue :r2 it is covered by columnar epithelium :r3 firmly grows together with periosteum :r4 it is almost not movable against the bottom :r5 it contains glandulae palatinae -- 9. Mark the true statement describing the palate: :r1 there is papilla incisiva positioned there :r2 mucosa contains glandulae palatinae :r3 there are plicae palatinae transversae positioned there :r4 the basis of soft palate is made by fibrous aponeurosis palatina :r5 all mentioned statements are correct -- 10. -

Fig. 2-32 Facial Muscles. Fig. 2-33 Trigeminal Nerve (CN V)
Fig. 2-32 Facial Muscles. Fig. 2-33 Trigeminal Nerve (CN V) leaving the Skull. 51 thetic agent at the infraorbital foramen or in the infraor- posterior to its head and anterior to the auricle. It then bital canal (e.g., for treatment of wounds of the upper crosses over the root of the zygomatic process of the lip and cheek or for repairing the maxillary incisor teeth). temporal bone, deep to the superficial temporal artery. The site of emergence of this nerve can easily be deter- As its name suggests, it supplies parts of the auricle, mined by exerting pressure on the maxilla in the region external acoustic meatus, tympanic membrane (ear- of the infraorbital foramen and nerve. Pressure on the drum), and skin in the temporal region. The inferior al- nerve causes considerable pain. Care is exercised when veolar nerve is the large terminal branch of the posterior performing an infraorbital nerve block because compan- division of CN V3; the lingual nerve is the other terminal ion infraorbital vessels leave the infraorbital foramen with branch. It enters the mandibular canal through the man- the nerve. Careful aspiration of the syringe during injec- dibular foramen. In the canal it gives off branches that tion prevents inadvertent injection of the anesthetic fluid supply the mandibular (lower) teeth. Opposite the mental into a blood vessel. The orbit is located just superior to foramen, the inferior alveolar nerve divides into its ter- the injection site. A careless injection could result in minal incisive and mental branches. The incisive nerve the passage of anesthetic fluid into the orbit, causing supplies the incisor teeth, the adjacent gingiva, and temporary paralysis of the extraocular muscles.