12 IJBMRF20131339 Dr Sindhoori Komma
Total Page:16
File Type:pdf, Size:1020Kb
Load more
Recommended publications
-

An Institutional Experience
Original Research Article Skin Adnexal Tumors- An Institutional Experience 1 2* 3 4 5 6 Rekha M Haravi , Roopa K N , Priya Patil , Rujuta Datar , Meena N Jadhav , Shreekant K Kittur 1,5Associate Professor, 2Post Graduate Student, 3,4Assistant Professor, 6Professor & HOD, Department of Pathology, Belgaum Institute of Medical Sciences Dr B R Ambedkar Road, Belagavi, Karnataka – 590001, INDIA. Email: [email protected] Abstract Background: Skin adnexal tumors are a wide spectrum of benign and malignant tumors that differentiate towards one or more adnexal structures found in normal skin. The adnexal structures of skin are the hair follicles, sebaceous glands, eccrine and apocrine sweat glands. These skin adnexal tumors are often difficult to diagnose clinically. This retrospective study was undertaken to know the various histomorphological patterns of skin adnexal tumors at our institution and to determine the incidence among the genders and age groups along with the site distribution. Materials and methods: A total of 40 specimens received and diagnosed as skin adnexal tumors in the department of Pathology at Belgaum Institute of Medical Sciences, Belagavi for a period of 6 years from January 2014 to December 2019 were taken for the study. Histopathological slides prepared from tissue blocks retrieved from departmental archives were reviewed and classified according to the WHO classification 2017. Results: Out of the total 40 samples, benign tumors were 36 (90%) and malignant were 4 (10%). Largest group was the benign tumors of apocrine and eccrine differentiation (47.5%) followed by benign tumors of hair follicle differentiation (40%). Malignant tumors of sebaceous differentiation were 5%, malignant tumors of eccrine and apocrine differentiation were 2.5% and malignant hair follicle differentiation tumors were 2.5% of the total. -

Inherited Skin Tumour Syndromes
CME GENETICS Clinical Medicine 2017 Vol 17, No 6: 562–7 I n h e r i t e d s k i n t u m o u r s y n d r o m e s A u t h o r s : S a r a h B r o w n , A P a u l B r e n n a n B a n d N e i l R a j a n C This article provides an overview of selected genetic skin con- and upper trunk. 1,2 These lesions are fibrofolliculomas, ditions where multiple inherited cutaneous tumours are a cen- trichodiscomas and acrochordons. Patients are also susceptible tral feature. Skin tumours that arise from skin structures such to the development of renal cell carcinoma, lung cysts and as hair, sweat glands and sebaceous glands are called skin pneumothoraces. 3 appendage tumours. These tumours are uncommon, but can Fibrofolliculomas and trichodiscomas clinically present as ABSTRACT have important implications for patient care. Certain appenda- skin/yellow-white coloured dome shaped papules 2–4 mm in geal tumours, particularly when multiple lesions are seen, may diameter (Fig 1 a and Fig 1 b). 4 These lesions usually develop indicate an underlying genetic condition. These tumours may in the third or fourth decade.4 In the case of fibrofolliculoma, not display clinical features that allow a secure diagnosis to be hair specific differentiation is seen, whereas in the case of made, necessitating biopsy and dermatopathological assess- trichodiscoma, differentiation is to the mesodermal component ment. -

The Best Diagnosis Is: H&E, Original Magnification 2
Dermatopathology Diagnosis The best diagnosis is: H&E, original magnification 2. a. adenoid cysticcopy carcinoma arising within a spiradenoma b. cylindroma and spiradenoma collision tumor c. microcysticnot change within a spiradenoma d. mucinous carcinoma arising within a spiradenoma Doe. trichoepithelioma and spiradenoma collision tumor CUTIS H&E, original magnification 100. PLEASE TURN TO PAGE 211 FOR DERMATOPATHOLOGY DIAGNOSIS DISCUSSION Amanda F. Marsch, MD; Jeffrey B. Shackelton, MD; Dirk M. Elston, MD Dr. Marsch is from the Department of Dermatology, University of Illinois at Chicago. Drs. Shackelton and Elston are from the Ackerman Academy of Dermatopathology, New York, New York. The authors report no conflict of interest. Correspondence: Amanda F. Marsch, MD, University of Illinois at Chicago, 808 S Wood St, Chicago, IL 60612 ([email protected]). 192 CUTIS® WWW.CUTIS.COM Copyright Cutis 2015. No part of this publication may be reproduced, stored, or transmitted without the prior written permission of the Publisher. Dermatopathology Diagnosis Discussion Trichoepithelioma and Spiradenoma Collision Tumor he coexistence of more than one cutaneous adnexal neoplasm in a single biopsy specimen Tis unusual and is most frequently recognized in the context of a nevus sebaceous or Brooke-Spiegler syndrome, an autosomal-dominant inherited disease characterized by cutaneous adnexal neoplasms, most commonly cylindromas and trichoepitheliomas.1-3 Brooke-Spiegler syndrome is caused by germline muta- tions in the cylindromatosis gene, CYLD, located on band 16q12; it functions as a tumor suppressor gene and has regulatory roles in development, immunity, and inflammation.1 Weyers et al3 first recognized the tendency for adnexal collision tumors to present in patients with Brooke-Spiegler syndrome; they reported a patient with Brooke-Spiegler syndrome with spirad- Figure 1. -

Rippled-Pattern Sebaceoma: a Report of a Lesion on the Back with a Review of the Literature
View metadata, citation and similar papers at core.ac.uk brought to you by CORE provided by University of Fukui Repository Rippled-pattern sebaceoma: A report of a lesion on the back with a review of the literature Takahiro Kiyohara, M.D., Masanobu Kumakiri, M.D., Hiroaki Kuwahara, M.D., Atsuko Saitoh, M.D., and Shinichi Ansai, M.D. Department of Dermatology (T.K., M.K.), University of Fukui, Fukui; Division of Plastic Surgery (H.K.), Obihiro-Kousei General Hospital, Obihiro: Sapporo Institute for Dermatopathology (S.A.), Sapporo, Japan Address correspondence and reprint requests to: Takahiro Kiyohara, M.D. Department of Dermatology, University of Fukui 23-3 Shimoaizuki, Matsuoka-cho, Yoshida-gun, Fukui 910-1193, Japan Tel: +81 776 61 3111 Fax: +81 776 61 8112 e-mail: kiyo @ fmsrsa.fukui-med.ac.jp Abstract A 68-year-old Japanese man presented with a tumor that had been present for 5 to 6 years on the right back. Physical examination revealed a dome-shaped, 12x13-mm, dark red tumor. The tumor was excised with a 2 to 3-mm margin. The patient has remained free of disease during 77-months of follow-up. Microscopic examination revealed a bulb-like tumor in the dermis, contiguous with the overlying epidermis. It was composed of small, monomorphous, cigar-shaped basaloid cells in linear, parallel rows, resembling the palisading of nuclei of Verocay bodies, and presenting a rippled-pattern. There were scattered cells showing sebaceous differentiation with vacuolated cytoplasm and scalloped nuclei. There were tiny, duct-like spaces. The tumor revealed characteristics of rippled-pattern sebaceoma. -

Genetics of Skin Appendage Neoplasms and Related Syndromes
811 J Med Genet: first published as 10.1136/jmg.2004.025577 on 4 November 2005. Downloaded from REVIEW Genetics of skin appendage neoplasms and related syndromes D A Lee, M E Grossman, P Schneiderman, J T Celebi ............................................................................................................................... J Med Genet 2005;42:811–819. doi: 10.1136/jmg.2004.025577 In the past decade the molecular basis of many inherited tumours in various organ systems such as the breast, thyroid, and endometrium.2 syndromes has been unravelled. This article reviews the clinical and genetic aspects of inherited syndromes that are Clinical features of Cowden syndrome characterised by skin appendage neoplasms, including The cutaneous findings of Cowden syndrome Cowden syndrome, Birt–Hogg–Dube syndrome, naevoid include trichilemmomas, oral papillomas, and acral and palmoplantar keratoses. The cutaneous basal cell carcinoma syndrome, generalised basaloid hallmark of the disease is multiple trichilemmo- follicular hamartoma syndrome, Bazex syndrome, Brooke– mas which present clinically as rough hyperker- Spiegler syndrome, familial cylindromatosis, multiple atotic papules typically localised on the face (nasolabial folds, nose, upper lip, forehead, ears3 familial trichoepitheliomas, and Muir–Torre syndrome. (fig 1A, 1C, 1D). Trichilemmomas are benign ........................................................................... skin appendage tumours or hamartomas that show differentiation towards the hair follicles kin consists of both epidermal and dermal (specifically for the infundibulum of the hair 4 components. The epidermis is a stratified follicle). Oral papillomas clinically give the lips, Ssquamous epithelium that rests on top of a gingiva, and tongue a ‘‘cobblestone’’ appearance basement membrane, which separates it and its and histopathologically show features of 3 appendages from the underlying mesenchymally fibroma. The mucocutaneous manifestations of derived dermis. -
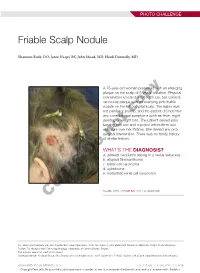
Friable Scalp Nodule
PHOTO CHALLENGE Friable Scalp Nodule Shannon Buck, DO; Jaree Naqvi, BS; John Moad, MD; Heidi Donnelly, MD A 75-year-old woman presented with an enlarging plaque on the scalp of 5 years’ duration. Physical examination revealed a 5.6×2.9-cm, tan-colored, verrucous plaque with an overlying pink friable nodule on the left occipital scalp. The lesion was not painful or pruritic,copy and the patient did not have any constitutional symptoms such as fever, night sweats, or weight loss. The patient denied prior tanning bed use and reported intermittent sun exposure over her lifetime. She denied any prior surgicalnot intervention. There was no family history of similar lesions. WHAT’S THE DIAGNOSIS? Doa. adnexal neoplasm arising in a nevus sebaceus b. atypical fibroxanthoma c. basal cell carcinoma d. cylindroma e. metastatic renal cell carcinoma CUTIS PLEASE TURN TO PAGE E20 FOR THE DIAGNOSIS Drs. Buck and Donnelly are from Dayton Skin Care Specialists, Ohio. Mr. Naqvi is from Boonshoft School of Medicine, Wright State University, Dayton. Dr. Moad is from Dermatopathology Laboratory of Central States, Dayton. The authors report no conflict of interest. Correspondence: Shannon Buck, DO, Dayton Skin Care Specialists, 3025 Governor’s Pl Blvd, Dayton, OH 45409 ([email protected]). WWW.MDEDGE.COM/DERMATOLOGY VOL. 105 NO. 1 I JANUARY 2020 E19 Copyright Cutis 2020. No part of this publication may be reproduced, stored, or transmitted without the prior written permission of the Publisher. PHOTO CHALLENGE DISCUSSION THE DIAGNOSIS: Adnexal Neoplasm Arising in a Nevus Sebaceus iopsy of the lesion showed a proliferation of basa- secondary neoplasms, 88% of which were benign.2 The loid-appearing cells with focal ductal differentiation origins of these neoplasms can be epithelial, sebaceous, Band ulceration consistent with poroma (Figure 1). -

Current Diagnosis and Treatment Options for Cutaneous Adnexal Neoplasms with Apocrine and Eccrine Differentiation
International Journal of Molecular Sciences Review Current Diagnosis and Treatment Options for Cutaneous Adnexal Neoplasms with Apocrine and Eccrine Differentiation Iga Płachta 1,2,† , Marcin Kleibert 1,2,† , Anna M. Czarnecka 1,* , Mateusz Spałek 1 , Anna Szumera-Cie´ckiewicz 3,4 and Piotr Rutkowski 1 1 Department of Soft Tissue/Bone Sarcoma and Melanoma, Maria Sklodowska-Curie National Research Institute of Oncology, 02-781 Warsaw, Poland; [email protected] (I.P.); [email protected] (M.K.); [email protected] (M.S.); [email protected] (P.R.) 2 Faculty of Medicine, Medical University of Warsaw, 02-091 Warsaw, Poland 3 Department of Pathology and Laboratory Diagnostics, Maria Sklodowska-Curie National Research Institute of Oncology, 02-781 Warsaw, Poland; [email protected] 4 Department of Diagnostic Hematology, Institute of Hematology and Transfusion Medicine, 00-791 Warsaw, Poland * Correspondence: [email protected] or [email protected] † Equally contributed to the work. Abstract: Adnexal tumors of the skin are a rare group of benign and malignant neoplasms that exhibit morphological differentiation toward one or more of the adnexal epithelium types present in normal skin. Tumors deriving from apocrine or eccrine glands are highly heterogeneous and represent various histological entities. Macroscopic and dermatoscopic features of these tumors are unspecific; therefore, a specialized pathological examination is required to correctly diagnose patients. Limited Citation: Płachta, I.; Kleibert, M.; treatment guidelines of adnexal tumor cases are available; thus, therapy is still challenging. Patients Czarnecka, A.M.; Spałek, M.; should be referred to high-volume skin cancer centers to receive an appropriate multidisciplinary Szumera-Cie´ckiewicz,A.; Rutkowski, treatment, affecting their outcome. -

Report of Three Novel Germline CYLD Mutations in Unrelated Patients
Zurich Open Repository and Archive University of Zurich Main Library Strickhofstrasse 39 CH-8057 Zurich www.zora.uzh.ch Year: 2016 Report of three novel germline CYLD mutations in unrelated patients with Brooke-Spiegler syndrome, including classic phenotype, multiple familial trichoepitheliomas and malignant transformation Tantcheva-Poór, Iliana ; Vanecek, Tomas ; Lurati, Massimo C R ; Rychly, Boris ; Kempf, Werner ; Michal, Michal ; Kazakov, Dmitry V Abstract: Brooke-Spiegler syndrome is a rare autosomal-dominant genetic disorder characterized by multiple adnexal tumors, including cylindromas, spiradenomas, spiradenocylindromas and trichoepithe- liomas. It is caused by germline CYLD mutations commonly leading to a premature stop codon. We here report on 3 novel CYLD mutations in 3 unrelated BSS patients, including the classic phenotype, mul- tiple familial trichoepitheliomas phenotype and malignant transformation. These included c.18211826 + 1delinsCT/L607Ffs∗9, c.2666A > T/p.D889V andc.2712delT/p.905Kfs∗8.ByextendingthespectrumofCY LDmutations, DOI: https://doi.org/10.1159/000437303 Posted at the Zurich Open Repository and Archive, University of Zurich ZORA URL: https://doi.org/10.5167/uzh-115928 Journal Article Published Version Originally published at: Tantcheva-Poór, Iliana; Vanecek, Tomas; Lurati, Massimo C R; Rychly, Boris; Kempf, Werner; Michal, Michal; Kazakov, Dmitry V (2016). Report of three novel germline CYLD mutations in unrelated patients with Brooke-Spiegler syndrome, including classic phenotype, multiple familial trichoepitheliomas and malignant transformation. Dermatology, 232(1):30-37. DOI: https://doi.org/10.1159/000437303 Original Paper Dermatology 2016;232:30–37 Received: March 13, 2015 DOI: 10.1159/000437303 Accepted after revision: June 13, 2015 Published online: September 2, 2015 Report of Three Novel Germline CYLD Mutations in Unrelated Patients with Brooke-Spiegler Syndrome, Including Classic Phenotype, Multiple Familial Trichoepitheliomas and Malignant Transformation a b, c d f Iliana Tantcheva-Poór Tomas Vanecek Massimo C.R. -

Multiple Familial Trichoepithelioma Caused by Mutations in the Cylindromatosis Tumor Suppressor Gene
[CANCER RESEARCH 64, 5113–5117, August 1, 2004] Multiple Familial Trichoepithelioma Caused by Mutations in the Cylindromatosis Tumor Suppressor Gene Aicha Salhi,1 Dorothea Bornholdt,2 Frank Oeffner,2 Sajid Malik,2 Ernest Heid,4 Rudolf Happle,3 and Karl-Heinz Grzeschik2 1Department of Dermatology, University of Algiers, Algiers, Algeria; Departments of 2Human Genetics and 3Dermatology, Philipp University, Marburg, Germany; and 4Department of Dermatology, Universite´Louis Pasteur, Strasbourg, France ABSTRACT In some MFT tumors, structures reminiscent of basal cell carci- noma (BCC) may be found (14), although MFT clearly differs from The recessive oncogene cylindromatosis (CYLD) mapping on 16q12-q13 Gorlin syndrome (multiple nevoid BCC syndrome) that is caused by is generally implicated in familial cylindromatosis, whereas a gene region mutations in the patched gene (PTCH1) on 9q22.3. In half of a series for multiple familial trichoepithelioma has been assigned to 9p21. Mark- ers from both chromosome intervals were subjected to linkage analysis in of sporadic TEs loss of heterozygosity (LOH) at 9q22.3, the region a large family with multiple hereditary trichoepithelioma (TE) from where PTCH1 maps was detected by Matt et al. (15) who postulated Algeria. Linkage to 9p21 was excluded, whereas CYLD remained as a a common gatekeeper mechanism for both TE and BCC. Their ob- candidate. Mutation analysis identified a single bp germ-line deletion servations corroborate a previous report that sporadic TE contain expected to result in truncation or absence of the encoded protein, which somatic mutations in the overexpressed PTCH gene, suggesting that a segregated with the multiple TE phenotype. In individual tumors, loss of failure in the negative feedback mechanism in the sonic hedgehog- heterozygosity at 16q or a somatic point mutation in the CYLD gene was patched (SHH-PTC) signaling pathway may be an early and necessary detected. -

Proliferating Trichilemmal Cyst with Lymphadenopathy: a Discussion of Cutaneous Neoplasms Involving the Scalp
Central Journal of Ear, Nose and Throat Disorders Bringing Excellence in Open Access Case Study *Corresponding author James Paul Dworkin-Valenti, Department of Otolaryngology, Head & Neck Surgery, Detroit Medical Proliferating Trichilemmal Center, 5807 Cedar Ridge Dr, Ann Arbor, MI 48103, USA, Tel: 313-966-9406; 248-444-7396; Email: Cyst with Lymphadenopathy: Submitted: 22 April 2016 Accepted: 29 April 2016 A Discussion of Cutaneous Published: 02 May 2016 Copyright Neoplasms Involving the Scalp © 2016 Valenti et al. OPEN ACCESS Richard T. Klapchar1, Billie Jean Crigger2 and James Paul Dworkin-Valenti3* 1Department of Otolaryngology, Head & Neck Surgery, Doctors Hospital, USA 2Private Practice, Owensboro, USA 3Department of Otolaryngology, Head & Neck Surgery, Detroit Medical Center, USA Abstract This paper introduces a unique case example of a trichilemmal scalp cyst that was initially erroneously diagnosed as a cancerous lesion because of its proliferating cellular morphology. The evaluation and treatment histories of this patient are augmented by a detailed review of the literature on this condition, especially with respect to cases of rare malignant transformation to squamous cell carcinoma. Whereas proliferating pilar or trichilemmal cysts are uncommon tumors that rarely undergo malignant transformation [1]. Squamous cell carcinomas with metastasis to regional head and neck lymph nodes rarely develop from proliferating pilar cysts. However, such degeneration has been reported in the literature [2]. These lesions are fraught with significant morbidity and mortality, and their treatment usually consists of substantial surgical excision. Histopathologic evidence of malignancy often demands adjuvant regimens of radiation therapy (+/-chemotherapy) [3]. The purpose of this case report is to present a patient with an ulcerative, necrotic scalp mass and lymphadenopathy whose initial biopsy demonstrated squamous cell carcinoma. -

Cytological Diagnosis of Cylindroma Scalp- a Rare Case Report Dr
Saudi Journal of Pathology and Microbiology Abbreviated Key Title: Saudi J Pathol Microbiol ISSN 2518-3362 (Print) |ISSN 2518-3370 (Online) Scholars Middle East Publishers, Dubai, United Arab Emirates Journal homepage: https://saudijournals.com/sjpm Case Report Cytological Diagnosis of Cylindroma Scalp- A Rare Case Report 1*, 2 3 4 Dr. Sabina Khan Dr. Sayika Hameed , Dr. Nehal Ahmad MD , Dr. Rubeena Mohroo MD , Dr. Mohd. Jaseem Hassan 5 6 MD , Prof. Sujata Jetley MD 1,5Associate Professor, Department of Pathology, Hamdard Institute of Medical Sciences and Research, Jamia Hamdard New Delhi 110062, India 22nd year post graduate, Pathology, Hamdard Institute of Medical Sciences and Research, Jamia Hamdard New Delhi 110062, India 3Assistant Professor Pathology, Hamdard Institute of Medical Sciences and Research, Jamia Hamdard New Delhi 110062, India 4Demonstrator Pathology, Hamdard Institute of Medical Sciences and Research, Jamia Hamdard New Delhi 110062, India 6Professor and Head Pathology, Hamdard Institute of Medical Sciences and Research, Jamia Hamdard New Delhi 110062, India DOI: 10.36348/sjpm.2020.v05i05.009 | Received: 07.05.2020 | Accepted: 14.05.2020 | Published: 21.05.2020 *Corresponding author: Dr. Sabina Khan Abstract Cylindromas are rare slow growing benign skin appendageal tumors with eccrine and apocrine differentiation. Multiple cylindromas are commonly genetically inherited and also known as “turban tumor.” Here, we have discussed a case of scalp swelling in a male patient having lung cancer, which was clinically suspicious of metastasis. However, cytology revealed many clusters of small round to oval basaloid cells surrounded and attached with magenta coloured acellular hyaline material. The cells had very scanty cytoplasm and dark, round to oval hyperchromatic nuclei without any nuclear membrane irregularity. -

Clear Cell Hidradenoma/Hidradenocarcinoma
UPDATE ON MALIGNANT ADNEXAL NEOPLASMS David S. Cassarino, M.D., Ph.D. Los Angeles Medical Center, Southern California Permanente Medical Group, Department of Pathology University of California, Irvine, Department of Dermatology CLASSIFICATION OF ADNEXAL TUMORS • Older classifications based on questionable morphologic and histochemical observations - Most of these are not specific for apocrine vs. eccrine diff’nt • Many tumors designated as eccrine or apocrine have features of the other category or features of adnexal ducts - Ducts of apocrine and eccrine nature show similar features and are essentially indistinguishable • Benign versus malignant determination is crucial for treatment and prognosis • Features such as asymmetry, infiltrative borders, increased mitoses, and necrosis favor malignancy • Atypical adnexal tumors show some, but not all, of these features • In many cases, due to limited sampling of the tumor (i.e., shave or punch biopsy), a definitive classification is not possible ◼ Such cases should be signed out descriptively, with a differential diagnosis, and complete excision recommended to obtain a definitive diagnosis • Newer immunohistochemical and molecular findings associated with particular tumors: • SOX10 in apocrine and some eccrine tumors • GATA3 in follicular, sebaceous, and apocrine tumors • MYB in adenoid cystic carcinoma, apocrine tumors • Beta-catenin overexpression in pilomatrical tumors • FXIIIa (nuclear) in sebaceous tumors • CYLD mutations in cylindroma, spiradenoma, trichoblastomas, and adenoid cystic carcinoma • HRAS, p53, RB1, APC, CDKN2A, and PTEN mutations in porocarcinoma • t(11;19) translocation in hidradenomas and hidradenocarcinomas • ETV6-NTRK3 translocation in primary cutaneous mammary analog secretory carcinoma CD117 and SOX-10 had similar overall positivity rates in benign apocrine and eccrine tumors (45% and 68% respectively), and were generally negative in other benign and malignant adnexal tumors.